Article Text

Statistics from Altmetric.com
- Granulomatosis
- lymphomatoid
- precancerous conditions
- pulmonary vasculitis
- rare lung diseases
- systemic disease and lungs
- interstitial fibrosis
- pulmonary lymphoma
- antineutrophil cytoplasmic antibody related vasculitides
- ARDS
- assisted ventilation
Case presentation
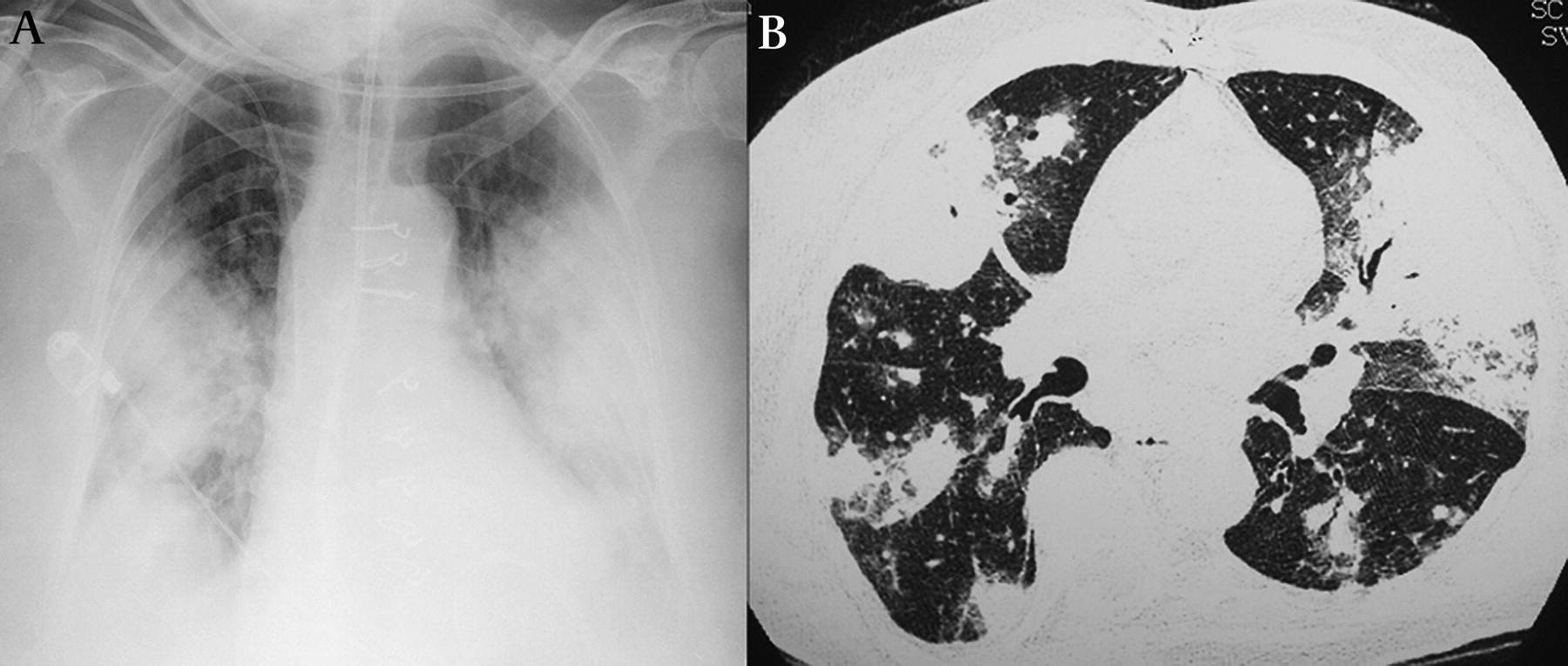
A 67-year-old woman presented to the emergency room in acute respiratory failure. She had a 4-month history of dry cough, fever, intense fatigue, progressive dyspnoea and recent visual impairment. Her prior medical history included a mitral valve replacement in 2005 due to post-endocarditis mitral regurgitation. On examination, the patient was in hypoxemic acute distress. She was intubated and mechanically ventilated. A chest x-ray (figure 1A) just prior to endotraqueal intubation revealed bilateral air space disease and high-resolution CT of the chest (figure 1B) revealed irregular nodules, bilateral areas of conglomerate masses with air bronchograms of peribronchovascular orientation surrounded by ground glass opacities and no mediastinal lymphadenopathy. Laboratory findings indicated mild normocromic and normocytic anaemia, haemoglobin 10 g/dl, lymphopenia 168 cells/mm3, C-reactive protein 157 mg/litre (0.0–3.0 mg/litre). Tests for HIV, serum cytoplasmic antineutrophil cytoplasmic antibody, antinuclear antibody and rheumatoid factor were negative. A transesophageal echocardiogram displayed a bioprosthetic mitral valve with mild stenosis, no evidence of endocarditis, and minimum regurgitation with negative blood cultures. MRI of the brain displayed bilateral optic neuritis.
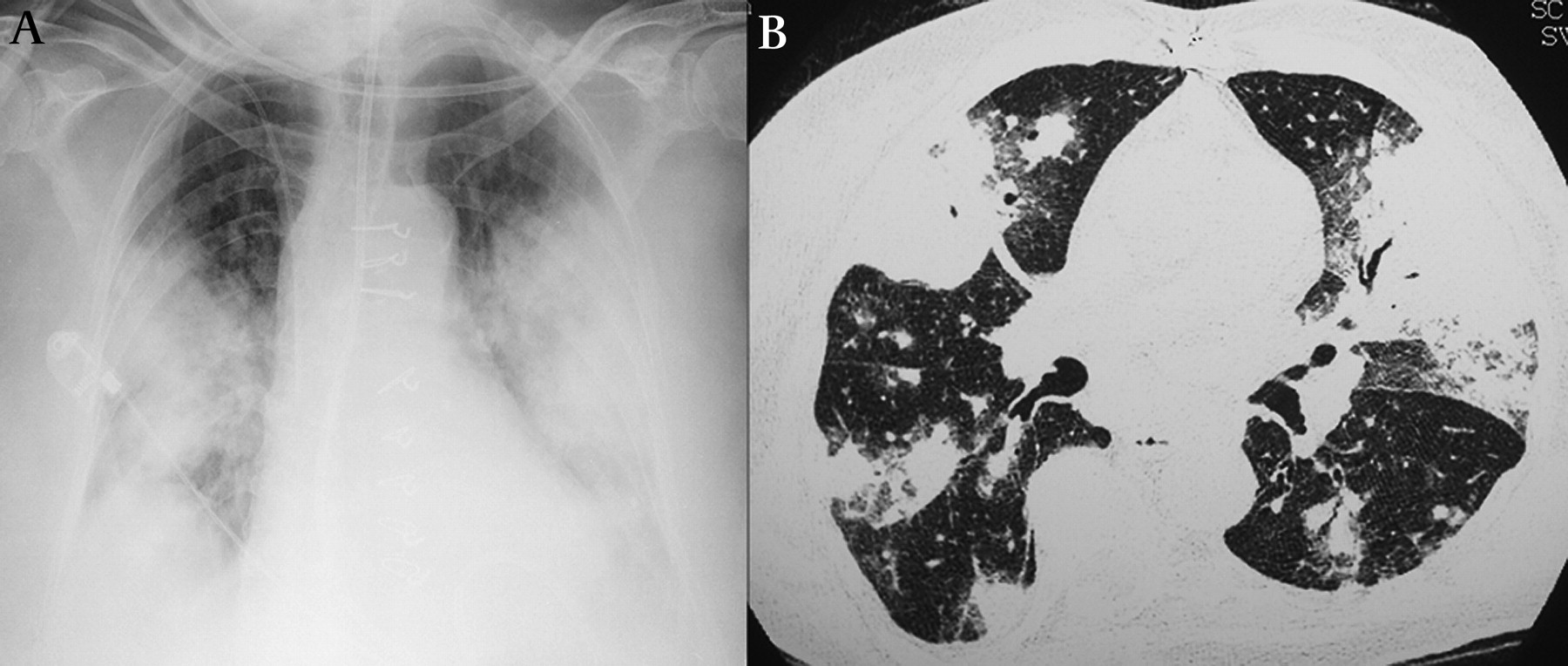
(A) Chest x-ray (anteroposterior view) just prior to endotracheal intubation revealed midline sternotomy metallic wires, bilateral mass-like opacities predominating in the middle and lower lung zones. (B) High-resolution CT of the chest revealed nodules, bilateral areas of conglomerate masses with air bronchograms of peribronchovascular distribution surrounded by ground glass opacities.
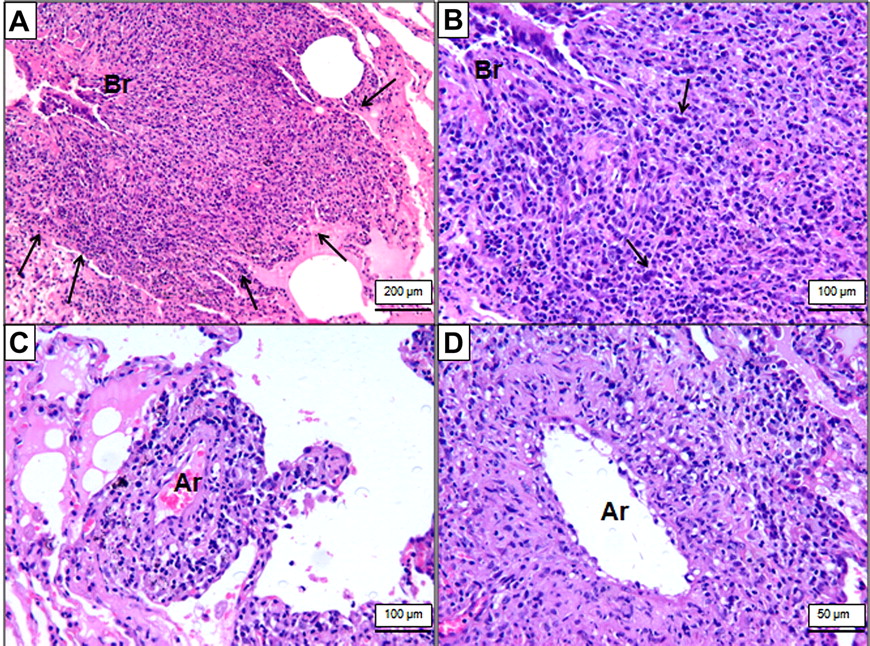
An open lung biopsy was performed: angiocentric nodules comprised a mixture of lymphocytes with variable numbers of associated plasma cells and histiocytes (figure 2A). The lymphocytic infiltrate was mainly composed of small and intermediate size cells that were CD3 positive T lymphocytes. Scattered large atypical cells (figure 2B) were CD20 positive B lymphocytes. The polymorphic lymphoid infiltrate showed a distinctive predilection to infiltrate vessel walls (figure 2C), resulting in thickening of the lumens of affected vessels (figure 2D).

{kind=link}
{kind=link}
Low magnification photomicrograph illustrating a zone of pulmonary parenchyma displaying a dense cellular infiltrate forming angiocentric nodules (A, arrows). A high-magnification view illustrating a polymorphic lymphocytic infiltrate that includes isolated large atypical cells (B, arrows). A transmural infiltrate of lymphoid cells involving a pulmonary artery is shown in panels (C) and (D). Hematoxylin-eosin stain. Ar, artery; Br, bronchioli.
Question
What is the diagnosis?
See page 280 for the answer
Answer
From the question on page 273
Lymphomatoid granulomatosis (LYG) grade 1 was diagnosed. LYG is a rare T-cell rich, Epstein-Barr virus (EBV)-associated, B-cell lymphoproliferative disorder. Lung involvement is the predominant feature but extrapulmonary manifestations occur, especially skin and nervous system involvement such as optic neuritis.1 2 Systemic symptoms and lymphopenia are also described. Lung Involvement in LYG may be unilateral or bilateral and includes interstitial and alveolar compartments of the lung. The most common radiographic findings are multiple nodular opacities and masses with poorly defined margins distributed along the peribronchovascular bundle or interlobular septa.3 Reticular opacities associated with nodules, mediastinal lymphadenopathy and large conglomerate masses with air bronchograms are also observed.3
Histologic and immunohistochemical features are crucial for LYG diagnosis: mixed mononuclear cell infiltrate containing CD20-positive large B lymphocytes and numerous CD3-positive small lymphocytes, vascular infiltration, necrosis, and evidence of EBV infection.1 Positivity for EBV infection in histological specimens ranges from 57 to 100% and therefore its absence does not rule out the diagnosis in proper clinical, radiological and histological scenarios, as was the case for our patient.1 4
Grade 1 LYG contains only a few large B cells whereas numerous large B cells are present in grade 3 disease, which means worse prognosis. Current knowledge about LYG tends to categorise grades 2 and 3 as lymphomas, considering the frequent presence of monomorphous foci of atypical B cells and the clinical behaviour.1 5
The treatment of LYG is not well established. There has been a tendency to treat higher grade LYG with chemotherapy regimens for lymphomas but the treatment for grade 1 LYG is less clear.1 There are some reports of spontaneous resolution and treatment success with interferon alfa-2b, corticosteroids, cyclophosphamide, and bone marrow transplant. Our patient was treated with corticosteroids, cyclophosphamide and rituximab with complete remission of lung lesions. The optic neuritis also remitted but the patient retained significant visual impairment. The patient was placed on prednisone and oral cyclophosphamide with slow tapering in the following 18 months. There have been no recrudescences in the last 3 years of follow-up.
Footnotes
Competing interests None.
Patient consent Obtained.
Ethics approval Ethics approval was provided by CAPPesq.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Data about the case report are available upon request from the corresponding author.
Linked Articles
- Airwaves