Article Text

Statistics from Altmetric.com
- Asthma mechanisms
- COPD pathology
- pulmonary embolism
- asbestos induced lung disease
- mesothelioma
- occupational lung disease
Case
A 58-year-old never-smoker man developed dyspnoea, cough, fevers, weight loss and tremulousness over 4 weeks. He had a brief history of asbestos exposure. Significant medical history included autosomal-dominant polycycstic kidney disease (APKD) and renal transplantation 7 years previously. He took mycophenolate mofetil and tacrolimus immune-suppressants. Examination revealed tachypnoea, a fine right arm tremor, bronchial breathing on the right and a superficial 1×2 cm non-fluctuant lump over the abdomen. Lymph nodes were impalpable.
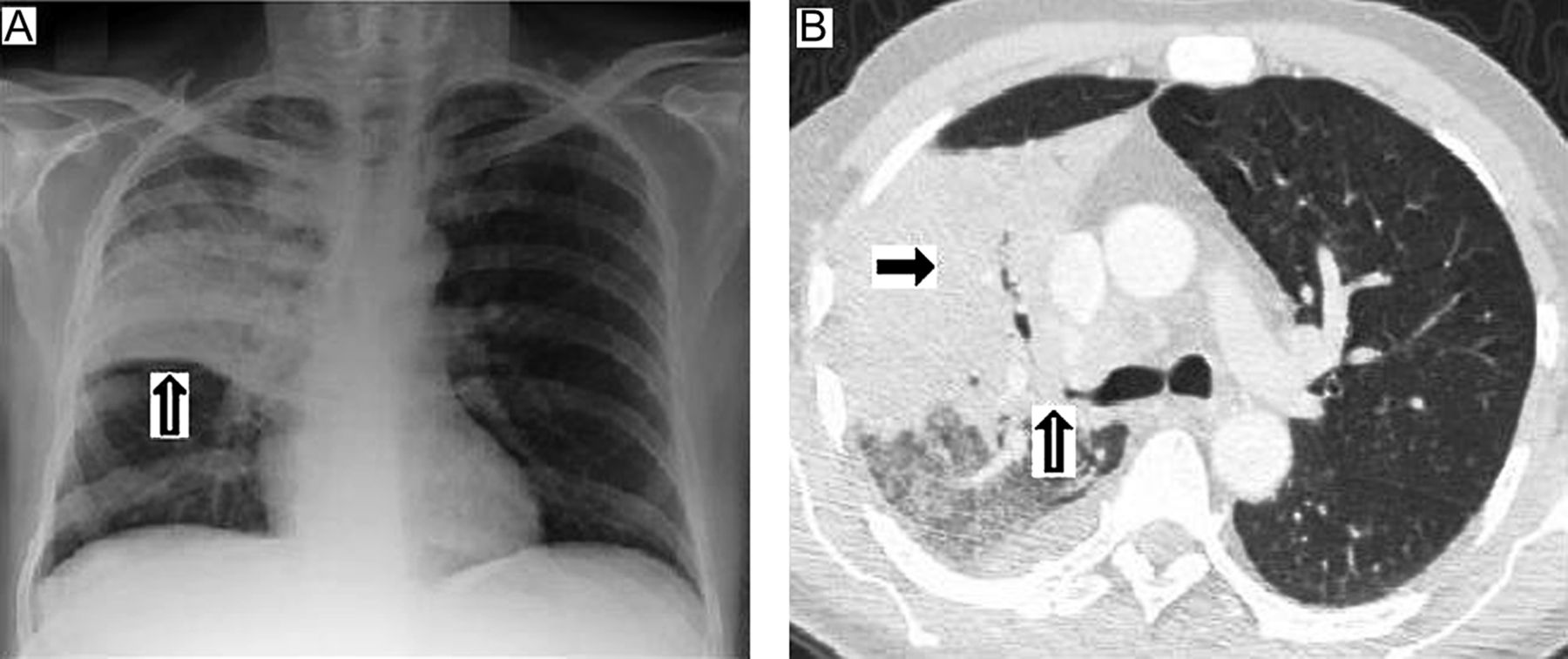
Screening blood tests showed values of c reactive protein 115 mg/l (NR <6.0), urea 25.8 mmol/l, creatinine 254 umol/l (post-transplant baseline 220–230) and tacrolimus 25.5×µg/l (NR 5–10). Autoimmune profile was negative. PCR detected cytomegalovirus (CMV) levels at 31 338 copies/ml. Plain chest radiography showed right upper lobe consolidation (figure 1A). An abdominal ultrasound scan revealed a normal transplanted kidney. Intravenous empirical antibiotics and oral valganciclovir, subsequently changed to intravenous ganciclovir, were administered.

Chest radiographic images. (A) Chest radiograph showing right upper lobe consolidation; (B) CT scan of the thorax at the level of the bifurcation of the trachea showing a 10 cm right upper lobe soft-tissue mass (black arrow) abutting the mediastinum and compressing the right upper lobe bronchus (open arrow), mediastinal lymphadenopathy (maximum 2.2 cm diameter) and a small right pleural effusion.
The clinical response was slow. CT thoraco-abdominal scans noted a right upper lobe mass (figure 1B). Fibre-optic bronchoscopy revealed widespread right-sided endobronchial ‘tumours’ (figure 2). Microbiological analysis of bronchial samples was unrevealing. Histological analysis suggested possible tuberculosis (figure 3) and antituberculous therapy was commenced, which was later stopped after PCR analysis and mycobacterium cultures proved negative.

Images at fibre-optic bronchoscopy. The arrows indicate ‘tumours’ seen at the initial fibre-optic bronchoscopy. The adjacent corresponding images were taken after 4 months of specific therapy.

{kind=link}
{kind=link}
{kind=link}
Biopsy specimen of bronchial mucosae. Some of the bronchial mucosae are ulcerated, and adjacent epithelium shows squamous metaplasia with regenerative change. The stroma is acutely inflamed (A), with evidence of acute-on-chronic inflammatory cell infiltrate in which macrophages and plasma cells are numerous. The macrophages form confluent sheet-like foci raising the possibility of a granulomatous infiltrate (B) but no multinucleated giant cells are seen. There was no evidence of lymphoma. Subsequent stains for tuberculosis (ZN stain), atypical mycobacteria (Wade Fite stain) and fungi (Grocott and PAS stains) were all negative.
Question
How would you proceed with the investigation and management?
See page 1118 for the answer
Answer
From the question on page 1116–1117.
The abdominal nodule was excised, revealing an abscess cavity. Microbiological analysis identified Gram-positive bacilli, which were confirmed as Nocardia farcinica. An MRI brain scan was normal. Linezolid and meropenem were administered. The risk of peripheral neuropathy necessitated changing linezolid (2 weeks) to co-trimoxazole, which was then changed (16 days) to oral moxifloxacin after pancytopenia occurred. There was substantial clinical improvement and renal function returned to baseline. Tacrolimus and CMV levels at 2 months were 9.7 µg/l and 2458 copies/ml, respectively. Repeat fibre-optic bronchoscopy after 4 months revealed normal bronchial epithelium (figure 2).
Nocardiae are ubiquitous environmental aerobic filamentous actinomycetes, classically Gram-positive, often acquired through inhalation and implicated in fatal opportunistic infections.1 ,2 About 500–1000 cases of nocardiosis occur annually in the USA.3 Risk factors include organ transplantation, immunosuppression, CMV infection and excess calcineurin inhibitors (ie, tacrolimus).1 Fifty to seventy per cent of cases present with suppurative and/or granulomatous pulmonary complications.4 Pulmonary tumours are a rare presentation. Secondary central nervous system (CNS) and cutaneous spread complicates 50% of patients with pulmonary nocardiosis. Interestingly, APKD is a ciliopathy, with defective primary (non-motile) cilia, although the relevance of this to pulmonary infections is unclear, where impaired motile cilia render susceptibility to chronic recurrent airways infections.
Nocardiae are weakly acid fast, which aids their distinction from other actinomycetes. Their structure and other additional tests distinguish them from mycobacteriae. Species identification with antimicrobial susceptibility analysis is recommended. N farcinica is especially aggressive and resistant to many antibiotics.2 Sulphonamides, often as co-trimoxazole, form the cornerstone of empirical therapy, but mortality in disseminated nocardiosis is 50–85%.2 Combination therapy, often with amikacin, ceftriaxone, imipenem, minocycline and recently linezolid, is recommended.2 ,5 The duration is dictated by underlying immunosuppression and CNS disease. Immunocompetent hosts without CNS involvement require 6 months of therapy; those with CNS involvement or immunocompromised patients require at least 12 months of therapy.5 All these cases require monitoring for recurrence for at least 1 year.5 Immunocompromised patients may benefit in the long term from prolonged low-dose maintenance therapy.5
Acknowledgments
We would like to thank the patient concerned for giving us his consent to write this article.
Footnotes
-
Competing interests None.
-
Patient consent Obtained.
-
Ethics approval Since this paper is a case report rather than a study, consent was obtained from the patient concerned, who is anonymised in the report.
-
Provenance and peer review Not commissioned; externally peer reviewed.