Article Text

Abstract
Introduction Non Cystic Fibrosis (CF) Bronchiectasis is increasingly recognised as a major cause of respiratory morbidity in the UK. Previous BTS audits have shown poor adherence to the 2010 BTS guidelines for non-CF bronchiectasis. Specialist clinics for cystic fibrosis have been shown to improve survival and quality of life in CF bronchiectasis. The majority of patients with non-CF bronchiectasis are managed in general respiratory clinics. We hypothesised that the introduction of a specialist clinic for non-CF bronchiectasis would improve compliance with the BTS 2012 standards of care for non-CF bronchiectasis.
Methods Data was collected prospectively as part of the BTS national bronchiectasis audit 2012. All patients with bronchiectasis attending an outpatient respiratory clinic in Imperial NHS Trust between 1/10/12 to 31/11/12 were eligible for inclusion. Comparison between groups was performed using fischers exact test using GraphPad Prism software.
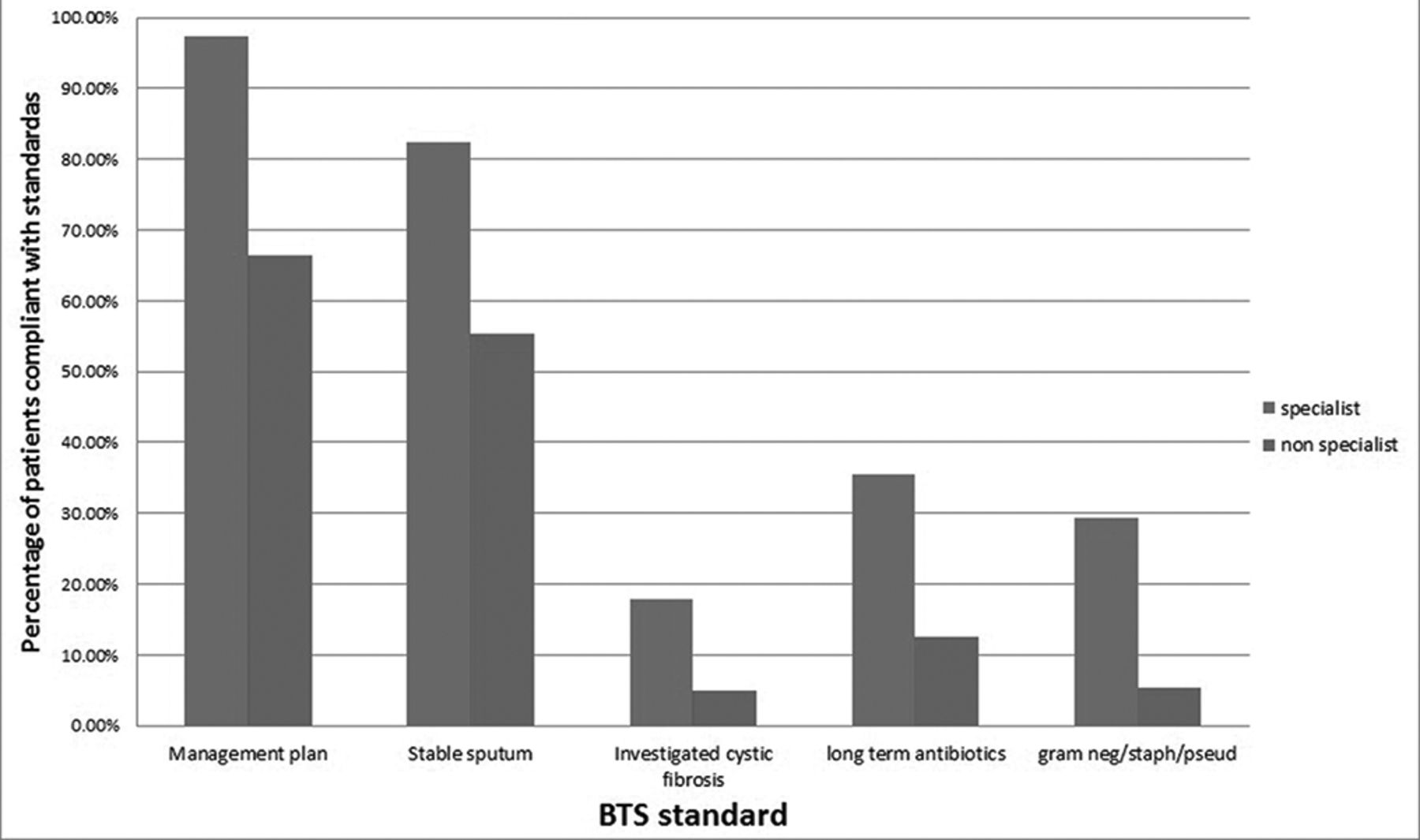
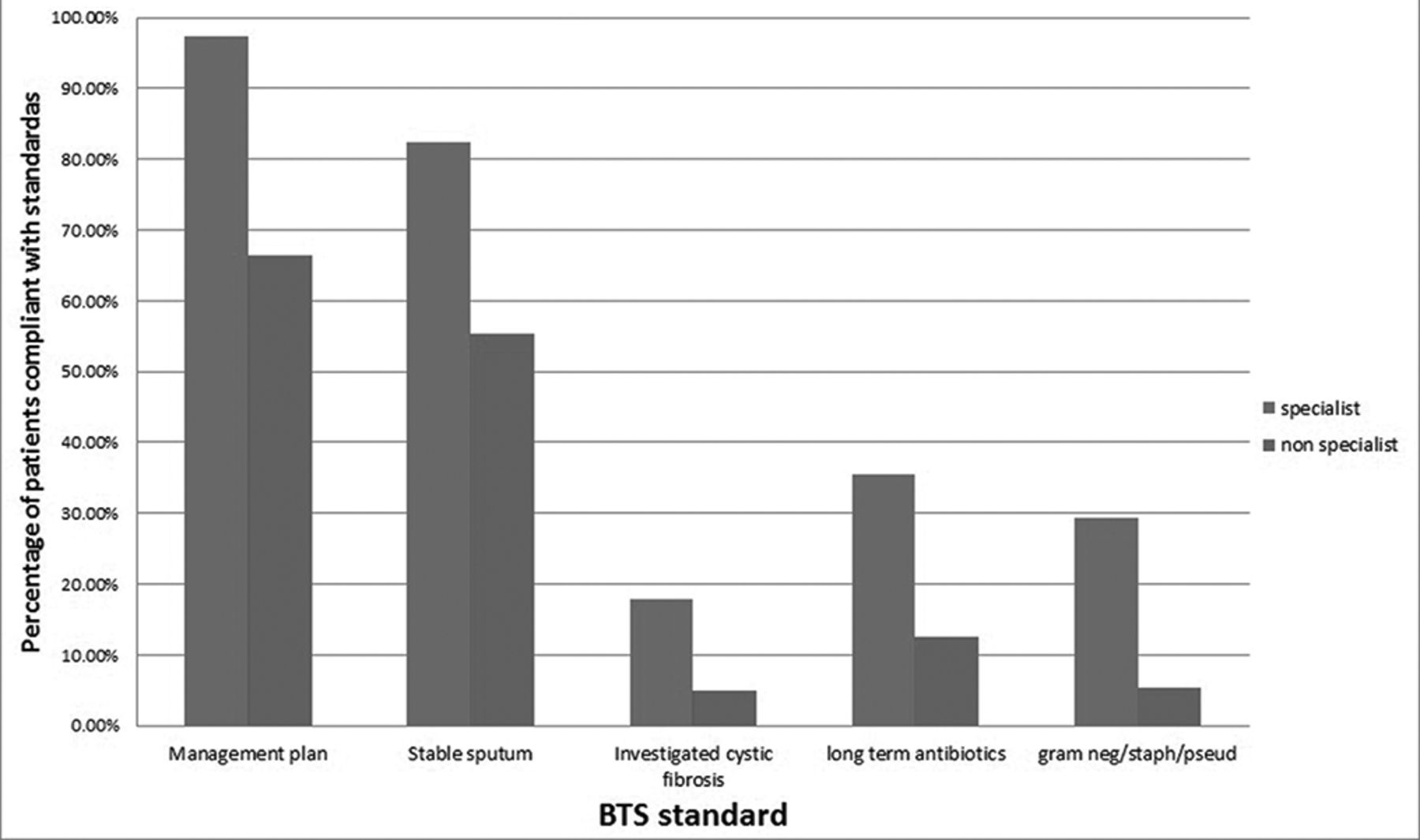
Results Forty patients attended a specialist bronchiectasis clinic, 56 patients were reviewed in a general respiratory clinic. Patients under the care of a bronchiectasis specialist were significantly more likely to have an individualised management plan (97.4% vs. 66.0% p = 0.002), to have their sputum sent for culture when clinically stable (82.5% vs. 55.4% p = 0.0018), and be investigated for cystic fibrosis (17.9% vs. 4.9% p = 0.007). They were significantly more likely to have grown a pseudomonas, staph aureus or a gram negative bacteria in their sputum in the last 12 months (29.4% vs. 5.4%, p = 0.0036) and be treated with either oral or nebulised long term antibiotics (35.0% vs. 12.5%, p = 0.012) graph 1.
Conclusions Patients attending specialist bronchiectasis clinics were more likely to be managed according to BTS quality standards. Specialist non-CF bronchiectasis clinics may improve quality of care. Further longitudinal studies are needed to investigate if specialist clinics improve clinical outcomes.
{kind=link}
Comparison between specialist and non specialist clinics for management of bronchiectasis