Article Text

Statistics from Altmetric.com
- Radiology
- heterotopic ossification
- tuberculosis
- collapse therapy
- imaging/CT MRI etc
- thoracic surgery
- drug induced lung disease
- emphysema
- interstitial fibrosis
- lung cancer
- sarcoidosis
- systemic disease and lungs
- tobacco and the lung
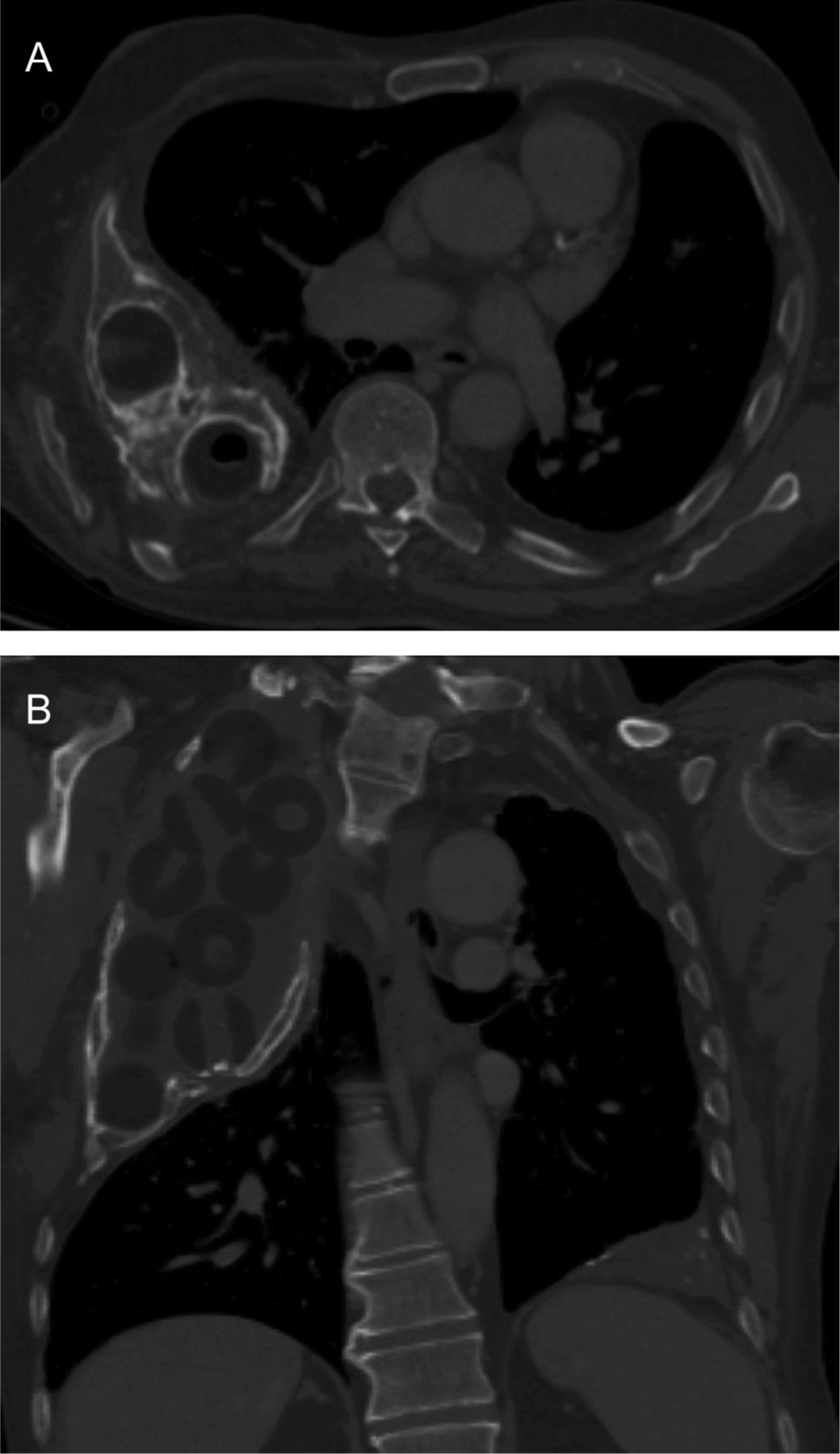
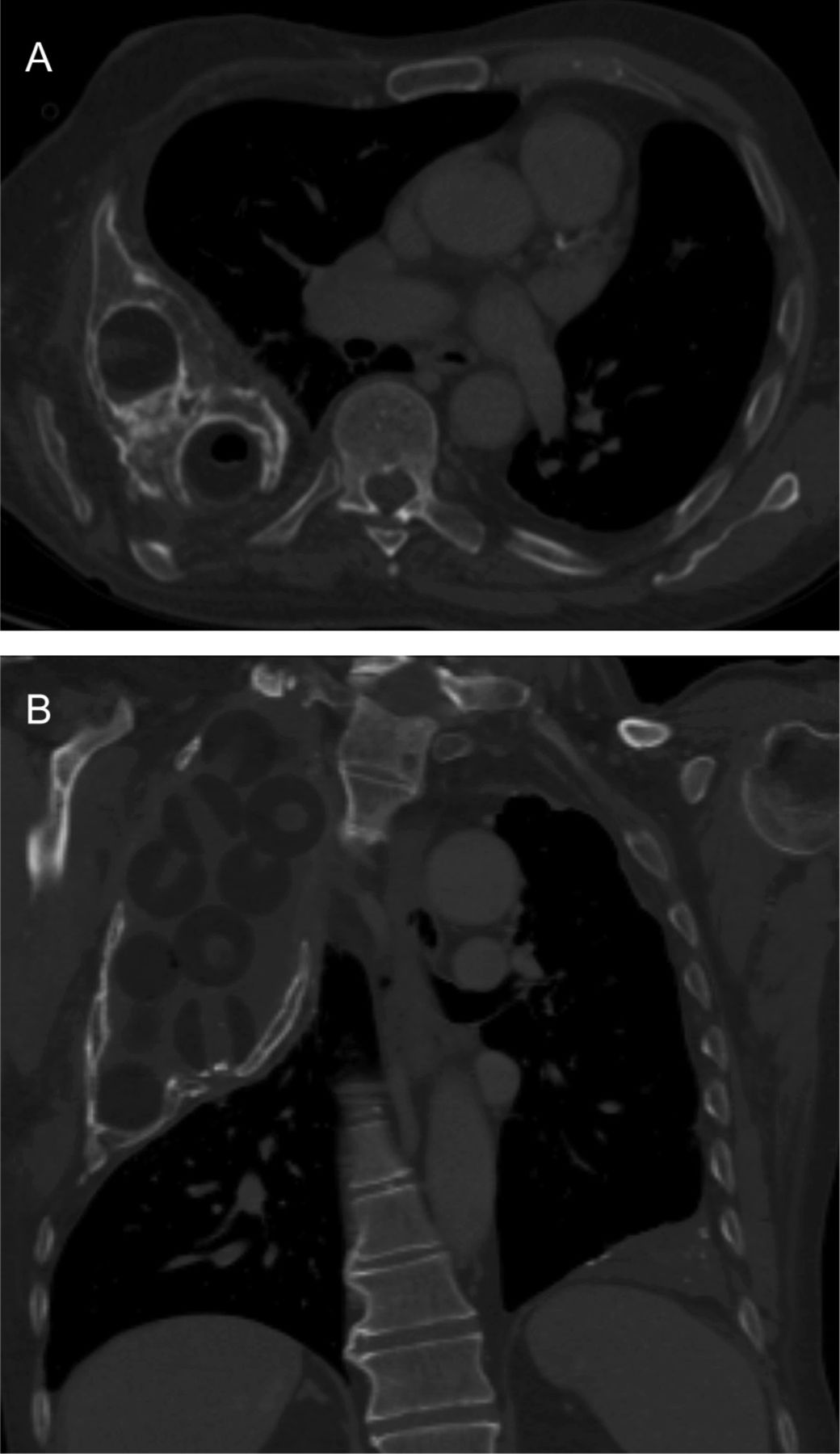
An 80-year-old patient presented with a chronic right sided chest wall sinus discharging pus. The patient had undergone an ipsilateral thoracoplasty and Lucite ball plombage for the treatment of tuberculosis in 1955, and the sinus was known to communicate with a plombage cavity. Until this presentation the sinus was uncomplicated, occasionally discharging clear fluid and a conservative approach to management was adopted. At this presentation, however, the discharge was culture positive for Staphylococcus aureus. Removal of the Lucite balls and repeat thoracoplasty using a muscle flap to fill the cavity were considered. A chest x-ray demonstrated a large right upper zone plombage cavity containing Lucite balls. The cavity appeared to be encased by a rind of abnormal bone, thought to be heterotopic ossification (figure 1). A subsequent thoracic CT demonstrated encasement of the plombage cavity by heterotopic ossification with invagination of bone between the Lucite balls (figure 2).

Chest radiograph showing right apical Lucite ball plombage with surrounding abnormal bone.
{kind=link}
{kind=link}
Axial (A) and coronal (B) chest CT images with bony window settings demonstrating abnormal corticated bone encasing the plombage cavity and invaginating around the Lucite balls.
Discussion
Heterotopic ossification is the formation of mature lamellar bone in non-ossified soft tissue. Its precise pathophysiology is unclear, but osteoblastic differentiation of pluripotent mesenchymal stem cells, often as a result of trauma or soft tissue injury, has been posited.1 This is supported by the observation that mesenchymal progenitor cells with osteogenic potential have been isolated from traumatised tissue.2 Although heterotopic calcification occurring around a plombage cavity is relatively common, to our knowledge, there are no prior reports of heterotopic ossification occurring in this setting. In our case, heterotopic ossification may have occurred in response to chronic low-grade trauma induced by the Lucite balls within the cavity or as a foreign body response to the Lucite balls themselves. Because plombage involves dissecting the periosteum and intercostal muscles away from the ribs to create the cavity, it is also possible that osteoprogenitor cells within periosteal tissue surrounding the cavity underwent osteoblastic differentiation: a complication previously reported in pedicled intercostal muscle flaps containing periosteum, which were constructed following pulmonary resection.3
Learning points
-
Extensive heterotopic ossification is a rare late complication of plombage therapy for tuberculosis.
-
CT is extremely useful in identifying this pathology and evaluating the anatomy prior to any surgical intervention.
Footnotes
-
Competing interests None.
-
Provenance and peer review Not commissioned; internally peer reviewed.
Linked Articles
- Airwaves