Article Text

Abstract
Concerns about the safety of long-acting β2-agonist (LABA) therapy, has led to the appearance of multiple publications and recommendations. This review critically examines the available clinical evidence and safety requirements for LABA use. On the basis of nearly 20 systematic reviews and databases, the authors conclude that LABA monotherapy significantly increases the risk of asthma-related adverse effects. We also conclude that the use of LABAs concomitantly with inhaled corticosteroids (ICS) significantly reduces asthma hospitalisations and is not associated with life-threatening events and asthma-related deaths, especially when concurrent use of LABAs and ICS can be reasonably assured (use of a single inhaler device). An appropriate clinical study would require an extremely large sample, making it impractical. Finally, some of the new US Food and Drug Administration (FDA) recommendations have caused confusion and do not appear to be fully evidence based. Although limited by low statistical power, the evidence supports the use of LABAs plus ICS in a single inhaler device (to increase adherence and reduce the potential use of LABA monotherapy) for all patients (not only children) with moderate to severe asthma.
- long-acting β agonists
- salmeterol
- formoterol
- safety
- asthma
- asthma pharmacology
- drug reactions
Statistics from Altmetric.com
Introduction
Short-acting β agonists (SABAs) have been used for decades as bronchodilators in the treatment of both chronic and acute asthma. Their therapeutic profile has generally been good, although safety concerns have persisted since SABAs were implicated in two epidemics of asthma deaths in the 1960s and 1970s.1 The question of whether these epidemics effectively resulted from the use of SABAs has been the subject of intense and persisting controversy. The introduction of long-acting β2 agonists (LABAs) in the 1990s was considered a major advance in bronchodilator therapy, with evidence that their use led to improved lung function and quality of life. However, concerns about the possible risks associated with LABA therapy appeared soon after its introduction, with the suggestion that regular use has the potential to reduce bronchodilator sensitivity to β agonists, and induce tolerance to their bronchoprotective effects.2 It also became evident that patients with asthma using LABAs may be at risk of increased morbidity and mortality if the symptom control achieved with LABA use led to a discontinuation of inhaled corticosteroid (ICS) therapy.3 Contrary to previous hypotheses, recent prospective data have shown no evidence of a pharmacogenetic effect of β-receptor variation on salmeterol response.4
Given the serious concerns about the use of LABAs for asthma, the following review critically examines the available clinical evidence and the different safety requirements for the use of LABAs.
Clinical evidence
The Serevent Nationwide Surveillance study
GlaxoSmithKline (GSK, Brentford, Middlesex, UK) sponsored the Serevent Nationwide Surveillance (SNS) study in which patients with asthma were recruited throughout the UK.5 It was a randomised, double-blind study in parallel groups over 16 weeks, comparing inhaled salmeterol (50 μg, twice daily) to salbutamol (200 μg four times daily). A total of 25 180 patients were randomised to salmeterol and 8393 to salbutamol. The only significant difference between the two groups was the number of medical withdrawals because of asthma, which were fewer with salmeterol than with salbutamol (table 1). Approximately 70% of patients received ICS concomitantly. The investigators reported 12 deaths caused by asthma in the salmeterol group (7.1 per 10 000 patients) and two in the salbutamol group (2.4 per 10 000 patients). This threefold increased risk did not reach statistical significance. Because the number of events was very small, it is not possible to determine if this difference is a chance finding. Moreover, bias may have been introduced by the higher proportion of withdrawals in the salbutamol group. Finally, the authors considered that a number of deaths could have been prevented by more appropriate use of ICS.
Summary of data from the Serevent Nationwide Surveillance study (adapted from Castle et al5)
The Salmeterol Multicenter Asthma Research Trial (SMART)
The US Food Drug Administration (FDA) required GSK to obtain additional data in a large new trial.6 This study was designed to evaluate the effects of salmeterol on respiratory and asthma-related deaths or life-threatening events. It was a multicentre, randomised, double-blind, parallel-group, placebo-controlled study conducted in the USA. Patients with asthma who were aged 12 years and over were assigned to receive either salmeterol 50 μg twice daily via metered-dose inhalers or placebo for 28 weeks in addition to their usual therapy. Initially, patients were recruited via print, radio, and television advertising from 1996 to 1999 (phase 1). When recruitment decreased, the advertising campaign was stopped and patients were recruited by the study investigators from 2000 to 2003 (phase 2). However, following an interim analysis of 26 355 patients, the sponsor decided to terminate the study due to preliminary findings in African Americans and difficulties in enrolment. This trial was planned for 60 000 patients, or 238 primary events, but was terminated when approximately half the target number of patients had been enrolled, subsequently providing 86 primary events.
Baseline ICS use was reported by 47% of the overall population, with 49% in white patients and 38% among African–American patients. Data indicate greater disease severity at baseline among the African–American subgroup compared with white patients. For the primary endpoint, there were no significant differences between treatment groups in the number of respiratory-related deaths or life-threatening events (figure 1). However, the number of combined asthma deaths and life-threatening events, and the number of asthma deaths alone were significantly higher in patients receiving salmeterol. There was one excess asthma death every 1318 salmeterol-treated patients (95% CI 734 to 23 666). Most asthma deaths occurred during phase 1 (13 of 16).

Pooled relative risk RR with 95% CI of primary and secondary endpoints during the 28-week study period in the Salmeterol Multicenter Asthma Research Trial (SMART) (n, number of events; N, total sample) (adapted from Nelson et al6).
There were statistically significant differences among the African–American population in the primary endpoint and for one of the secondary endpoints (figure 1). Although SMART was not designed to assess the effect of ICS use on the endpoints, post hoc analyses showed that the number of events for the primary and all secondary endpoints was similar for patients reporting baseline use of ICS in both treatment groups (figure 1). In contrast, the number of primary and secondary outcome events for patients reporting no baseline ICS use was significantly greater in the salmeterol group compared with the placebo group.
Overall, the results of SMART have been controversial. There were differences in baseline asthma characteristics between white patients and African–American patients (lower baseline peak expiratory flow, more nocturnal symptoms, more emergency department visits and hospitalisations, and more intubations in their lifetimes among the latter group). In the previous 12 months there were higher numbers of hospitalisations and emergency department visits in the African–American patients. There were also baseline differences in the use of ICS. Finally, the finding of more deaths with salmeterol use contrasts with national statistical data in the USA on asthma deaths and prescriptions for salmeterol and salmeterol plus ICS combinations. Extrapolation of the mortality data from SMART suggests that in 2004 there would have been twofold to threefold more asthma deaths than were reported in the national statistics.
Formoterol studies
The use of formoterol was approved in the USA in a 12 μg formulation based on two 12-week studies7 8 and one 1-year study in children aged 5–12 years.9 Clinical studies caused concern about a possible relationship between the use of higher doses (24 μg twice daily) and an increase in serious asthma exacerbations.10 As a consequence, the FDA asked the manufacturer (Novartis Pharmaceuticals Basel, Switzerland) to conduct a phase IV post-marketing clinical trial to investigate the relative safety of the two different doses of formoterol.11 This trial, which enrolled 2085 patients with stable mild-to-moderate persistent asthma (64% received regular concomitant ICS), showed five (0.9% of all patients) severe asthma-related complications in the group receiving 24 μg formoterol compared with two (0.4%) in the 12 μg group, and only one (0.2%) in the placebo group, suggesting that formoterol 24 μg twice daily was associated with an increase in serious asthma exacerbations. Likewise, tabular data from Novartis12 showed an increased incidence of serious asthma-related events in patients taking formoterol. Although the FDA confirmed the availability of both salmeterol and formoterol, black box warnings were required on their product labels.13
The FDA meta-analysis
This meta-analysis was in response to the recommendations from the Paediatric Advisory Committee meeting (28 November 2007) to continue assessing the risks and benefits of LABAs.14 It explored possible associations of LABAs with asthma hospitalisations, intubations, and deaths. It was based on data from 110 randomised, parallel controlled clinical trials (60 954 patients) that the sponsors submitted to the FDA. The meta-analysis considered four products that contain a LABA and are approved in the USA for the treatment of asthma: salmeterol plus fluticasone, formoterol, salmeterol, and formoterol plus budesonide. The majority of patients (>70% of total sample) were from salmeterol trials. SMART6 provided a substantial percentage (43%) of the total sample. For the overall analysis, 77% of patients were aged between 18 and 64 years, 11% between 12 and 17 years, 7% 65 years and over, and only 6% between 4 and 11 years. The majority of patients were white (72%), female (57%), and from trials with treatment durations of 12 weeks or more (94%).
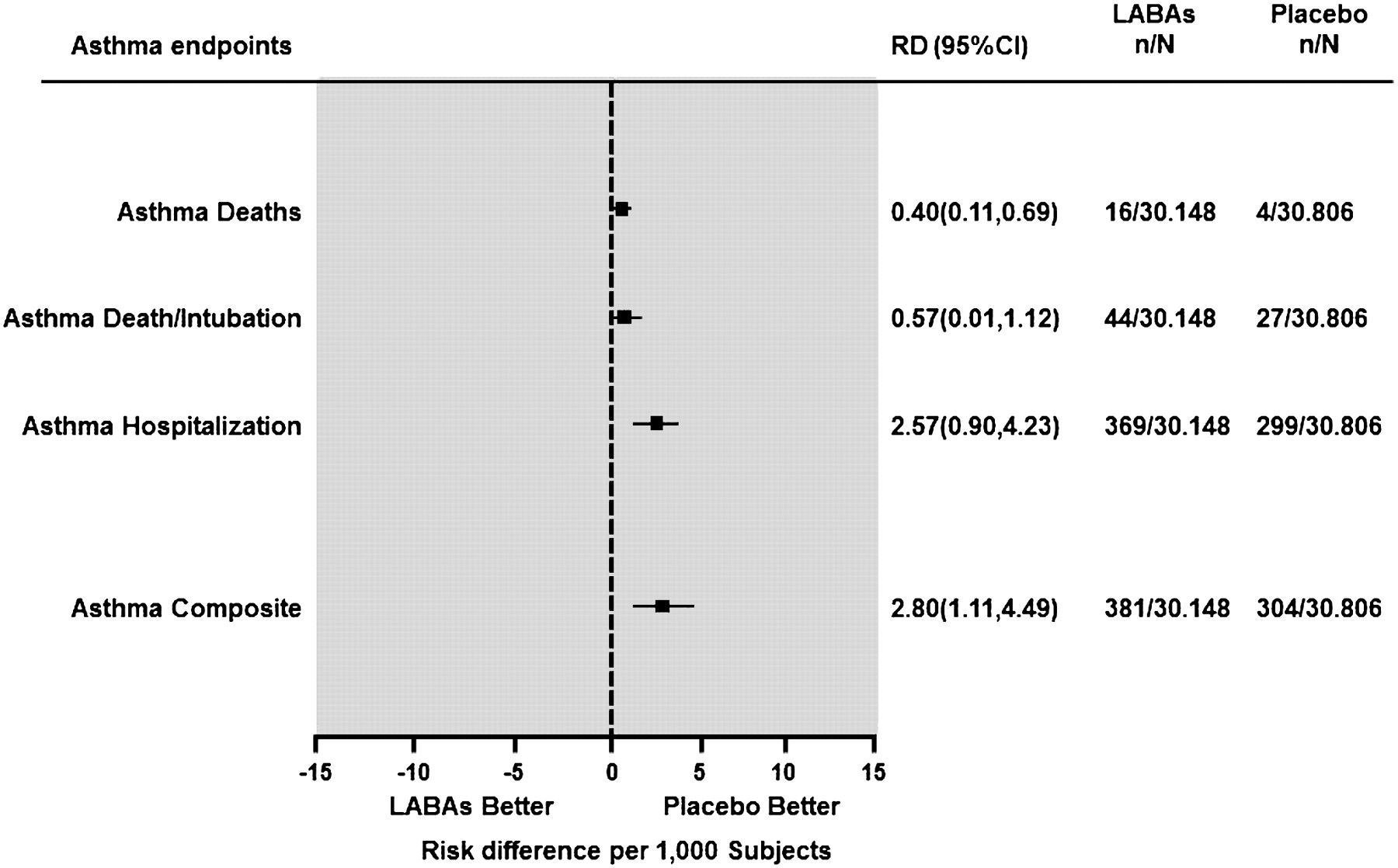
Overall, data showed that LABAs were associated with an increased risk difference (RD) of asthma-related events relative to non-LABA treatment as measured by the asthma composite endpoint consisting of asthma deaths, asthma intubations, and asthma hospitalisations (figure 2). Non-LABA treatments included ICS, SABAs, other non-LABA treatments, placebo, or a combination of treatments. This overall finding was supported by a significant increase in the asthma composite endpoint, but not in the individual endpoints.

Pooled risk difference (RD) with 95% CI of asthma endpoints in the US Food and drug Administration (FDA) meta-analysis (n, number of events; N, total sample; LABAs, long-acting β2 agonists) (adapted from Levenson14).
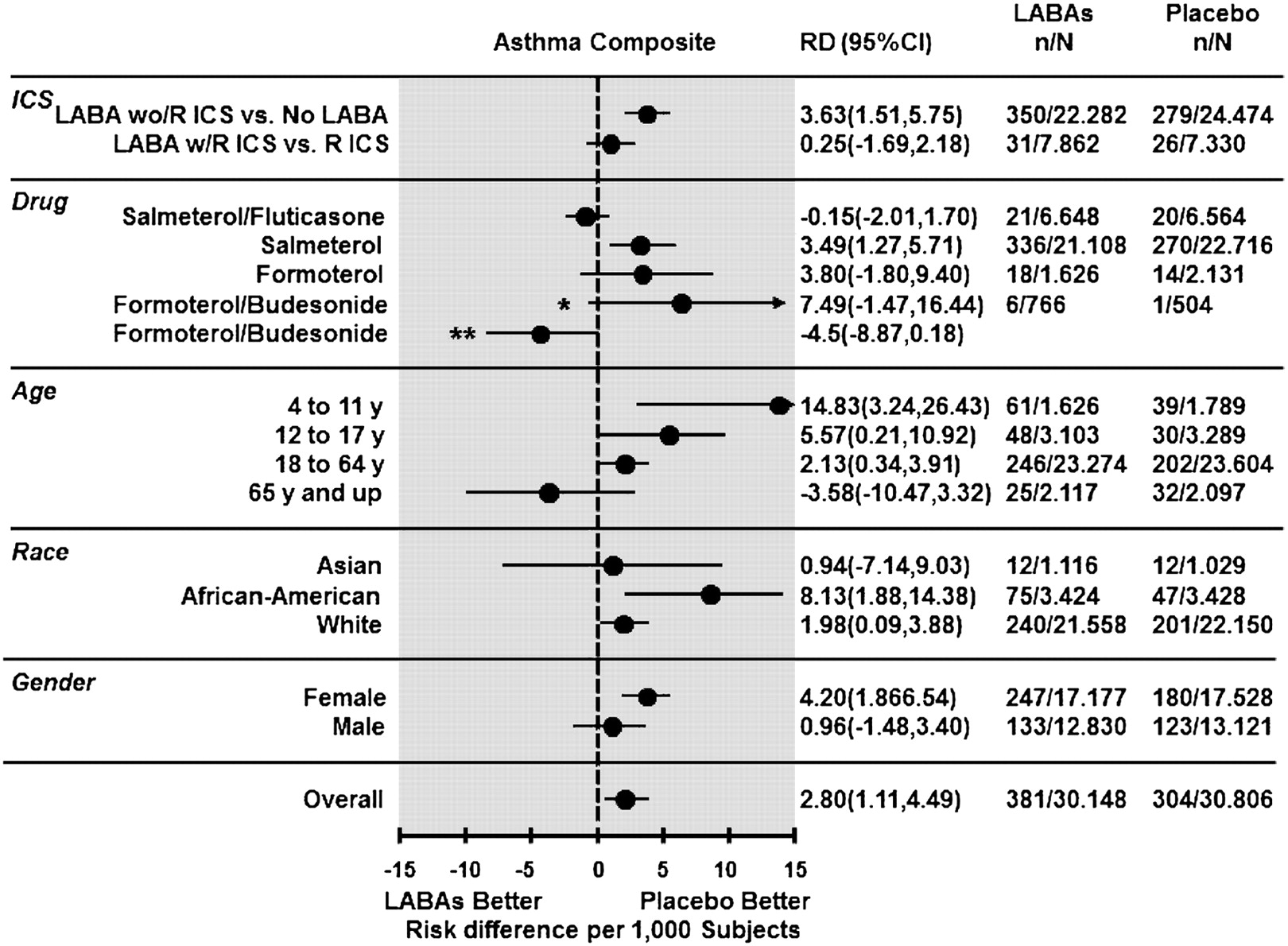
Interestingly, RDs for the asthma composite endpoint only increased when LABAs without randomly assigned ICS were compared with non-LABA treatment (figure 3). In contrast, the comparison of LABAs with randomised ICS versus randomised ICS alone (same ICS and dose) was not statistically significant. Three of the four products (formoterol, salmeterol, and formoterol plus budesonide) showed non-significant increases in the RD for the asthma composite endpoint; only salmeterol had a statistically significant estimate. There were 20 asthma-related deaths, 16 of which were in the LABA group (all occurred among salmeterol-treated patients) and four in the non-LABA group. It should be noted that the majority of trials submitted by AstraZeneca (Lund, Sweden) for the formoterol plus budesonide combination were not included in the FDA analysis (38 studies with 22 240 patients) for different reasons (non-US-approved doses and age (4–11 years).15 In contrast to the FDA analysis (four trials with 1270 patients), which showed a non-significant increased risk of asthma-related hospitalisations (RD=7.49 per 1000 patients), the analysis of the 44 trials (23 510 patients) submitted by AstraZeneca showed a non-significant decreased risk (RD=−4.5 per 1000 patients) for formoterol plus budesonide (figure 3). There was a general trend among age, with higher RD among the younger age groups. RDs for all age groups, except the 65 and over age group, were positive and statistically significant. Women and African Americans showed significant increases in RD.
{kind=link}
{kind=link}
{kind=link}
Pooled risk difference (RD) with 95% CI of asthma composite by subgroups in the FDA meta-analysis (n, number of events; N, total sample; LABAs, long-acting β2-agonists; LABAs wo/R ICS versus No LABAs, LABAs without randomised ICS versus no LABAs; LABAs w/R ICS versus R ICS, LABAs with randomised ICS versus randomised ICS). *RD from 4 (n=1270) of 42 (n=23 510) studies included in the FDA analysis; **RD from 42 (n=23 510) studies) (adapted from Levenson14).
In summary, LABAs were associated with an increased risk of an asthma composite endpoint. Of 44 deaths and intubations in the LABA-exposed population, 43 occurred among 22 286 patients (0.19%) in trials in which ICS use was not mandatory compared with one death among 7862 patients (0.01%) in trials with mandatory ICS therapy. No deaths or intubations were reported for patients treated with single-device combinations of ICS and LABAs.
Systematic reviews with meta-analyses based on randomised controlled trials and clinical databases
Because of the rarity of death in asthma clinical trials, one useful approach is to analyse systematic reviews using a meta-analysis based on randomised controlled trials (RCTs). The authors examined 16 meta-analyses: three compared LABAs with placebo,16–18 eight compared LABAs plus ICS with ICS alone,19–26 and three presented both comparisons.27–29 Additionally, we evaluated two databases of RCTs submitted by the sponsors to the FDA.30 31
Of the six reviews comparing LABAs with placebo (table 2), four17 18 27 29 showed significant increases in asthma deaths in the LABA group, with one excess asthma death every 1127–1824 LABA patients. The majority of deaths recorded in these reviews were from SMART. The only review that examined exclusively the effect of formoterol16 presented only one asthma death in the LABA group. LABA monotherapy increased the risk of life-threatening asthma and asthma hospitalisation events, although in some reviews the effect was not statistically significant.17 27 29 Clearly, analysis of these data confirms previous concerns arising from studies such as SNS or SMART. An important limitation was the low number of paediatric studies.
Data from a meta-analysis of randomised, controlled trials comparing long-acting β2 agonists with placebo*
Reviews comparing LABAs plus ICS versus ICS alone showed quite a different picture (table 3). All reviews, except two,28 29 presented the same dose of ICS in both arms, and one included trials exclusively in children.22 Overall, asthma deaths and life-threatening events were very rare, and patients treated with LABAs plus ICS presented a reduced risk of asthma hospitalisations. The only paediatric review22 did not show asthma deaths or life-threatening events. However, it presented a non-significant increased risk of asthma hospitalisations.
Data from a meta-analysis of randomised, controlled trials comparing long-acting β2 agonists plus inhaled corticosteroids with ICS alone (same dose as a part of the study protocol)
These findings differ markedly from the Salpeter et al review.28 These authors selected RCTs (≥3 months) that compared LABAs with placebo or LABAs plus ICS with ICS alone. The primary outcome was catastrophic events, defined as asthma-related intubation or death. Using data from six trials and one database provided by GSK (7253 patients), the authors concluded there was a surprisingly threefold increase in catastrophic events among patients treated with LABAs plus ICS compared with those treated with ICS alone (table 3). Nevertheless, this finding appears problematic because of different factors. Therefore, all trials included were very heterogeneous in terms of doses of ICS. Additionally, many patients received ICS as uncontrolled background treatment, and only a few studies used single inhaler devices for the combination therapy administration. Of particular interest is the GSK database of RCTs of salmeterol30 included in the Salpeter analysis. In response to an FDA request of January 2008, GSK submitted a database with a meta-analysis of 215 studies representing over 100 000 patients. These data explain 57% (8 of 14) of the primary outcome events for LABA plus ICS therapy in the Salpeter review. Three clinical situations were examined during which a patient could have received ICS concurrently with salmeterol: the addition of salmeterol to background ICS (ICS were not administered as part of the protocol); salmeterol and ICS as blinded study medications administered in separate inhaler devices, as part of the study protocol; and administration of salmeterol and ICS as a blinded study medication in a single inhaler. Only the last situation assures the concurrent use of ICS each time a patient was exposed to salmeterol. Therefore, the latter population was the most accurate to inform the safety profile of salmeterol in the presence of ICS. The results showed (table 4) that for studies in which the concurrent use of salmeterol and ICS can be reasonably assured (eg, salmeterol plus ICS in a single inhaler device vs ICS), there was no evidence of increased risk for asthma deaths or intubations. In contrast, when salmeterol was used in the absence of an ICS or when the use of an ICS was not controlled (eg, salmeterol plus ICS vs ICS background or separate inhaler devices), an increase (although not significant) in serious asthma-related events was observed. A final objection to the Salpeter review is the absence of several additional published and unpublished studies that met the inclusion criteria.
Risk differences per 10 000 patients for asthma-related deaths and intubations (adapted from GlaxoSmithKline30)
AstraZeneca (Lund, Sweden) also submitted a comprehensive review to the FDA of the available data for formoterol plus budesonide metered-dose inhalers and Turbuhaler trials (≥12 years).31 The most relevant subset of the full dataset consists of 15 852 patients across 27 studies and consists of patients that received formoterol plus ICS versus ICS alone. There were no asthma-related deaths, and the FDA asthma composite endpoint (death, intubation, and hospitalisation) decreased significantly (odds ratio (OR)=0.62; 95% CI 0.42 to 0.93) in patients receiving combination therapy.
A different development for combined ICS plus LABA treatment is the use of budesonide plus formoterol as both maintenance and reliever therapy (SMART strategy).32 Safety data from six double-blind RCTs (14 346 patients) in which budesonide plus formoterol was used for at least 6 months showed good tolerance and no increased safety concerns, with lower or similar incidence of death and asthma-related serious adverse events compared with the fixed-dose comparators.33
Finally, the analysis of 41 AstraZeneca-sponsored RCTs (≥3 months)34 showed that formoterol (82% with concomitant ICS) as maintenance and/or as reliever therapy with almost 12 000 children and adolescents was not associated with any increased risk of asthma hospitalisations. There was only one asthma death among formoterol-treated patients.
Are new data needed?
Although mortality is a very rare event in the use of LABAs with mandatory ICS trials, estimates of risk should be interpreted with caution, given that such trials were not powered on these events. Accordingly, the FDA is requiring the manufacturers of LABAs to conduct additional studies to evaluate their safety.35 Likewise, some authors36 37 have issued a call for a very large randomised clinical study. The appropriate next step could be to conduct an adequately powered, well designed, prospective study to define the magnitude of the risk resulting from treating patients with asthma with LABAs plus ICS versus the same dose of ICS alone. Kazani et al38 proposed that 50 000 patients with moderate or severe asthma should be enrolled in a randomised double-blind trial, with half of the patients treated with ICS and the other half treated with ICS plus LABAs. Enrolled patients should be followed until 20 severe asthma episodes or asthma deaths have occurred in the entire cohort. However, this proposed study would not have the power to definitively rule out a relative risk of less than fourfold because the sample size was based on data from LABA studies that did not mandate ICS use. In contrast, Sears38 states that a large trial is neither practicable nor necessary and will not provide any more useful data about adverse asthma events than those presently available. Based on data from the FDA meta-analysis,14 Sears has estimated the large sample sizes necessary for different outcomes (table 5). The use of the FDA composite outcome of deaths, intubations and hospitalisations would introduce major difficulties in interpretation because data have shown that LABA use with concomitant randomised ICS is either neutral in risk for exacerbations (dominantly hospitalisations), or reduces risk.5 23–27 Therefore, using the composite outcome would produce results opposing those suggested by the worst-case interpretation of the mortality data.
Sample sizes calculations for a new study comparing long-acting β2 agonists plus mandatory inhaled corticosteroids versus ICS alone (adapted from Kazani38)
Observational studies
With rare outcomes of treatment, such as asthma mortality, the failure of different designs to detect associations may represent type II error, and so indicate a lack of statistical power rather than the absence of an association. Researchers should very cautiously interpret evidence of safety for a rare adverse event, such as asthma death with LABA use, based on the traditional categories of evidence. It has been established that in a real scenario, meta-analyses of RCTs and single large RCTs lack statistical power to detect or rule out this association.39 Case–control methodology may be a better approach because it requires a smaller sample size. However, the risks of bias are higher than those of a well designed RCT, or a properly conducted meta-analysis of RCTs.
A case–control study of 532 patients who died from asthma found an association between asthma deaths and use of SABAs in the period 1–5 years prior to death40 without evidence of any positive association of LABAs in any period (3, 4–12 months and 1–5 years before death). Another case–control study used the UK's General Practice Research Database (GPRD) (96 258 patients) to assess respiratory mortality and found the strongest association with heavy use of SABAs.41 Lanes et al42 performed an open cohort study with a nested case–control analysis in the UK based on the GPRD (14 657 patients). The authors concluded that salmeterol use was not associated with an increase in short-term mortality compared with the use of ipratropium and theophylline. Finally, Lang et al43 looked at data on asthma hospitalisations in Philadelphia from 1995 to 1999 and prescription rates for LABAs and other asthma drugs. The authors found that asthma hospitalisation was significantly associated with increased SABA prescriptions, poverty, area of residence, and African–American identity. By contrast, LABAs appeared to be protective, with lower rates of hospitalisation. However, asthma deaths are highly related to health behaviour, psychosocial factors,44 poor adherence, and the underuse of primary care services,45and it is unlikely that sufficient information will be available in epidemiological datasets to deal completely with these biases. Finally, ecological analysis of asthma-related events and ICS dispensing observational data have shown a gradual reduction in asthma mortality in the USA since 2000, in the setting of a marked increase in LABA use predominantly in combination therapy.46
A novel approach has recently been developed to describe the patterns of hazard rates of asthma outcomes with changes in exposures.47 This pattern analysis focuses on the convergence or divergence of hazard rates rather than on estimating relative rates. The objectives of this study were to describe the patterns of risk of death and asthma outcomes with exposure to different asthma medications in general practice, and to statistically compare these patterns of risk among LABAs, inhaled SABAs and ICS. The study population included patients receiving β-agonist treatment aged 18 years and over in the UK GPRD (507 966 patients), which is linked to the national registry of hospitalisations. The mortality rate increased with the least and the most severe treatment steps. Higher relative rates of outcomes were found in patients who had recently started treatment and in those receiving long-term LABA, SABA and ICS treatment. The relative death rate was statistically similar over time between LABAs and ICS despite differences in exposure. There were no statistically significant increases in the risk of death and asthma outcomes with LABAs compared with other asthma medications.
FDA 2010 new safety requirements for LABAs
Recently, because of safety concerns and exercising new authority under the FDA Amendments Act of 2007, the FDA implemented new recommendations about how LABAs should be used in the treatment of asthma.48 The specific label changes were:
the use of LABAs without the use of an asthma controller medication such as an ICS is contraindicated (absolutely advised against) in the treatment of asthma;
LABAs should only be used as additional therapy for patients with asthma who are currently taking a long-term asthma control medication, such as an ICS, but whose symptoms are not adequately controlled;
LABAs should be used for the shortest period of time required to achieve control of asthma symptoms and then discontinued, if possible, once asthma control is achieved; patients should then be maintained on asthma controller medication;
paediatric and adolescent patients who require the addition of an LABA to an ICS should use a combination product containing both an ICS and a LABA to ensure adherence to both medications.
These changes are based on FDA analyses of studies showing an increased risk of severe adverse effects in paediatric and adult patients using LABAs for the treatment of asthma.
These recommendations appropriately emphasise the risk associated with the use of LABA monotherapy (largely based on findings of SNS and SMART trials 5 6 and meta-analysis). 12 27 29 Also, the FDA's reminder that LABAs are not recommended as adjunct therapy in patients whose asthma is adequately controlled with low-dose ICS agrees with the National Asthma Education and Prevention Program's Expert Panel Report-3 (EPR-3) guidelines.49 However, some of the new recommendations have caused confusion and do not appear to be fully evidence based.50 For example, the change proposed by the FDA in point 3 implies that once adequate control is achieved after the addition of an LABA to ICS therapy, initial consideration should be given to stepping down therapy by discontinuing the LABA. However, the EPR-349 and the Global Initiative for Asthma 51 guidelines recommend that care is stepped down only after asthma control is achieved and maintained for a sufficient length of time (several months). The idea of stopping LABA use ‘once control is achieved’ suggests a quick or sudden withdrawal of therapy (LABAs) as soon as control is achieved. We must keep in mind that the concept of asthma control includes two different domains (impairment and risk), and that medications might affect the two in different ways, particularly in patients with severe asthma. In fact, evidence suggests that stopping LABAs after the achievement of asthma control results in the patient's asthma becoming less controlled.52 Recently, Reddel et al53 showed that patients with well controlled asthma who are taking high doses of ICS plus LABAs can safely reduce the ICS dose to levels that are lower than advisable with ICS alone, without loss of asthma control or evidence of disease activity.
The FDA's recommendation against LABA use in patients whose asthma is controlled with a low–medium dose of ICS is also controversial. Therefore, the EPR-349 considers the choice of either increasing the dose of an ICS or adding a LABA as equal options for preferred step-up therapy. This recommendation is the result of weighing the benefits of combining LABAs and low-dose ICS therapy and the infrequent risk of serious adverse events. In effect, there is a large body of evidence that supports the superior effectiveness of adding LABAs to low-dose ICSs rather than increasing the dose of ICSs, even in preschoolers and school children with moderate to severe asthma, and in adults with asthma.54 55 Finally, it is difficult to understand why the FDA recommended the use of combination products in a single device only in children and adolescents. The difficulty of ensuring compliance might apply to all age groups. Actually, there are no data to indicate a higher risk exclusively in the paediatric population. Compliance to treatment is a crucial issue of the therapeutic process that can increase the risk of serious adverse effects. It has been suggested that adherence profiles of ICS plus LABAs in a single inhaler are significantly better when compared with the controller regimens in separate inhalers.56
Conclusions
Based mainly on the safety concerns arising from the SNS and SMART5 6 studies, some authors have suggested withdrawing LABA use for asthma therapy. However, these serious events have been infrequent and appeared when LABAs were used as monotherapy. By contrast, evidence from RCTs, meta-analysis of RCTs and observational studies, although limited by low statistical power, have indicated that the use of combination therapy (LABAs plus ICS) is associated with a decreased risk of serious asthma-related events. This is particularly true when the concomitant use of LABAs plus ICS can be reasonably assured (combined in a single inhaler). Therefore, the use of separate inhalers could result in periods of LABA monotherapy because of poor compliance with ICS use. Combination therapy could reduce asthma mortality by increasing the prescription and increasing compliance with ICS in the community. Furthermore, combination therapy should be applied to all patients with moderate to severe asthma, and not just paediatric and adolescent patients, as suggested by the FDA guidelines.
References
Supplementary materials
Web Only Data thx.2010.155648
Files in this Data Supplement:
Footnotes
Funding This study came from salary support for Drs Rodrigo and Castro-Rodriguez.
Competing interests In the past 3 years, GJR has received compensation for participating as a lecturer and speaker in scientific meetings and courses under the sponsorship of Boehringer Ingelheim, GlaxoSmithKline, AstraZeneca, Dr Esteve SA and Merck Sharp & Dome, and received a consulting fee from Almirall. JCR received compensation for participating as a lecturer and speaker in scientific meetings and courses under the sponsorship of Merck Sharp & Dohme, GlaxoSmithKline and AstraZeneca.
Provenance and peer review Not commissioned; externally peer reviewed.