Article Text

Abstract
Context Newborn screening for cystic fibrosis (CF) is included in many routine programmes but current strategies have considerable drawbacks, such as false-positive tests, equivocal diagnosis and detection of carriers.
Objective To assess the test performance of two newborn screening strategies for CF.
Design, setting and participants In 2008 and 2009, CF screening was added to the routine screening programme as a prospective study in part of the Netherlands.
Interventions Two strategies were performed in all newborns. In the first strategy, concentrations of immunoreactive trypsinogen (IRT) and pancreatitis-associated protein (PAP) were measured. In the second method, samples with IRT ≥60 μg/litre were analysed for 36 CFTR mutations, followed by sequencing when a single mutation was detected. Tests were positive only with two identified CFTR mutations.
Main outcome Sensitivity, specificity and positive predictive value (PPV) of both screening strategies.
Results 145 499 infants were screened. The IRT/PAP approach showed a sensitivity of 95.0%, a specificity of 99.897% and a PPV of 12.3%. Test properties for the IRT/DNA/sequencing strategy were respectively 100%, 100% and 64.9%. Combining both strategies (IRT/PAP/DNA/sequencing) led to a sensitivity of 95.0%, a specificity of 100% and a PPV of 87.5%.
Conclusion In conclusion, all strategies performed well. Although there was no statistically significant difference in test performance, the IRT/DNA/sequencing strategy detected one infant that was missed by IRT/PAP (/DNA/sequencing). IRT/PAP may be the optimal choice if the use of DNA technology must be avoided. If identification of carriers and equivocal diagnosis is considered an important disadvantage, IRT/PAP/DNA/sequencing may be the best choice.
- Cystic fibrosis newborn screening
- immunoreactive trypsinogen
- pancreatitis-associated protein
- mutation analysis
- sequencing
- sensitivity
- specificity
- clinical epidemiology
- cystic fibrosis
- infection control
- alpha1 antitrypsin deficiency
- lung cancer
- lung proteases
- macrophage biology
- respiratory infection
- cystic fibrosis
- oxidative stress
- asthma
- exhaled airway markers
- paediatric asthma
- paediatric physician
- respiratory infection
Statistics from Altmetric.com
- Cystic fibrosis newborn screening
- immunoreactive trypsinogen
- pancreatitis-associated protein
- mutation analysis
- sequencing
- sensitivity
- specificity
- clinical epidemiology
- cystic fibrosis
- infection control
- alpha1 antitrypsin deficiency
- lung cancer
- lung proteases
- macrophage biology
- respiratory infection
- cystic fibrosis
- oxidative stress
- asthma
- exhaled airway markers
- paediatric asthma
- paediatric physician
- respiratory infection
Key messages
What is the key question?
Newborn screening programmes for cystic fibrosis have considerable drawbacks, such as false-positive tests, equivocal diagnosis and detection of carriers. This study investigated three novel screening strategies.
What is the bottom line?
A screening strategy consisting of immunoreactive trypsinogen and pancreatitis-associated protein, DNA and sequencing has the best test performances and less carrier detection and equivocal diagnosis than other programmes.
Why read on?
We show the results of three screening programmes for cystic fibrosis, the test performances, number of carriers detected and equivocal diagnosis.
Introduction
Newborn screening (NBS) for cystic fibrosis (CF) is widely accepted, but there is no universally accepted screening strategy.1 A survey of screening programmes in Europe described 26 different screening strategies.2
All programmes start by measuring the concentration of immunoreactive trypsinogen (IRT) in dried blood spots. The second tier is either a limited CFTR mutation analysis or a repeat measurement of the IRT concentration at the age of 4–6 weeks.3 Protocols using IRT alone or IRT/IRT have a high false-positive rate.4 The major drawback of using CFTR mutation analysis is the high number of identified healthy carriers and cases with an equivocal diagnosis.1 5
In 2005, pancreatitis-associated protein (PAP) was described as a possible second tier in NBS for CF. Measurement of IRT as well as PAP in dried blood spots may lead to a specific and sensitive screening programme.5 6 A different IRT/PAP protocol was used in Germany in 2009; that is, a 99th percentile IRT cut-off level and a PAP cut-off level of 1.6 μg/l.7
Screening with IRT/DNA followed by sequencing of the CFTR gene in all samples with only one CFTR mutation may be an alternative strategy. In this approach the screening test is only positive when two mutations are identified.8 In California a comparable screening protocol has been in use since 2007, but infants with a single mutation are also referred for a sweat test.9
We hypothesised that these two novel screening strategies (IRT/PAP and IRT/DNA/sequencing) may lead to a similar sensitivity to current NBS strategies, but with a higher specificity, less carrier detection and less equivocal diagnoses. The study aim was to compare the test performance of these two strategies in a large population of newborns in the Netherlands.
Methods
Study population
In the Netherlands all newborns are included in the routine NBS programme, unless the parents refuse participation (opting-out procedure). The Dutch NBS programme consists of 17 diseases (congenital adrenal hyperplasia, congenital hypothyroid disease, sickle cell disease and 14 metabolic diseases; http://www.rivm.nl/hielprik). Five laboratories spread over the country perform NBS, and receive heel prick samples from five designated areas. Two laboratories, the reference laboratory (RIVM) and the laboratory of the region South East (Clinical Chemical Laboratory, St Elisabeth Hospital, Tilburg) participated in the study.
All heel prick samples received in the two participating laboratories were tested with both screening strategies in 2008 and 2009, unless the parents refused the screening for CF. Parents were informed about the screening for CF by a leaflet, available in 10 languages.
Screening protocols
Figure 1 shows a flow chart of both screening strategies. The IRT/PAP protocol consisted of measurement of IRT and PAP in all samples. A positive result was defined as a combination of IRT ≥100 μg/litre and PAP ≥1.6 μg/litre or IRT ≥60 μg/litre and PAP ≥3.0 μg/litre, as described before,6 and corrected according to the publication at http://www.isns-neoscreening.org/htm/news in March 2011. In the IRT/DNA/sequencing protocol, an elevated IRT (≥60 μg/l) was followed by a DNA mutation analysis consisting of 36 mutations. When only one mutation was detected, DNA sequencing was performed. In this strategy the screening test was positive when two mutations were detected. All newborns with a positive screening result with one or both strategies were referred to a CF centre for a sweat test to confirm or to exclude the diagnosis.

Flowcharts of both screening strategies: immunoreactive trypsinogen (IRT)/pancreatitis-associated protein (PAP) and IRT/DNA/sequencing. CF, cystic fibrosis.
Definitions
The diagnosis of CF was confirmed by a sweat chloride concentration of ≥60 mmol/litre. If this was not possible or the sweat test failed, the diagnosis can also be confirmed by two CFTR mutations, and/or a meconium ileus and/or positive family history.10 11
An equivocal diagnosis was defined according to international standards as an equivocal sweat test result (chloride 30–60 mmol/litre) or a normal sweat test result (chloride <30 mmol/litre) on two occasions in a newborn with two CFTR mutations of which one or both have unclear clinical consequences.11 All infants with an equivocal diagnosis were regularly seen at the CF centres during the first year of life. For the IRT/PAP strategy, CF was excluded when the chloride concentration was below 30 mmol/litre. For the IRT/DNA/sequencing strategy newborns with a single CFTR mutation after DNA sequencing were considered as healthy carriers and screen negative.
Laboratory techniques
The AutoDELFIA Neonatal IRT (B005-112, Perkin-Elmer, Turku, Finland) was used for determination of IRT, according to the manufacturer's protocol.
For measuring PAP, the MucoPAP ELISA (DynaBio, Marseille, France) was modified to a DELFIA method following a protocol of PerkinElmer. This is a time-resolved fluoroimmunoassay, based on a biotinylated anti-PAP antibody and a 100 μl Eu-Streptavidin tracer. The minimal detectable value of the PAP assay was 0.1 μg/litre and the maximal value 15.8 μg/litre.
DNA was extracted from dried blood spots using the EZ1 DNA tissue kit on a Biorobot EZ1 (Qiagen, Valencia, California, USA). Mutation analysis of the CFTR gene was performed by screening for 35 CFTR mutations with the Line Probe Assay of Innogenetics (INNO-LiPA CFTR19 and INNO-LiPA CFTR17+Tn) (Innogenetics, Gent, Belgium) or by DNA sequence analysis of all coding exons of the CFTR gene (including intron/exon boundaries) using standard procedures. Newborns with two CFTR mutations or one CFTR mutation and one variant with unknown clinical significance were referred. Polymorphisms and variants known to cause only male infertility were considered non disease causing and ignored.
Sweat tests were performed by the Gibson-Cooke Quantitative Pilocarpin Iontophoresis or the Macroduct method according to international guidelines.12
The Dutch Pediatric Surveillance Unit
Paediatricians in the Netherlands reported all children with a new diagnosis of CF to the Dutch Paediatric Surveillance Unit (DPSU). This registration started in July 2007 and is still running. The main goal of the registration is to find infants missed by NBS.
Retrospective analysis
When parents gave permission, we performed a retrospective analysis using both screening protocols in heel prick cards of children reported to have CF at the DPSU and those from the four participating CF centres born since 2003.
Statistical analysis
We determined the test characteristics (with 95% CIs) of the two screening protocols (sensitivity, specificity and positive predictive value (PPV)). For determination of the sensitivity, newborns with a meconium ileus were excluded from the analysis.13
A power analysis was made for both specificity and sensitivity. For both strategies a cohort of 80 000 newborns would be sufficient to show that the specificity will be higher than 99.64% with a power of 80%. Assuming a sensitivity of 95% a total number of 62 infants with CF will lead to an estimated 95% CI between 85% and 99%. To achieve a reliable estimate of the sensitivity a cohort of children known to have CF was added to the study for a retrospective analysis.
We compared the test performances of the two strategies using a McNemar's test. p Values <0.05 were considered statistically significant.
A post hoc analysis was done for a combined IRT/PAP/DNA/sequencing strategy using the data of both strategies. Statistical analysis was carried out using SPSS V.17.0 software.
Results
In 2008 and 2009, 145 499 newborns were screened for CF; 72 874 in 2008 and 72 625 in 2009. A total number of 372 713 newborns were born alive in the Netherlands in both years; the study region counted for 39% of all births.
IRT/PAP strategy
Results of the IRT/PAP strategy are shown in figure 2A and tables 1 and 2. A total of 171 (0.12%) newborns were referred for a sweat test. CF was confirmed in 19 newborns. One infant was missed because of a low PAP concentration (0.8 μg/litre); this infant had two mutations (F508del and A455E) and a positive sweat test (chloride 65 mmol/litre).

(A) Results of the immunoreactive trypsinogen (IRT)/pancreatitis-associated protein (PAP) screening strategy. (B) Results of the IRT/DNA/sequencing screening strategy (2008 and 2009). CF, cystic fibrosis.
Results of three different screening strategies with an immunoreactive trypsinogen cut-off level of 60 μg/l (n=145 499)
Immunoreactive trypsinogen and pancreatitis-associated protein concentrations, CFTR gene mutation analysis and sweat tests in infants with cystic fibrosis detected by newborn screening
Six infants had an equivocal sweat test result (chloride concentration 30–51 mmol/litre); two of these infants were diagnosed with CF by two mutations (F508del and F508del); one of them had an abnormal repeat sweat test (69 mmol/litre). One infant had a normal repeat sweat test and no mutations. In three infants a follow-up sweat test was not performed by the paediatric pulmonologist because the DNA results showed no mutations.
IRT and PAP concentrations for the whole population are presented in figure 3.
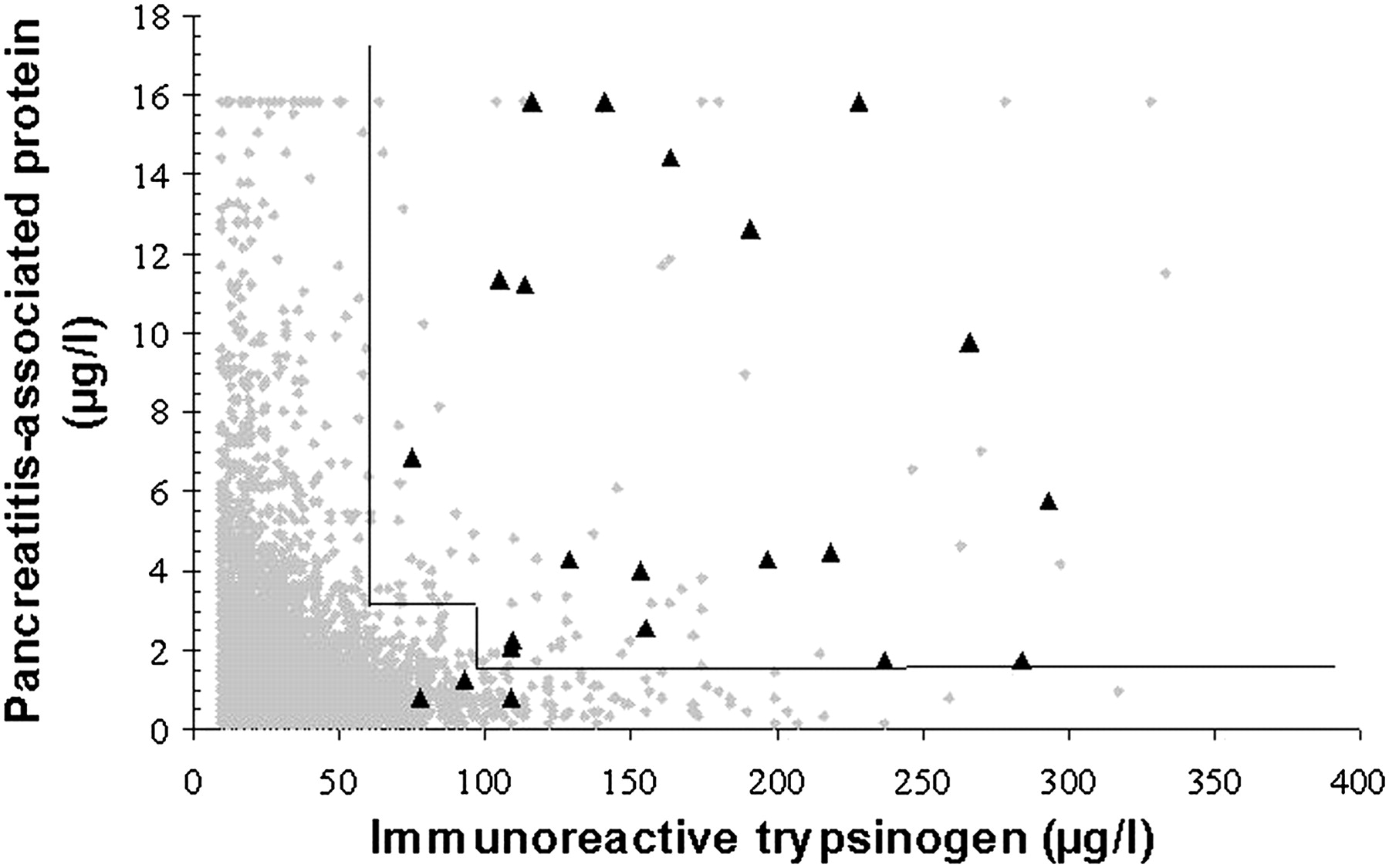
Correlation between immunoreactive trypsinogen and pancreatitis-associated protein concentrations in heel prick blood.
IRT/DNA/sequencing strategy
The results are presented in figure 2B and tables 1 and 2.This strategy revealed 20 infants with CF, 13 infants with an equivocal diagnosis and 67 carriers, and had a referral rate of 0.026%. The PPV of this strategy was 64.9% because infants with an equivocal diagnosis cannot be considered to have CF.
IRT/PAP and IRT/DNA/sequencing identified the same 19 patients, whereas the second strategy detected one more patient. Although the IRT/DNA/sequencing strategy was better for sensitivity, specificity and PPV (McNemar; p=1.00) the differences were not significant. The prevalence of CF in the study region was 1:6062.
IRT/PAP/DNA/sequencing strategy
A post hoc analysis was performed for the IRT/PAP/DNA/sequencing strategy. In this strategy a DNA mutation analysis would be done in all samples with a positive IRT/PAP result, followed by sequencing when a single mutation was found. The results are presented in figure 4 and table 1. With this screening strategy the same 19 patients as in the IRT/PAP strategy would have been found, three infants with an equivocal diagnosis and eight carriers.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Adjusted cut-off levels. CF, cystic fibrosis; IRT, immunoreactive trypsinogen; PAP, pancreatitis-associated protein.
Diagnosis
Sweat tests were performed between 3 and 4 weeks after birth. A total of 175 sweat tests were performed of which 145 succeeded (83%). In five infants no sweat test was done because of a congenital lethal condition (n=3; cardiomyopathy, multiple congenital anomalies and trisomy 18), refusal of the parents (n=1; no mutations after DNA analysis), a premature infant of 25 weeks (n=1; the DNA analysis was repeated instead of the sweat test).
The sweat test confirmed the diagnosis of CF in 17 infants. The test failed in two infants but their diagnosis could be based on two mutations (F508del and F508del) and clinical symptoms (ileum atresia and meconium plug respectively). One infant had an equivocal sweat test result but was diagnosed because of two mutations (F508del and F508del).
The IRT/DNA/sequencing strategy revealed 13 infants with an equivocal diagnosis, all of whom had two mutations identified, with one of the two being of unclear clinical significance. Three of these infants had equivocal sweat test results (chloride 33, 34, 36 mmol/litre; all had R117H-7T as a second mutation), the other 10 had normal sweat tests (F508del/394delTT/S1251N/R553X combined with R117H-7T n=8, F508del/L967S, F508del/Q1352H) (table 3).
Immunoreactive trypsinogen and pancreatitis-associated protein concentrations, CFTR gene mutation analysis and sweat tests for all infants with an equivocal diagnosis
Time to diagnosis
Median times between heel prick and screening test result and between screening test result and diagnosis are shown in table 4. All infants with CF were diagnosed within 2 months of birth. In 90% of all newborns, the heel prick was taken within 144 h of birth (day 6). Median age at heel prick was 96 h (day 4) (IQR 96–120). Median time between heel prick and screening test result was 7 days for IRT/PAP (IQR 5–9) and 16 days for IRT/DNA/sequencing (IQR 15–19). For IRT/PAP/DNA/sequencing the predicted time between heel prick and test result is 21 days. The period of uncertainty for parents from being informed about a positive heel prick result and confirmation or exclusion of the diagnosis was 4 days (IQR 3–7) in the first year of the study, and 1 day (IQR 1–7) in the second year, for both strategies.
Time to diagnosis
DPSU and the retrospective analysis
Between January 2008 and April 2011 no false-negative results were reported.
A retrospective analysis was performed in 74 cards. IRT and PAP concentrations declined with age of the heel prick card, therefore the results of the retrospective analysis could not be used to determine the sensitivity of this strategy. Our mutation panel detected two mutations in 66 cards, one mutation in seven cards and no mutations in one card. Eight cards were sequenced and after sequencing all cards contained two mutations. The 36-mutation panel therefore had a sensitivity of 98.6% (95% CI 91.6 to 99.9) for detection of one or two mutations.
Discussion
As far as we know, our study is the first prospective study comparing two novel screening strategies in NBS for CF (IRT/PAP and IRT/DNA/sequencing). The best test performance was found for IRT/DNA/sequencing. A post hoc analysis of a combination of both strategies (IRT/PAP/DNA/sequencing) resulted in a programme with a sensitivity similar to IRT/PAP but a higher specificity and PPV. This third strategy led to detection of considerably fewer carriers and fewer equivocal diagnoses than current screening strategies. This strategy has never been studied before.
All infants with CF were diagnosed within 2 months of birth, which is within the window of opportunity to create a better prognosis.14 Our study has some limitations that should be considered in the interpretation of the results. The currently most applied screening strategy for NBS for CF is the IRT/DNA strategy with referral of all infants with one or two mutations. In an ideal study design this strategy would have been used as the ‘gold standard’. Using our study data an IRT/DNA programme would have had a sensitivity of 100% (95% CI 88.2% to 100%), a specificity of 99.954% (95% CI 99.941% to 99.964%) and a PPV of 26.4% (95% CI 17.9% to 36.8%), this may be investigated prospectively in a new study comparing those protocols. However, sequencing the CFTR gene in all infants with a single mutation and an equivocal sweat test is advised as the optimal diagnostic strategy in the current European consensus guidelines,11 and this most probably has a similar sensitivity to performing a sweat test in infants with a single CFTR mutation. Moreover, within our study it was possible to compare specificity and PPV with the ‘gold standard’ strategy; the IRT/DNA/sequencing strategy appears to have a considerably better specificity as well as PPV. We did not find a statistically significant difference between the IRT/PAP and IRT/DNA/sequencing strategies; this may have been caused by the relatively small number of infants with CF in our screened population, which is also a limitation of our study.
The diagnosis was confirmed by the sweat test in 17 of the 20 infants. In all cases the diagnosis could be confirmed according to the international definition10 11 by a sweat test or a second DNA analysis and clinical symptoms and/or a sibling with CF. We used the DPSU to detect children with CF who were potentially missed by screening.
The power analysis showed that we needed 62 infants to determine the sensitivity reliably. In the study design a retrospective analysis of children known to have CF was planned to calculate the sensitivity, but this partly failed because IRT and PAP concentrations decreased over time (results not shown). The prevalence of CF in our study was 1:6062. In 2005 and 2006, the Dutch CF Registry registered a nationwide prevalence of 1:5000 comparable to the prevalence of 1:4750 published in 2005.15 The reason for this difference may be that the prevalence of CF is declining as it is in the whole of Europe.16 17 Causes for this decline may be preconception and prenatal screening, parents deciding not to have any more children with NBS detecting carrier couples. Another cause may be a lower prevalence of CF in the southern part of the Netherlands where our study was performed.18 19 Our results for IRT/PAP are comparable to the findings of two previous studies.6 7 One previous study found a sensitivity of 100% for detection of CF with a specificity of 99.81% and a PPV of 9.4%.6 Another prospective study comparing IRT/PAP with IRT/DNA showed a sensitivity of 85.7%, a specificity of 99.90% and a PPV of 12.2% for the IRT/PAP strategy.7 The sensitivity in the last study appears low but this study used a slightly different protocol.
Internationally used screening programmes consisting of IRT, IRT/IRT or IRT/DNA (one or more mutations) show variable test performances.4 IRT/IRT programmes show a sensitivity between 80.2% and 96.8%, with a specificity of 99.8%.20 21 In DNA-based programmes (IRT/DNA, IRT/DNA/IRT, IRT/IRT/DNA), the sensitivity varies depending on the mutation panel, the IRT cut-off level and the fail-safe procedures. Previous studies showed sensitivities of between 96.0% and 99.5% with specificities between 99.60% and 99.97%.22–24
IRT/PAP has advantages compared with DNA-based programmes. First, no carriers are detected. Although carrier detection is sometimes considered an advantage, this is not a universal opinion.25–28 The advantages of detection of trait-trait couples and extended family screening do not counterbalance this disadvantage in our opinion. Second, no second heel prick is needed in contrast to IRT/IRT programmes. Disadvantages are the high number of false-positive test results, and a long period of uncertainty and parental stress due to the frequent failure of the sweat test.
The IRT/DNA/sequencing strategy had the best test performance in our study, but this strategy led to equivocal diagnoses and identified carriers. However, the number of referrals was considerably lower and the specificity and PPV higher than those of the most applied screening strategy, IRT/DNA. In contrast to current IRT/DNA-based programmes, the advantage of the IRT/DNA/sequencing approach was that parents were not aroused by a positive screening test result when a single mutation was identified.29 The information leaflet about NBS for CF that the parents received at three occasions (during pregnancy, when registering the baby and immediately before the heel prick) mentioned that parents could ask for the DNA results, but very few parents did (0.007%).
Eleven of the 13 infants with an equivocal diagnosis in the IRT/DNA/sequencing strategy had R117H-7T as a second mutation. Most of them had normal sweat test results (table 3), which means that they would probably have a normal or subnormal CFTR function. The Dutch CF Registry showed only 10 patients (1196 registered patients in 2008) with a R117H-7T mutation, and only four of them were diagnosed under the age of 18 years. Our findings confirm an earlier observed discrepancy in frequency of this mutation in screened populations and CF registries. This indicates that this mutation mostly acts as a non-disease-causing variant.30 31 Many experts on NBS for CF therefore advise exclusion of this mutation.31 If R117H-7T were to be excluded from the panel, only two infants with an equivocal diagnosis would have been identified with this strategy. With a IRT/DNA strategy these two infants would probably not be identified as having an equivocal diagnosis but only as carriers.
Because of the multi-ethnic Dutch population, infants with two rare mutations in the non-Caucasian population might be missed when using a DNA-based screening strategy. But in the retrospective analysis we identified only one patient that would not have been detected by the IRT/DNA/sequencing analysis. The IRT/PAP strategy reveals infants with CF because of high IRT and PAP levels, which makes this a more robust screening strategy when the screened population has ethnic differences.
In conclusion, all three studied screening strategies seem useful for NBS for CF, but the choice of which strategy to implement depends on the requirements of the test. Both strategies (IRT/PAP and IRT/DNA/sequencing) performed well, better than expected. Although there was no statistically significant difference, the IRT/DNA/sequencing strategy detected one infant that was missed by IRT/PAP. This strategy also leads to fewer referrals and therefore to a higher specificity and PPV than the current IRT/DNA strategy. IRT/PAP may be the optimal choice if the use of DNA technology must be avoided. When identification of carriers or false-positive results are considered to be important disadvantages and the number of equivocal diagnoses should be minimised, IRT/PAP/DNA/sequencing may be the best choice. The Dutch Ministry of Health decided to implement this last strategy in the Dutch NBS programme as of 1 May 2011.32
Acknowledgments
We thank the paediatric pulmonologists and CF nurses in the four participating CF centres for their care for the parents and their children: H G M Arets and Professor C K van der Ent, C de Kiviet (University Medical Centre Utrecht); Professor H A W M Tiddens, Y B de Rijke, A Kok and I Heeres (Erasmus Medical Centre Rotterdam); J B Yntema and J Sintnicolaas (Radboud University Nijmegen Medical Centre); Professor E Dompeling and D Holtslag (Maastricht University Medical Centre). We also thank Paul Verkerk from TNO Quality of Life for his contribution in preparation of the study protocol.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Download Supplementary Data (PDF) - Manuscript file of format pdf
Footnotes
See Editorial, p 281
CHOPIN Study Group J E Dankert-Roelse, MD, PhD, A M M Vernooij-van Langen, MD (Atrium Medical Centre); J G Loeber, PhD, L H Elvers (RIVM); R H Triepels, PhD (St Elisabeth Hospital); J J P Gille, PhD (VUmc); C P B Van der Ploeg, PhD (TNO Quality of Life); E Dompeling, MD, PhD (MUMC); G Pals, PhD (VU Medical Centre), S M van der Pal, PhD, M E van den Akker van Marle, PhD (TNO Quality of Life); V A M Gulmans, PhD (NCFS, Dutch CF Foundation), M J W Oey-Spauwen, MD, Y H H M Wijnands, MD, L M Castricum, MD (RIVM); H G M Arets, MD, PhD, Professor C K van der Ent, MD, PhD (University Medical Centre Utrecht); Professor H A W M Tiddens, MD, PhD, Y B de Rijke, PhD (Erasmus Medical Centre Rotterdam); J B Yntema, MD, PhD (Radboud University Nijmegen Medical Centre).
Funding ZonMw, the Dutch Organization for Health Research Development, financed the study at the request of the Dutch Health Council. ZonMw in no way influenced the data collection, analysis or interpretation of the results, and they did not comment about the writing of this article or the decision for submission.
Competing interests None.
Ethics approval The Medical Ethical Committee of the Atrium Medical Centre approved the performance of the CHOPIN study according to the Good Clinical Practice guidelines and privacy statements.
Provenance and peer review Not commissioned; externally peer reviewed