Article Text

Statistics from Altmetric.com
- Asthma
- asthma pharmacology
- paediatric asthma
- exhaled airway markers
- respiratory measurement
- asthma epidemiology
- asthma mechanisms
The clinical efficacy of inhaled corticosteroids (ICSs) in asthma has been demonstrated in long-term intervention studies,1 2 and ICSs are recommended first-line treatment of persistent asthma, even in children.3 The long-term benefits of early intervention with ICS have been well documented in adults with asthma.4 In children, early intervention with ICS has not altered the natural history of the disease.1 We have recently finalised a series of studies related to the Helsinki Early Intervention Childhood Asthma Programme.5 The programme highlights the benefits and safety aspects of intermittent treatment with an ICS, budesonide, in comparison with continuous daily ICS and non-steroidal maintenance treatment. In this study, we summarise our experiences.
In the 18-month intervention, we compared two budesonide regimens with a control group treated with a fixed dose of disodium cromoglycate (DSCG). The study evaluated the antiasthmatic efficacy and systemic effects of daily versus as-needed intermittent budesonide in prepubertal children with mild persistent asthma. The efficacy variables were morning peak expiratory flow, FEV1, the number of asthma exacerbations and asthma-free days. The indicators of systemic effect were standing-height velocity, bone mineral density (BMD), skin thickness, intraocular pressure and the occurrence of lens opacities.
Children aged 5–10 years (n=176) with newly detected asthma were randomised into three treatment groups: (1) continuous budesonide (400 μg twice daily for 1 month, 200 μg twice daily for months 2–6 and 100 μg twice daily for months 7–18), (2) budesonide, identical treatment to group 1 during months 1–6, then placebo as regular treatment and budesonide intermittently for exacerbations during months 7–18 and (3) DSCG 10 mg three times daily for months 1–18. Exacerbations were treated with budesonide 400 μg twice daily for 2 weeks. If an oral or parenteral corticosteroid was needed, the child was withdrawn from the study.
The use of a relatively high-dose budesonide for the initial 6 months was based on our pilot study showing that treatment with inhaled budesonide rapidly decreases sputum eosinophils along with clinical and functional improvements.6
No significant differences were observed between the groups in morning peak expiratory flow at any time point. After 6 months of treatment, improvements in FEV1 in litres were significantly greater in the two budesonide groups than in the DSCG group. However, from baseline to 18 months, no significant differences in FEV1 were observed.5
For the 18-month study period, 364 asthma exacerbations were recorded in 133 patients (2.07 exacerbations per patient in the study). During the first 6 months of treatment, children receiving budesonide had significantly less exacerbations than the children in the DSCG group. During months 7–18, the continuous budesonide group (ie, children on low-dose budesonide) had significantly fewer exacerbations (0.97 per patient) than the intermittent ICS group (1.69 per patient, see figure 1A).5

{kind=link}
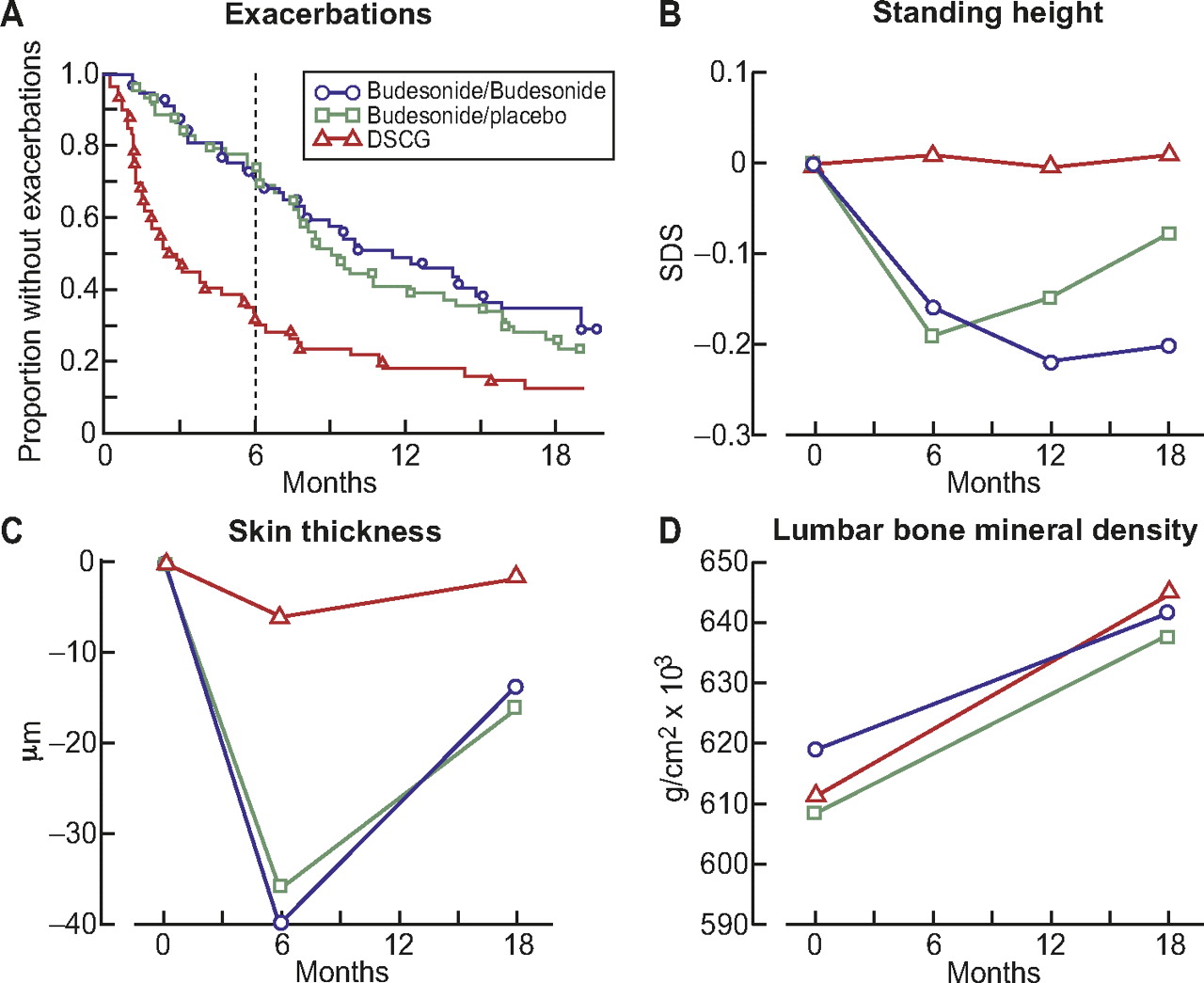
Major findings of the Helsinki Early Intervention Childhood Asthma Study. (A) The median time to the first exacerbation was significantly longer for both the continuous budesonide and the budesonide/placebo groups compared with the DSCG group (p<0.001 for both). After 6 months (vertical line), the median time to the next exacerbation was still significant between the continuous budesonide and DSCG groups (p=0.03).5 (B) Mean changes in standing height (SDS). For months 1–6, both budesonide groups versus DSCG group (p<0.001); for months 7–18, continuous budesonide versus budesonide/placebo group (p=0.016).5 (C) Changes in skin thickness (μm) of the right forearm. At 6 months, the difference between the budesonide groups combined and the DSCG group was significant (p=0.004).16 (D) The changes in lumbar BMD during 18 months as g/cm2. A larger increment in BMD was found in the DSCG than in the continuous budesonide group (p=0.021). The increment was intermediate in the budesonide/placebo group.15
At 6 months, the mean number of symptom-free days increased more in the two budesonide groups than in the DSCG group. During months 7–18, the symptom-free days did not differ between the continuous budesonide group and the intermittent group.5
From baseline to 6 months, the mean standing-height velocity in the two budesonide groups was 2 cm/year slower than in the DSCG group (figure 1B). From 7 to 18 months, height velocity increased in both budesonide groups. The mean height velocity was greater in the intermittent treatment group than in the continuous budesonide group (6.2 vs 5.6 cm; p=0.016), suggesting catch-up of the initial loss in standing height. After 18 months of treatment, children receiving DSCG had grown on average 1.0 cm more than children in the continuous budesonide group and 0.6 cm more than children in the intermittent budesonide group.
The height velocity in asthmatic children is influenced by normal developmental factors such as seasonal variation, delay in growth spurt, disease severity and the use of corticosteroids.7 8 A meta-analysis of children receiving oral or ICS therapy revealed a significant tendency for corticosteroid therapy to reduce final height.9 To minimise confounding factors, our study dealt with prepubertal children treated with ICS but with no oral or parenteral steroids. Interruption of regular maintenance ICS treatment may be necessary to reduce the suppressive effect of ICS on bone. This mechanism may also explain the finding in a long-term study with ICS in children, who achieved normal adult height but later than healthy subjects.10 Interestingly, in our 18-month study, the decline in height velocity was measurable, although the true adherence to treatment (recorded with a pneumotachograph) was reduced to levels around 50–60% during the study period.11
BMD increased in all treatment groups. However, at the end of the study, the regular use of budesonide had resulted in a significantly smaller increment in BMD than DSCG, calculated as grams per square centimetre and Z score (figure 1D). The increase in BMD (g/cm2) in the group receiving intermittent budesonide after the first 6 months was not different from the other two groups. When corrected for growth data, the differences in BMD data disappeared. The correlation between height and BMD suggests that following children's height might afford a good enough estimation of ICS effects on BMD.12
In adults, asthma treatment with high doses of ICSs has resulted in dermal thinning. In our study, initial 6-month budesonide treatment resulted in a greater reduction in skin thickness in the forearms compared with DSCG (figure 1C). At month 18, the intergroup differences were no longer significant. Thus, daily doses of 400 to 800 μg budesonide in prepubertal children may cause minor dermal thinning. The changes were reversible during continuous low-dose or periodic treatment.13 In adults, long-term treatment with glucocorticoids may result in posterior subcapsular cataracts and glaucoma. In the present study, the children underwent ophthalmologic examinations with lens photography and measurements of intraocular pressure before and after treatment. No case of cataract was found. Mean intraocular pressure in the two budesonide groups did not differ from that in healthy children or children treated with DSCG. With standard ICS doses, ophthalmologic examinations are not necessary except in the case of risk factors for glaucoma or elevated intraocular pressure.14
Adults without maintenance treatment for mild asthma who were instructed to initiate corticosteroid therapy according to a symptom-based action plan did not have poorer clinical or functional outcome over a year compared with those who did use regular treatment with either inhaled budesonide or oral zafirlukast.15 Furthermore, in adults with mild asthma, the symptom-driven use of inhaled beclomethasone and salbutamol in a single inhaler was as effective as regular use of inhaled beclomethasone and was associated with a lower 6-month cumulative dose of the ICS.16
In our study, lung function or asthma-free days were not different between children on regular or intermittent budesonide treatment. The maintenance low-dose budesonide afforded, however, a better control of asthma exacerbations but caused more systemic effects. Our results have been recently supported by a 44-week, randomised, double-blind, placebo-controlled trial in patients with mild persistent asthma aged 5–18 years.17 The authors suggest that ICS used as rescue together with salbutamol shows benefits over rescue β-2-agonist alone and avoids the growth effects associated with use of daily ICSs.17 The result was in line with a previous 6-month study in adults where ICS together with formoterol was more beneficial than formoterol alone in patients with intermittent asthma and signs of airway inflammation.18
In conclusion, intermittent treatment with ICS is an attractive alternative for treatment of children with mild persistent asthma. In most asthmatic children, the disease is mild.19 Most of these children are well controlled with proactive use of ICS at times of exacerbations after 6 months of regular ICS treatment. A prerequisite for successful intermittent treatment is that patients and parents understand and participate in a guided self-management programme.20 Children with frequent exacerbations, as judged by a follow-up of 12 months, should have regular maintenance therapy. The benefits of daily therapy in these children outweigh any potential adverse effects and risks associated with poorly controlled asthma.21
Our results were obtained with budesonide, and efficacy/safety profiles with different ICS treatments are drug and dose dependent. The meta-analysis of Sharek and Bergman, 22 10 years ago, claimed that fluticasone slowed the growth less down than beclomethasone or budesonide. With increasing doses of fluticasone, the systemic effects may, however, seem quite significant.23 Ciclesonide seems to have little effect on growth.24 Nevertheless, our results accord the clinical experience. Most school-aged asthma children cope with intermittent ICS therapy, which also is favoured by parents and especially by those with corticosteroid fears.
References
Footnotes
Funding Helsinki University Hospital Research Grant (grant number: TYH2008302). Funder role: Academic support.
Competing interests None.
Patient consent Obtained.
Ethics approval Ethics approval was provided by Helsinki University Hospital Ethical Committee.
Provenance and peer review Not commissioned; externally peer reviewed.