Article Text

Statistics from Altmetric.com
A 74-year-old Asian female underwent a chest CT scan because of a pulmonary nodule observed on her chest radiograph (figure 1A). She complained of mild dyspnoea on exertion for few weeks. Her past history was significant for hypertension and obesity (body mass index 39 kg/m2). Physical examination, electrocardiography (EKG), cardiac echogram and laboratory biochemistry were all unremarkable. Chest CT scan revealed a 3.6×2.8 cm solitary nodule locating at the tip of the lingual lobe with strong vascular enhancement demonstrated during contrast phase (figure 1B). The patient was afebrile and mildly anxious, and her blood pressure was 118/64 mm Hg. Since she was symptomatic without surgical contraindication, video-assisted thoracic surgery (VATS) exploration was proceeded. Under VATS, a bright-red and well-circumscribed cystic lesion at the tip of the lingual lobe was noted (figure 2), and a wedge resection was performed.
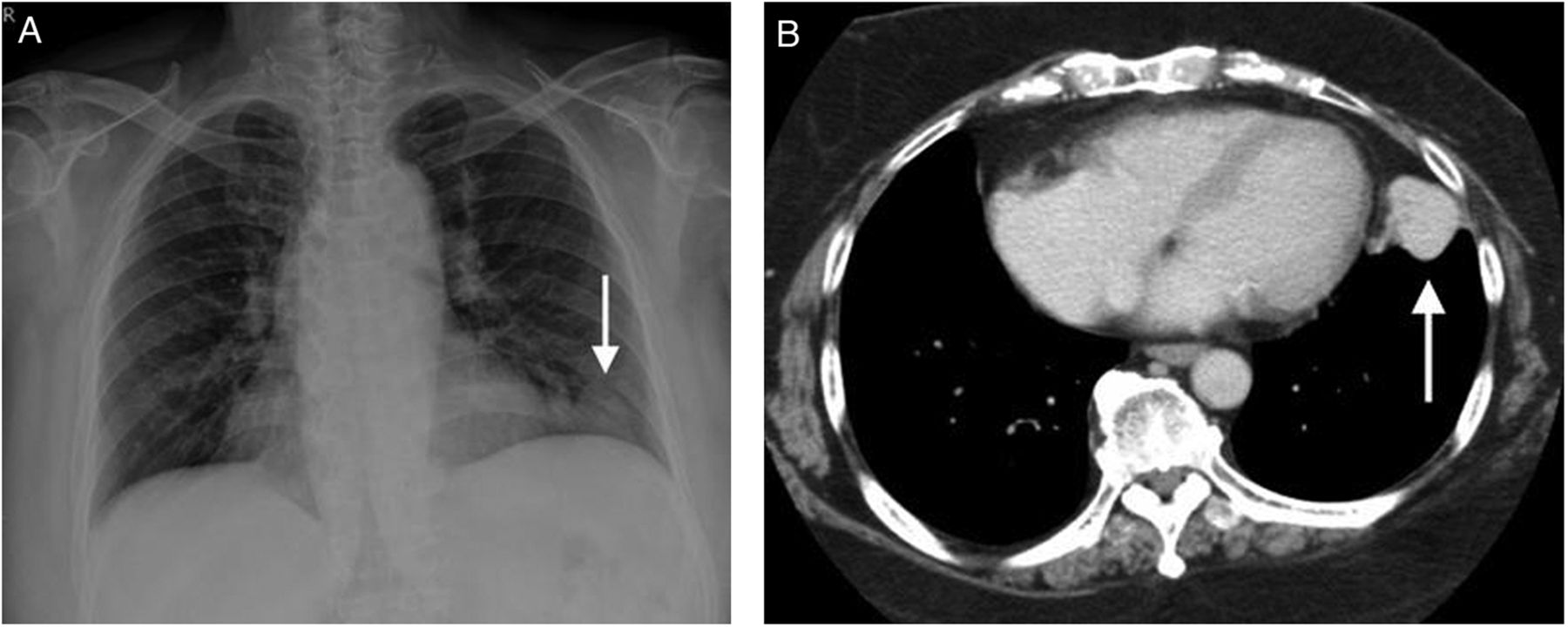
(A) Plain chest film: a faint, peripheral located nodule noted near left costo-phrenic angle. (B) Chest CT scan: a 3.6×2.8 cm solitary nodule with strong vascular enhancement.
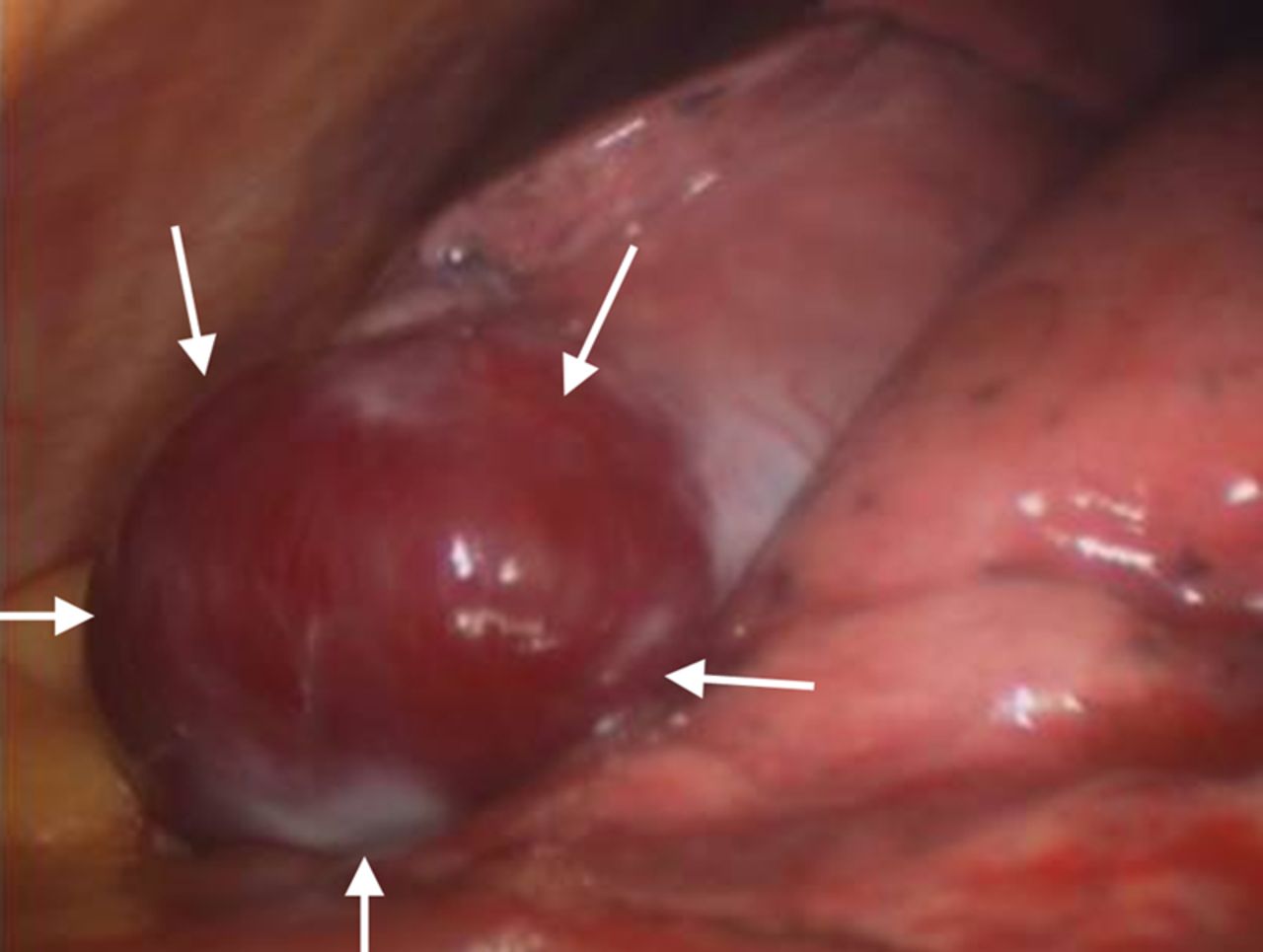
Under video-assisted thoracotomy: a cystic appearance, bright red, pulsatiled lesion.
Question
What is the diagnosis?
Answer
Macroscopically, a feeding vessel was seen entering the aneurysm cavity (figure 3A), and the microscopic appearances were consistent with a true pulmonary artery aneurysm (PAA) (figure 3B). The final diagnosis was a PAA in the left lingular lobe. The postoperative recovery was uneventful, and the patient was discharged home on day 3.

{kind=link}
{kind=link}
{kind=link}
(A) Macroscopic view of specimen with two vessel lumens in arrow. (B) Microscopic view of pulmonary artery aneurysm.
Discussion
The PAA is rare. In 1947, Deterling et al1 described only eight cases of PAA in a total of 109 571 autopsies. PAA is divided into central and peripheral types, with the former more commonly encountered. The central type involves the main pulmonary trunk or main pulmonary arteries. A congenital pathology with pulmonary hypertension or cauterisation prior to diagnosis is the usual finding in this category. The peripheral type includes lobar and segmental branches of pulmonary arteries. Syphilis, tuberculosis and trauma are the common aetiologies of solitary peripheral pulmonary aneurysm. In addition, the mycotic aneurysms are usually multiple, small in size and often with bilateral distribution. In our current case, the condition of solitary peripheral PAA in a patient without any predisposing factor is uncommon.
The most serious complication of PAA is rupture. Monchic et al2 summarised that 21 patients with solitary peripheral PAA ruptured among a total of 60 patients, with the rupture rate of 35%. Symbas et al3 reported five patients with traumatic peripheral PAA, and two patients died of aneurysm rupture, whereas two patients were treated successfully by lobectomy.
Transthoracic needle biopsy is frequently used in diagnosis of solitary pulmonary nodule, especially when it is located peripherally. It is considered a safe procedure with the bleeding rate between 2% and 10%.4 However, biopsy of a vascular structure could be fatal and, therefore, the CT scan should be carefully reviewed for its vascular enhancement before the procedure. Nowadays, (multidetector CT) MDCT angiography is a very effective tool for depicting vasculature structure.5 In our case, MDCT was not available, and needle biopsy was also declined due to strong vascular enhancement of the lesion on CT scan.
Footnotes
-
Competing interests None.
-
Patient consent Obtained.
-
Contributors C-WH and K-TK involved in collecting clinical information and drafting the manuscript. C-ML analysed the radiological studies, provided the macroscopic specimen and operation findings. C-WS carried out pathological examination. K-CK and C-TH helped in preparing this manuscript.
-
Provenance and peer review Not commissioned; externally peer reviews.