Article Text

Abstract
Background Short-term exposure to air pollution can trigger hospital admissions for asthma in children, but it is not known which components of air pollution are most important. There are no available studies on the particular effect of ultrafine particles (UFPs) on paediatric admissions for asthma.
Aim To study whether short-term exposure to air pollution is associated with hospital admissions for asthma in children. It is hypothesised that (1) the association between asthma admissions and air pollution is stronger with UFPs than with coarse (PM10) and fine (PM2.5) particles, nitrogen oxides (NOx) or nitrogen dioxide (NO2); and (2) infants are more susceptible to the effects of exposure to air pollution than older children.
Method Daily counts of admissions for asthma in children aged 0–18 years to hospitals located within a 15 km radius of the central fixed background urban air pollution measurement station in Copenhagen between 2001 and 2008 were extracted from the Danish National Patient Registry. A time-stratified case crossover design was applied and data were analysed using conditional logistic regression to estimate the effect of air pollution on asthma admissions.
Results A significant association was found between hospital admissions for asthma in children aged 0–18 years and NOx (OR 1.11; 95% CI 1.05 to 1.17), NO2 (1.10; 95% CI 1.04 to 1.16), PM10 (1.07; 95% CI 1.03 to 1.12) and PM2.5 (1.09; 95% CI 1.04 to 1.13); there was no association with UFPs. The association was stronger in infants than in older children for all pollutants, but no statistically significant interaction was detected.
Conclusion Short-term exposure to air pollution can trigger hospital admission for asthma in children, with infants possibly being most susceptible. These effects seemed to be mediated by larger particles and traffic-related gases, whereas UFPs showed no effect.
- Air pollution
- hospitalisations
- childhood asthma
- case-crossover study
- asthma
- asthma epidemiology
- paediatric asthma
- COPD epidemiology
- occupational lung disease
- asthma guidelines
- asthma mechanisms
- asthma pharmacology
- exhaled airway markers
- inhaler devices
- nebuliser therapy
Statistics from Altmetric.com
- Air pollution
- hospitalisations
- childhood asthma
- case-crossover study
- asthma
- asthma epidemiology
- paediatric asthma
- COPD epidemiology
- occupational lung disease
- asthma guidelines
- asthma mechanisms
- asthma pharmacology
- exhaled airway markers
- inhaler devices
- nebuliser therapy
Key messages
What is the key question?
Is the association between asthma admissions in children and air pollution stronger with ultrafine particles (UFPs) than with coarse and fine particles (PM10, PM2.5), as suggested by animal studies and toxicology? Are infants more susceptible to the effects of exposure to air pollution than older children?
What is the bottom line?
Exposure to air pollution triggers hospital admission for asthma in children. This effect was mediated by coarse and fine particles and traffic-related gases and not by UFPs. Infants are slightly more susceptible to the effects of air pollution, but the effects or air pollution are not limited to this group of children.
Why read on?
This is the first epidemiological study of hospital admissions for asthma in children with data on UFPs measured in the same way as larger particles and gases. It is also the first study of a link between air pollution and hospital admissions for asthma in children which also includes infants, and thus tests for effect modification in air pollution by age.
Introduction
Asthma is the most common chronic disease in children and the main cause of emergency room visits,1 hospital admissions2 and school absences. The incidence of childhood asthma has increased in recent decades in high-income countries, and environmental factors have gained increasing attention in attempts to understand the determinants of the asthma epidemic.1 3 Exposure to air pollution from traffic is ubiquitous in urban environments, affecting millions of people. Children are possibly more susceptible to the effects of air pollution than adults because their lungs and immune systems are developing, they inhale higher doses of air pollution relative to adults due to differences in breathing rates and patterns, and because they are generally more active in environments with high levels of pollutants when participating in sports and outdoor play.4 Chronic exposure to traffic-related air pollution in the early years of life has been suggested to contribute to the development of asthma in children,5–7 although evidence is mixed.8 Short-term exposures of several days to elevated levels of air pollution have been shown to trigger exacerbations of asthma leading to increased rates of emergency room visits9 10 hospital admissions for asthma,9 11–19 wheezing symptoms20 and decreased peak expiratory flow.21 However, many aspects of the relationship between air pollution and childhood asthma are not fully understood, including susceptibility by age and gender as well as which pollutants are most relevant. Ultrafine particles (UFPs; particulate matter with aerodynamic diameter <0.1 μm), the smallest fraction of particulate matter generated mainly by traffic, have been suggested to have particularly strong effects in the airways due to a high level of pulmonary deposition and their ability to cause inflammation and oxidative stress.22 However, epidemiological data have not been able to confirm this hypothesis, possibly due to lack of data on UFPs.14 19 20
We have studied the effects on hospital admissions for asthma in children aged 0–18 years in Copenhagen, Denmark related to short-term changes in exposure to UFPs, nitrogen oxides (NOx) and particulate matter with aerodynamic diameter ≤10 μm and 2.5 μm (PM10 and PM2.5), and tested for the effect modification by age (infants (0–1 years), preschool children (2–5 years) and school children (6–18 years)) and gender.
Methods
Study population
Hospital admissions due to asthma were obtained from the Danish National Patient Registry (DNPR) which is managed by the National Board of Health. We extracted daily counts of hospital admissions for asthma (ICD-10 codes J45-J46) among children aged 0–18 years between 15 May 2001 and 31 December 2008. Asthma admissions were extracted from eight hospitals located within a 15 km radius (average 6 km) from the central fixed background urban air pollution measurement station in Copenhagen.
Air pollution and meteorology
The pollutant and meteorological data were measured by the Danish National Environmental Research Institute at a fixed urban background measurement station (20 m height) in the centre of Copenhagen with low contributions from local streets. Main streets are located about 300 m west and 50 m east of the monitor, with 26 000 and 56 000 vehicles passing per working day, respectively. For the study period (May 2001 to December 2008), daily (24 h, midnight-to-midnight) mean concentrations were available for PM10 (SM200 Monitor, Opsis, Sweden), PM2.5 (TEOM Ambient Particulate Monitor, Thermo Fisher Scientific Inc., Waltham, Massachusetts, USA), nitrogen dioxide (NO2) and NOx (M200A; API, Ry, Denmark), UFPs (Differential Mobility Particle Sizer, Roskilde, Denmark) and meteorology (dew point, wind speed, global radiation), with missing data on days with equipment malfunctions. Although the total numbers of particles included particles of 10–700 nm in diameter, we define them as UFPs in this study because particles <100 nm in aerodynamic diameter (by definition, UFP) comprised more than 75% of the total concentration measurements.
Study design and statistical analyses
A case crossover design was used to assess the association between hospital admissions for asthma in children and air pollution levels in Copenhagen between May 2001 and December 2008. The case crossover design was developed to examine the association between transient short-term exposure and the risk of acute events in the case-only design.23 The design compares a subject's exposure immediately prior to the case-defining event (index time) to the same person's exposure at otherwise similar reference times (control periods), with reference and index times forming a matched case–control set. As each person serves as its own control, potential confounding for all personal characteristics is accomplished, while control for time-varying factors is accomplished by choosing a referent time close in time to the index time. We applied the time-stratified referent selection approach15 by comparing air pollution concentration on the day of hospital admission for asthma with to air pollution concentrations on other days falling on the same day of the week in the same calendar month as the asthma admission. This means that, if the index day is a Monday, then control days are the remaining Mondays in the same month that year, resulting in 3–4 reference periods. We performed conditional logistic regression separately for each pollutant, using the moving average of 5-day levels of air pollutants (mean of lag 0–4) as the main exposure proxy and, additionally, considered concentrations on the same day (lag 0), previous day (lag 1) and up to 4 days (lag 4) of the hospital admission, based on results from our previous study.19 The potential effect modification of an association between air pollution and hospital admissions for asthma by gender and three age groups (infants (0–1 years), preschool children (2–5 years) and school children (6–18 years)) were evaluated by introducing interaction terms into the model and tested by the Wald test. Two-pollutant models were fitted for the 5-day moving average to examine the robustness of one-pollutant association. Effects estimates were reported as OR associated with interquartile range (IQR) increases in air pollution concentration. The meteorological conditions, which may affect the risk of hospital admission for asthma as well as the levels of air pollution, were controlled by fitting the daily mean dew point, wind speed and global radiation by restricted cubic splines with three degrees of freedom for the same lag as the pollutants in the model. The natural logarithm was applied to normalise the air pollutants before the statistical analysis. Several sensitivity analyses were performed, including fitting the logistic regression model without wind speed and fitting the data with an alternative statistical model for Poisson data in time series format (ie, Generalised Additive Model (GAM)), with adjustment for meteorology and calendar time with restricted cubic splines. Only complete cases were considered in the analyses. The analyses were conducted using the software R, Version 2.12.0.
Results
A total of 8226 hospital admissions for asthma were recorded among children aged 0–18 years in the eight study hospitals in Copenhagen between 15 May 2001 and 31 December 2008, with a mean of 2.95 admissions per day. Of the 8226 hospital admissions, 2765 (33.6%) were for infants (0–1 years), 2892 (35.2%) for preschool children (2–5 years) and 2569 (31.2%) for school children (6–18 years). The majority of admissions were boys (67.3%).
Air pollution and meteorological conditions in Copenhagen between 2001 and 2008 are shown in table 1, and the correlations between pollution and weather are shown in table E1 in the online supplement. The yearly distribution of air pollution levels and meteorological conditions are given in table E2 in the online supplement. The monthly number of asthma admissions during the study period and the monthly levels of NOx and UFPs are shown in figure 1. The variation in hospital admissions over time showed approximately the same temporal variation as that of NOx, indicating similar patterns of higher levels in winter and lower levels in summer, while the variations in UFPs did not correlate well with asthma admissions.
Air pollutant levels and meteorological conditions in urban background in Copenhagen (May 2001-December 2008)

Number of hospitalised children with asthma during the study period (dashed lines) and average monthly air pollution measured as (A) nitrogen oxides (NOx) in parts per billion and (B) ultrafine particles (UFPs) in particles/cm3 (solid lines).
Air pollution and risk of hospital admission for asthma
We detected a significant positive association between hospital admissions for asthma in children and air pollution measured as NOx, NO2, PM10 and PM2.5, whereas a weak positive and non-significant association was detected with UFPs (table 2). The highest risk estimate per increase in IQR of 5-day mean air pollution levels prior to hospital admission for asthma was observed for NOx (1.11; 95% CI 1.05 to 1.17), followed by NO2 (1.10; 95% CI 1.04 to 1.16), PM2.5 (1.09; 95% CI 1.04 to 1.13) and PM10 (1.07; 95% CI 1.03 to 1.12). No significant effect modification between air pollution levels and asthma hospital admissions were detected by age or gender (table 2).
Association* between air pollution (per IQR increase in mean 5-day (lag0-4) levels) and hospital admission for asthma in children, and effect modification by gender and age
The effect of NOx was slightly attenuated but significant in all two-pollutant models, except for NO2 (table 3) which showed a stronger association with hospital admissions for asthma than any other pollutant. The effect of NO2 was also slightly attenuated in two-pollutant models, except for PM2.5 and UFPs. The effect of PM10 and PM2.5 was slightly attenuated in two-pollutant models, except for the effect of PM10 which was slightly enhanced in the model with PM2.5. The effect of UFPs diminished after adjustment for other pollutants.
Association* between air pollution (per IQR increase in mean 5-day (lag 0–4) levels) and hospital admission for asthma in children: two-pollutant models
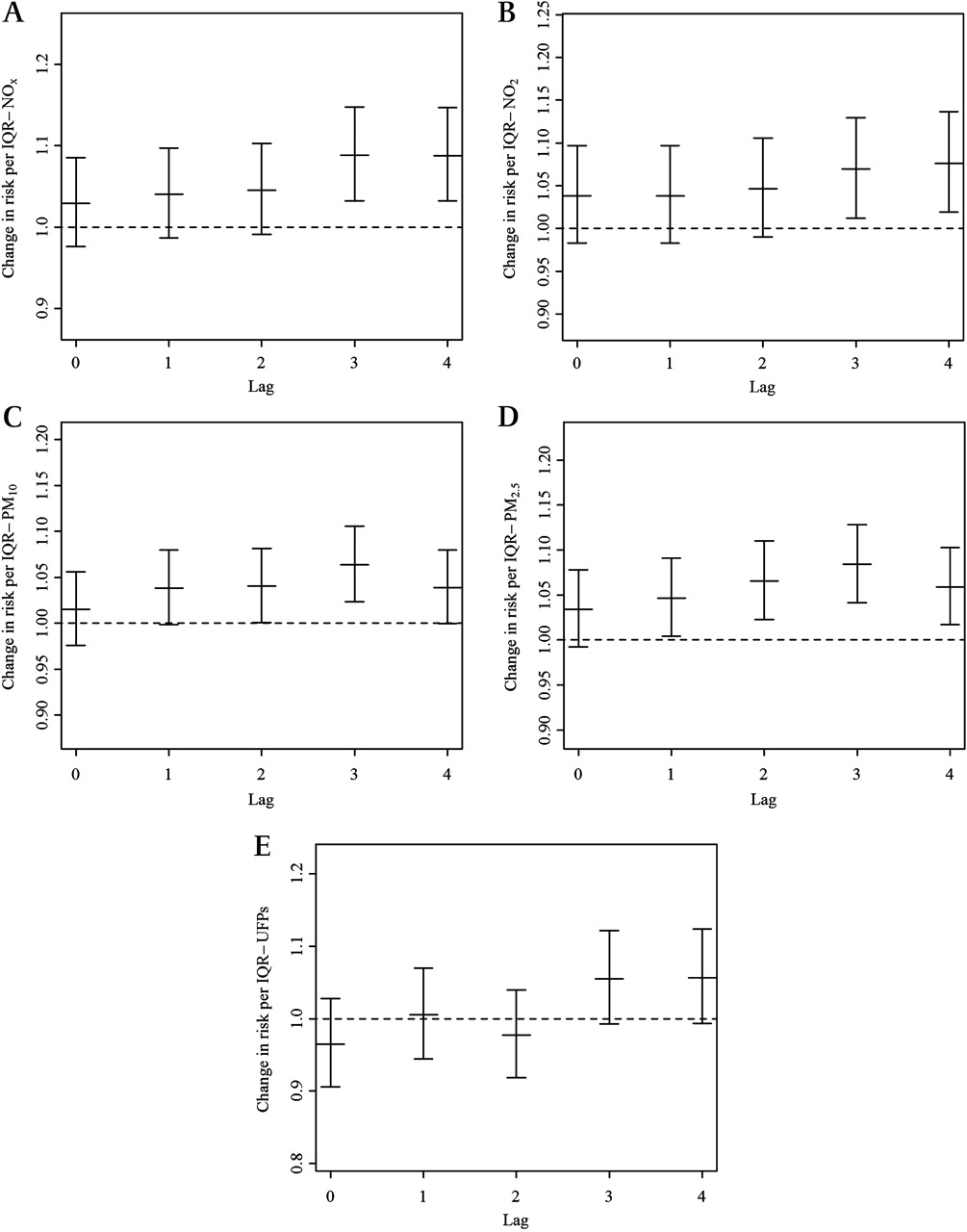
The associations between asthma admissions and single-day levels of air pollution up to 4 days prior to admission showed statistically significant associations for lag 3 (1.09; 95% CI 1.03 to 1.15 and 1.07; 95% CI 1.01 to 1.13) and lag 4 (1.09; 95% CI 1.03 to 1.15 and 1.08; 95% CI 1.02 to 1.14) for NOx and NO2, for lag 2 (1.04; 95% CI 1.00 to 1.08) and lag 3 (1.06; 95% CI 1.02 to 1.11) for PM10, and lag 1, lag 2 and lag 3 for PM2.5, with the strongest association at lag 3 (1.09; 95% CI 1.04 to 1.13) (figure 2). No significant association was found between any single-day levels of UFPs and asthma admission.
{kind=link}
{kind=link}
Effect estimates with 95% CI of risk of asthma exacerbation per increase in interquartile range (IQR) for (A) nitrogen oxides (NOx), (B) nitrogen dioxide (NO2), (C) particulate matter with an aerodynamic diameter ≤10 μm (PM10), (D) particulate matter with an aerodynamic diameter 2.5 μm (PM2.5) and (E) ultrafine particles (UFPs). The effect estimates are calculated for lags between zero and 4 days in air pollution.
Higher effect estimates of exposure to NOx, NO2, and PM2.5 were observed for hospital admissions for asthma in boys, but no statistically significant difference was detected between genders (table 2). The effects of exposure to PM10 and UFPs on hospital admissions for asthma were identical in boys and girls. We did not detect significant modification of the effect of air pollution on hospital admissions for asthma by age, but we found a stronger association in infants than in preschool and school children which was consistent for all pollutants.
We found slightly attenuated effects but statistically significant positive associations between hospital admissions for asthma and NOx, NO2, PM2.5 and PM10 without wind speed in the model (see table E3 in online supplement). Similarly, when modelling hospital admissions for asthma with the Poisson GAM model, almost identical results were observed (see table E4 in online supplement).
Discussion
Our study showed that ambient levels of particulates PM10 and PM2.5 and gases NOx and NO2 are associated with childhood hospital admissions for asthma in Copenhagen with an increase in the rate of admission of approximately 10% per IQR increase in air pollution levels.
We found no association between asthma admissions and UFPs, suggesting that adverse effects of acute exposures to air pollution on airways in children are more likely mediated by larger particles and/or gases. We previously studied similar exposures in the Copenhagen Prospective Study on Asthma Birth Cohort and found that several days of exposure to NO2 and NOx triggered episodes of ‘wheezing’ in infants born to mothers with asthma,20 whereas no significant association was detected with UFPs. Another Danish study of hospital admissions in school children (5–18 years) detected an association of borderline significance with PM2.5 and weaker and non-significant associations with UFPs.15 The effects associated with UFPs in both studies were similar and slightly stronger than those observed with PM10,15 20 but the study with hospital admissions showed that PM2.5 and not UFPs mediated the effect of particles.15 Both of these studies with follow-up until 2004 were limited by a large number of missing data on UFPs which were first available in Denmark in May 2001. In the present study on hospital admissions in children aged 0–18 years and UFP data from 2001 to 2008, we found that hospital admissions for asthma were triggered by several days' exposure to larger particles PM10 and PM2.5 but not to UFPs. This finding is in agreement with a study reporting acute effects of PM10 but no effect of UFPs on peak expiratory flow in children aged 7–12 years with asthma.21 Similarly, a study in dogs failed to detect an effect of acute exposure to UFPs on airway reactivity or immune response.24 On the other hand, three studies in adults with asthma showed that respiratory effects related to air pollution were mediated by UFPs and not by larger particles.24 25 Overall, the evidence regarding the effects of UFPs on asthma is limited and conflicting, warranting more research.
The main limitation of this study is the assessment of air pollution exposure from a single background monitor as a proxy for personal exposure. Depending on the traffic intensity, wind direction and speed and building topography, the concentration of pollutants can vary considerably between sites within a city. The resulting exposure misclassifications introduce bias into our analysis which is not possible to quantify owing to lack of information on personal exposure. Furthermore, it can be argued that exposure misclassification may be larger for UFPs than for larger particles,15 which may explain the lack of association with this fraction of particulate matter. A 15 km radius from the central urban background measurement station represents the municipality limits of Copenhagen City with a similar population and traffic density and is assumed to be representative of air pollution levels measured at the central urban background measurement station. We have previously shown that the levels of UFPs at this site correlate well with the levels at a monitoring site at the kerbside (2 m height) of a busy street 3000 m away (Spearman correlation coefficient (RS)=0.62) and a rural monitoring site located in an agricultural area 30 km west of Copenhagen (RS=0.80).15 This indicates that the daily oscillations in traffic-related air pollutants on busy streets due to variation in traffic intensity, weather conditions and other factors are also reflected by urban background monitoring, and that a radius of 15 km from the background monitor is reasonable for the assessment of daily variations in population exposure. However, in the same study we showed that correlation between measurements of the urban background (20 m) and kerbside (2 m) monitor was lower for UFPs (RS=0.62) than for PM2.5 (RS=0.86) and PM10 (RS=0.65) and was lowest for the smallest fractions of UFPs,15 implying larger exposure misclassification for UFPs than for larger particles, and probably a larger bias towards zero in UFP effect estimates. We therefore cannot exclude the possibility that the lack of effect of UFPs in this study is due to differential exposure misclassification. On the other hand, we have earlier linked exposure to the same UFP data (and not with larger particles) in Copenhagen to hospital admissions for stroke in the same nine hospitals using the same epidemiological design (within 15 km radius from the central measurement station).26
Various factors may modify the effect of air pollution on asthma. No significant evidence for effect modification by gender or age was found. However, boys seemed to be slightly more susceptible to outdoor air pollution than girls, since the risk estimates related to NOx and PM2.5 are higher. The effects of exposure to air pollution on asthma exacerbations are suggested to be stronger in children than in adults,4 as corroborated by two studies17 27 but not confirmed by a study reporting similar effects for children (3–15 years) and adults (15–49 years).10 Seasonality and associations with air pollution of asthma admissions in children have been shown to vary with age,12 showing the highest association with hospital admission rates for asthma among the youngest children (<2 years). One study found a stronger association between hospital admissions for asthma and air pollution in school children (age 6–18 years) than in preschool children (age <6 years)17 whereas, in our earlier birth cohort study, greater effects of air pollution on wheezing were seen in infants (aged 0–1 years) than in children aged 2–3 years.19 Other studies did not assess the susceptibility to air pollution by age.11 13–16 19
The strengths of our study include the long time series of daily measurements of UFP data (2001–8) which made it possible, for the first time, to investigate the association between UFPs and hospital admissions for asthma. A further strength of our study is the high quality of the hospitalisation register data derived from the DNPR. A validity study of DNPR data on asthma diagnoses in children aged 6–14 years showed that data on discharge asthma diagnoses were correct in 91% of cases, with medical records serving as the gold standard.28 Furthermore, the use of a time-stratified case crossover design minimises the effects of long-term seasonal trends and serial autocorrelation in the data and provides for full adjustment for confounders. We adjusted for possible effects of seasonal and long-time trends in air pollution levels or hospital admissions for asthma in the case crossover design by matching the air pollution level on the day of admission to hospital for asthma with the levels on the same weekday in the same month. Similarly, in time-series analyses (see online supplement), we modelled the calendar time by restricted cubic spline and thus adjusted for seasonal and long-varying trends. Finally, our findings were robust to a different modelling approach, using a time-series analysis with the GAM which used a different model of meteorology and long-term trends (see table E4 in online supplement). The risk of hospital admission for asthma using GAM was estimated to be 10% (95% CI 5% to 16%) per IQR increase for NOx (see table E4 in online supplement). The GAM analysis also indicated that infants were more sensitive to air pollution than preschool children and school children.
Our study also has some limitations. Caution should be taken when interpreting results from two-pollutant models with PM10 and PM2.5 (correlation coefficient r=0.93) as well as NOx and NO2 (r=0.85) as the effect estimates of these highly correlated variables may be artifacts of colinearity. Furthermore, the air pollution data were measured at a single background monitoring station and there were no residential or school and kindergarten addresses. Finally, we cannot exclude the possibility that the lack of effect of exposure to UFPs in this study is due to a potentially larger measurement error in UFP data than in data on larger particles and gases, and thus higher exposure misclassification for UFPs which would bias estimates towards zero.
Conclusions
Short-term exposure to ambient air pollution increases the risk of admission to hospital for asthma among children. Gases (NOx and NO2) and coarse and fine particles (PM2.5 and PM10) mediate the adverse effects whereas UFPs have no effect.
References
Supplementary materials
Web Only Data thoraxjnl-2011-200324
Files in this Data Supplement:
Footnotes
Funding COPSAC is funded by private and public research funds all listed on http://www.copsac.com. The Lundbeck Foundation, the Pharmacy Foundation of 1991, Augustinus Foundation, the Danish Medical Research Council and the Danish Paediatric Asthma Centre provided core support for COPSAC. Measurements of air pollution and meteorology have been funded by the Danish Environmental Protection Agency and via the Danish air quality monitoring programmes. The funding agencies did not have any role in study design, data collection and analysis, decision to publish or preparation of the manuscript.
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Airwaves