Article Text

Abstract
Rationale and objectives Impaired insulin sensitivity (ISx), increased visceral abdominal fat (VAF) and liver fat are all central components of the metabolic syndrome and characteristics of men with obstructive sleep apnoea (OSA). The reversibility of these observed changes with continuous positive airway pressure (CPAP) treatment in men with OSA has not been systematically studied in a randomised sham-controlled fashion.
Methods 65 men without diabetes who were CPAP naïve and had moderate to severe OSA (age=49±12 years, apnoea hypopnoea index (AHI)=39.9±17.7 events/h, body mass index=31.3±5.2 kg/m2) were randomised to receive either real (n=34) or sham (n=31) CPAP for 12 weeks. At 12 weeks, all subjects received real CPAP for an additional 12 weeks.
Measurements and main results Main outcomes were the change at week 12 from baseline in VAF, ISx and liver fat. Other metabolic outcomes were changes in the disposition index, total fat, and blood leptin and adiponectin concentrations. The AHI was lower on CPAP compared with sham by 33 events/h (95% CI−43.9 to −22.2, p<0.0001) after 12 weeks. There were no between-group differences at 12 weeks in VAF (−13.0 cm3, −42.4 to 16.2, p=0.37), ISx (−0.13 (min−1)(μU/ml))−1, −0.40 to 0.14, p=0.33), liver fat (−0.5 cm3, −3.8 to 2.7, p=0.74) or any other cardiometabolic parameter. At 24 weeks, ISx (3.2×104 (min−1)(μU/ml))−1, 0.9×104 to 6.0×104, p=0.009), but not VAF (−1.4 cm3, −19.2 to 16.4, p=0.87) or liver fat (−0.2 Hounsfield units, −2.4 to 2.0, p=0.83) were improved compared with baseline in the whole study group.
Conclusion Reducing visceral adiposity in men with OSA cannot be achieved with CPAP alone and is likely to require weight-loss interventions. Longer-term effects of CPAP on other cardiometabolic markers such as ISx require further investigation to fully examine time dependencies.
Trial Registration Number ACTRN12608000301369.
- Obstructive sleep apnoea
- intra-abdominal fat
- insulin resistance
- continuous positive airway pressure
- clinical epidemiology
- oxidative stress
- sleep apnoea
Statistics from Altmetric.com
- Obstructive sleep apnoea
- intra-abdominal fat
- insulin resistance
- continuous positive airway pressure
- clinical epidemiology
- oxidative stress
- sleep apnoea
Introduction
Obstructive sleep apnoea (OSA) is a common disorder that affects up to 25% of adult men.1 Untreated severe OSA increases the risk of all-cause and cardiovascular mortality.2–4 It is generally believed that these increased risks are partly due to obesity, increased visceral abdominal fat (VAF), insulin resistance (IR) and increased liver fat.5 This is because VAF, liver fat and IR (central components of the metabolic syndrome) are all independently associated with increased risk for cardiovascular disease and mortality in adults not selected for OSA.6–8 Furthermore, long-term CPAP treatment decreases mortality risk,9 but whether this is due to CPAP-induced improvements in IR or body fat distribution, including decreases in VAF and liver fat, has not been systematically studied. Indeed, the reversibility of IR, VAF and liver fat in OSA is still not known because few randomised controlled CPAP intervention studies have been performed.
Key messages
What is the key question?
-
Does continuous positive airway pressure therapy, as practically applied in the community, improve central parameters of cardiometabolic risk in men with obstructive sleep apnoea?
What is the bottom line?
-
We found that CPAP may improve insulin sensitivity but does not decrease visceral adiposity or liver fat by 24 weeks.
Why read on?
-
Our results are of relevance to sleep medicine physicians who now cannot rely solely on CPAP therapy to improve cardiometabolic health. Weight loss interventions are likely to be needed to reduce visceral adiposity in men with obstructive sleep apnoea.
Randomised studies investigating the effect of CPAP on VAF or liver fat are not yet available. However, we10 and others11 previously reported significant reductions in VAF volume after 3 and 6 months of CPAP treatment respectively, although other studies did not detect such changes.12–14 A single long-term (2–3 years) uncontrolled study showed that CPAP reduced liver fat but only in those who were CPAP compliant (n=6).15 Randomised controlled trials are required to fully address the question of whether CPAP alters VAF and liver fat.
Three randomised sham-controlled trials have examined the effect of CPAP therapy on IR, but the results are inconclusive. Only one of the three studies reported a statistically significant improvement in IR, but the controlled portion of this study was of 1 week duration, so that the durability of these findings is not known.14 The other two studies did not show any change in IR with CPAP. However, one was performed specifically in diabetic men in whom the extent of reversibility may be limited16 and the other did not assess insulin resistance by a sensitive method.17 Additionally none of these three studies examined other important measures of glucose metabolism such as the disposition index (DI), a measure which combines impaired β-cell activity with IR18 and is useful in predicting future diabetes.19 Furthermore, the important inter-relationships among VAF, liver fat and IR have not been investigated because no randomised controlled trial has measured all of these important biomarkers concurrently.
We therefore undertook a randomised sham-controlled trial to determine the effects of 12 weeks of CPAP treatment on VAF and liver fat (CT scans), insulin sensitivity (ISx) and DI (from minimal model analysis) in men with OSA without known diabetes. We also measured total body fat and muscle mass (whole body dual-energy X-ray absorptiometry (DEXA) scans), leptin and adiponectin concentrations. All subjects received an additional 12 weeks of open-label CPAP treatment after which all outcomes were remeasured.
Methods
Setting and participants
Participants were recruited from tertiary referral sleep clinics at Royal Prince Alfred Hospital and the Woolcock Institute of Medical Research, Sydney, Australia between July 2008 and December 2010. Eligible participants were adult men with moderate–severe OSA, defined as aged ≥18 years, an apnoea hypopnoea index (AHI) ≥20 events/h and an oxygen desaturation index 3% ≥15 events/h measured by in-laboratory polysomnography (PSG). Participants were excluded if they had diagnosed type II diabetes mellitus; previously used CPAP treatment; minimum oxygen saturation <65% or an AHI >80 events/h or required immediate CPAP treatment due to excessive sleepiness in relation to the subject's occupation; uncontrolled concurrent medical, drug abuse or psychiatric illness; contraindication to CPAP therapy; irregular sleep patterns such as shift workers; or participation in another clinical trial in the previous 30 days.
Design overview
This was a randomised, double-blind, sham-controlled, parallel-group study. Following baseline data collection, eligible participants were randomised to receive either real or sham CPAP for 12 weeks. Clinical assessments were performed before, midway at 6 weeks, and after treatment. At the end of the 12-week blinded period all participants were provided with open-label real CPAP for an additional 12 weeks. Assessments were recollected at 24 weeks.
The study complied with Good Clinical Practice guidelines, applicable regulatory requirements and the Declaration of Helsinki. All participants provided written informed consent to participate in the study, which was approved by the Sydney South West Area Health Service Human Research and Ethics Committee (RPAH Zone). The study is registered with the Australia New Zealand Clinical Trials Network, http://www.anzctr.org.au, number ACTRN12608000301369.
Randomisation, allocation concealment and blinding
A computer programme produced randomised permuted blocks with a block size of four. Participants were assigned to real or sham CPAP in a 1:1 ratio. At baseline each participant was assigned a unique number in sequential, ascending, chronological order which corresponded to the treatment allocation. Machine preparation was performed by a person separate to the study investigators and not involved in participant assessments. The study investigators were blinded to treatment allocation for the duration of the study. During the open-label period both the participants and study investigators remained blinded to the initial treatment allocation.
Outcomes
The predefined primary outcome was the change in VAF from baseline to week 12. The main predefined secondary outcome was the change in ISx from baseline to week 12. Other secondary outcomes were the changes from baseline to week 12 in liver fat, body composition (weight, body mass index (BMI), waist circumference, abdominal subcutaneous fat, total fat and lean mass) and metabolic markers (DI, homeostasis model assessment (HOMA), quantitative insulin sensitive check index (QUICKI), fasting glucose and insulin, leptin and adiponectin). We also assessed the change from baseline to week 24 in all measures.
CPAP machines and titration
The real and sham CPAP machines (Remstar Auto, Philips Respironics, Murrysville, Pennsylvania, USA) were identical in appearance to each other and have been used previously at our centre20 and by others.21 The sham device delivered airflow with minimal pressure (0.5 cm H2O). Prior to randomisation every subject was fitted with a mask and received a standard CPAP education programme operating in our clinic. Compliance data were recorded by an internal clock within all real and sham CPAP machines and were downloaded after the home titration and at each visit. Further details are available in the online supplement.
PSG and sleepiness
Sleep and breathing were assessed by attended overnight, in-laboratory PSG (Sandman Elite V.9.2, Tyco Healthcare, Denver, Colorado, USA). A standard diagnostic PSG was performed at week 0. At weeks 12 and 24, standard PSGs were recorded in all participants irrespective of whether the participant was using real or sham CPAP. Subjective sleepiness was measured by the Epworth Sleepiness Scale (ESS)22 at all visits. Further details are available in the online supplement.
VAF and body composition
VAF and subcutaneous fat were measured by CT (16-slice light speed extra; GE Healthcare, Madison, Wisconsin, USA). The volumes of VAF and subcutaneous fat were calculated using a validated software tool (Hippofat; CNR Institute of Clinical Physiology, Pisa, Italy)23 from two 10 mm contiguous CT images of the lower abdomen, at the level of the umbilicus, between the L4 and L5 vertebra. Liver fat, estimated by liver and spleen Hounsfield unit (HU) attenuations (E-FILM, Merge Healthcare, Milwaukee, Wisconsin, USA) was quantified from unenhanced CT slices by a previously published method.24 Total fat and muscle mass were measured by total body DEXA (Lunar Prodigy; GE Healthcare). All scans were performed at 0, 12 and 24 weeks. Anthropometric measurements were also recorded using standardised techniques at each visit by a single observer.25
Measures of metabolic dysfunction
ISx and the DI were calculated by minimal model.26 Venous blood samples were collected via a cannula following an overnight fast and a standard 3-day carbohydrate-loaded diet at 0, 12 and 24 weeks. A fasting blood sample was first collected and then at 10, 20, 30, 60, 75, 90 and 120 min after a 75 g/300 ml oral glucose load following an established protocol.26 Additionally fasting samples were collected at 0, 6, 12, 24 weeks and the HOMA27 and QUICKI28 were calculated. Glucose, insulin, C peptide, leptin and adiponectin concentrations were all measured with commercially available assays. All samples were stored at −80°C for subsequent batched analysis and all samples from an individual patient were run within a single assay.
Statistical analysis
The study was powered to detect a standardised mean change in VAF of 0.78±1 using our previously published data.10 The total sample size (assuming 1:1 randomisation) required to detect this effect with 80% power at a two-tailed significance level of 5% was 52 men treated for 12 weeks.
The outcome variables were the calculated differences from baseline at 6, 12 and 24 weeks. Linear regression was used to determine between-treatment group differences of these calculated differences from baseline during the blinded period (6 and 12 weeks). Mixed model analysis was used for outcomes with repeated measurements. Further analyses explored the influence of treatment compliance, baseline severity (AHI), obesity (BMI and waist circumference) and sleepiness (ESS). These potential confounders were included as linear covariates. Additionally covariates with predefined cut points were included in separate mixed models as a dichotomised factor (compliance 4 h/night; AHI 30 events/h; BMI 30 kg/m2; ESS 10). The statistical significance of the interaction terms of treatment and each dichotomised variable were examined. These analyses were performed to assess whether the effect of CPAP was influenced by compliance, baseline AHI, obesity or sleepiness. Pooled mean changes and the SE of the mean from baseline to week 24 were determined regardless of initial treatment allocation. Unpooled mean changes are also shown and analysed analogously.
Analyses were performed using SAS V.9.2 (SAS Institute). Data were considered significantly different at p<0.05 (two sided) and are presented as mean differences (95% CI), mean (SD), or median (IQR) as indicated.
Results
The flow of participants through the study is shown in figure 1. Sixty-nine men were enrolled of whom 65 were randomised to receive either real (n=34) or sham (n=31) CPAP treatment. Four participants could not complete home titration after multiple attempts and two other participants withdrew for personal reasons prior to starting real or sham CPAP (figure 1). Primary outcome data were available for 52 men at week 12 and 46 men at week 24. Baseline characteristics were comparable in the two treatment groups (table 1). The withdrawn subjects were comparable to those who completed, except for a significantly lower CPAP adherence rate (data not shown). None of the participants had physician-diagnosed diabetes at baseline, 92% were overweight, 70% had abdominal obesity and 55% were medically obese. Two participants without diagnosed diabetes during screening were randomised, and subsequently discovered to have diabetes after analysis of the oral glucose tolerance test at the end of the study.29 The analyses were performed with and without these participants and there was no difference in findings. All findings presented here are of all participants with available data.
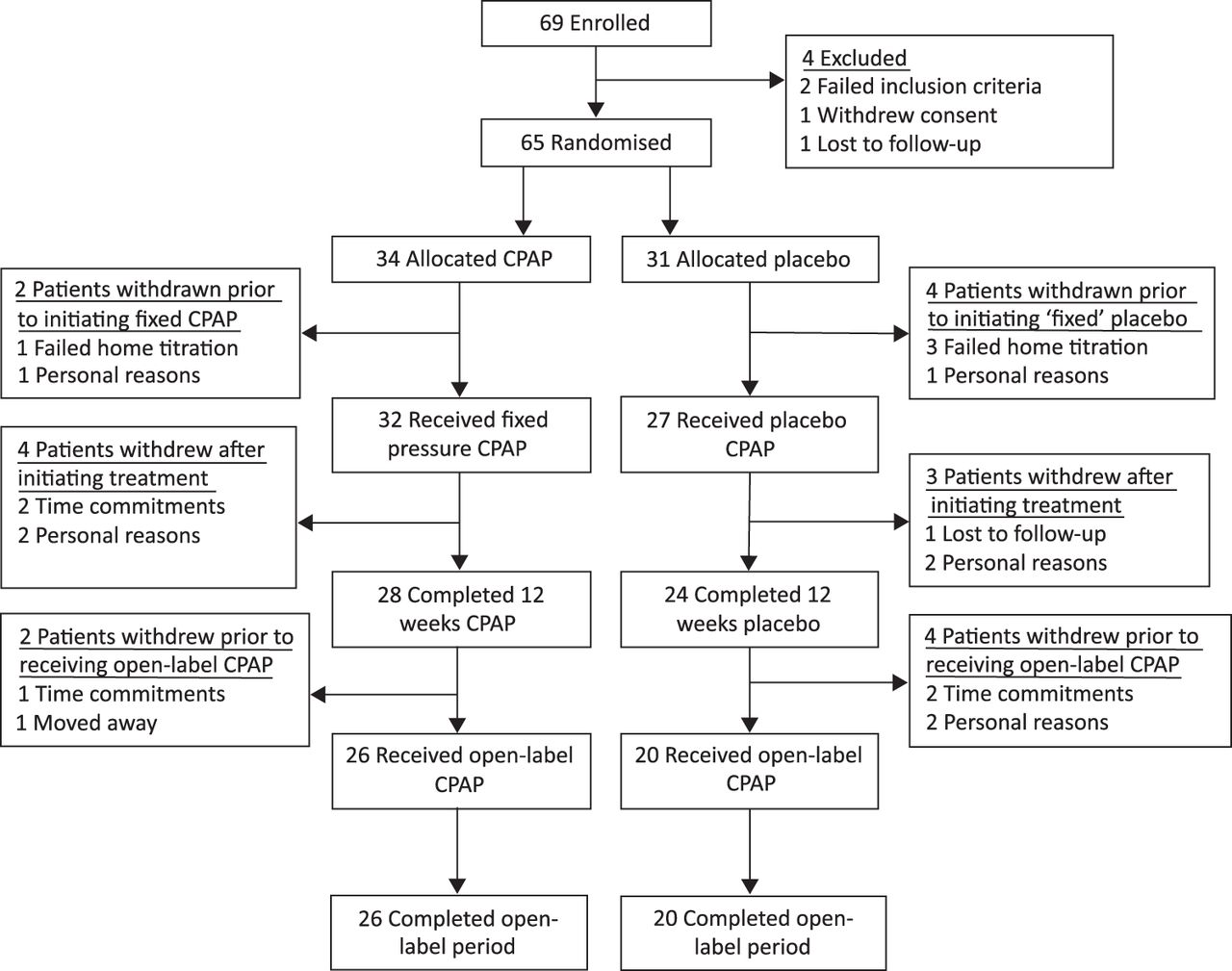
Study flow. CPAP, continuous positive airway pressure.
Baseline participant characteristics
During the blinded period, real CPAP use was 3.6 h per night and sham CPAP use was 2.8 h per night (p=0.07). During the open-label period, CPAP use was 4 h per night for both groups (p=0.72). CPAP use did not change during the open-label period in those initially randomised to CPAP therapy (p=0.16) but increased by 1.1 h in those initially randomised to sham therapy (p=0.04). All participants with available data, regardless of CPAP use, were included in the analysis.
The change in VAF or any other measurements of body composition at week 12 were not significantly different between groups (figure 2). At week 12 there was a within-group increase in lean muscle mass in the CPAP group (p=0.001) compared with a non-significant change after sham treatment (p=0.20). At week 24, lean muscle had increased in all participants but there were no changes in any other measures of body composition (figure 2 and table 3). Furthermore, the actual decrease in VAF at week 24 was 1.4 cm3 which corresponds to a standardised mean change in VAF of 0.08±1 (table 3).

Plot of mean and SE of the mean for (A) visceral abdominal fat (VAF), (B) subcutaneous abdominal fat (subcut), (C) liver fat, (D) the liver to spleen ratio (L/S ratio), (E) total body fat and (F) total lean mass. The left-hand plot (line graph) shows the mean change at week 12 from baseline for the real continuous positive airway pressure (CPAP) (filled circles) and sham CPAP (open circles) groups. The p value above this graph denotes the between-group difference as determined by linear regression. The right-hand plot (vertical bar graph) is the pooled mean change at week 24 from baseline in all participants regardless of initial treatment allocation. The p value above this graph denotes the significance of the change as determined by Student's t test. HU, Hounsfield unit.
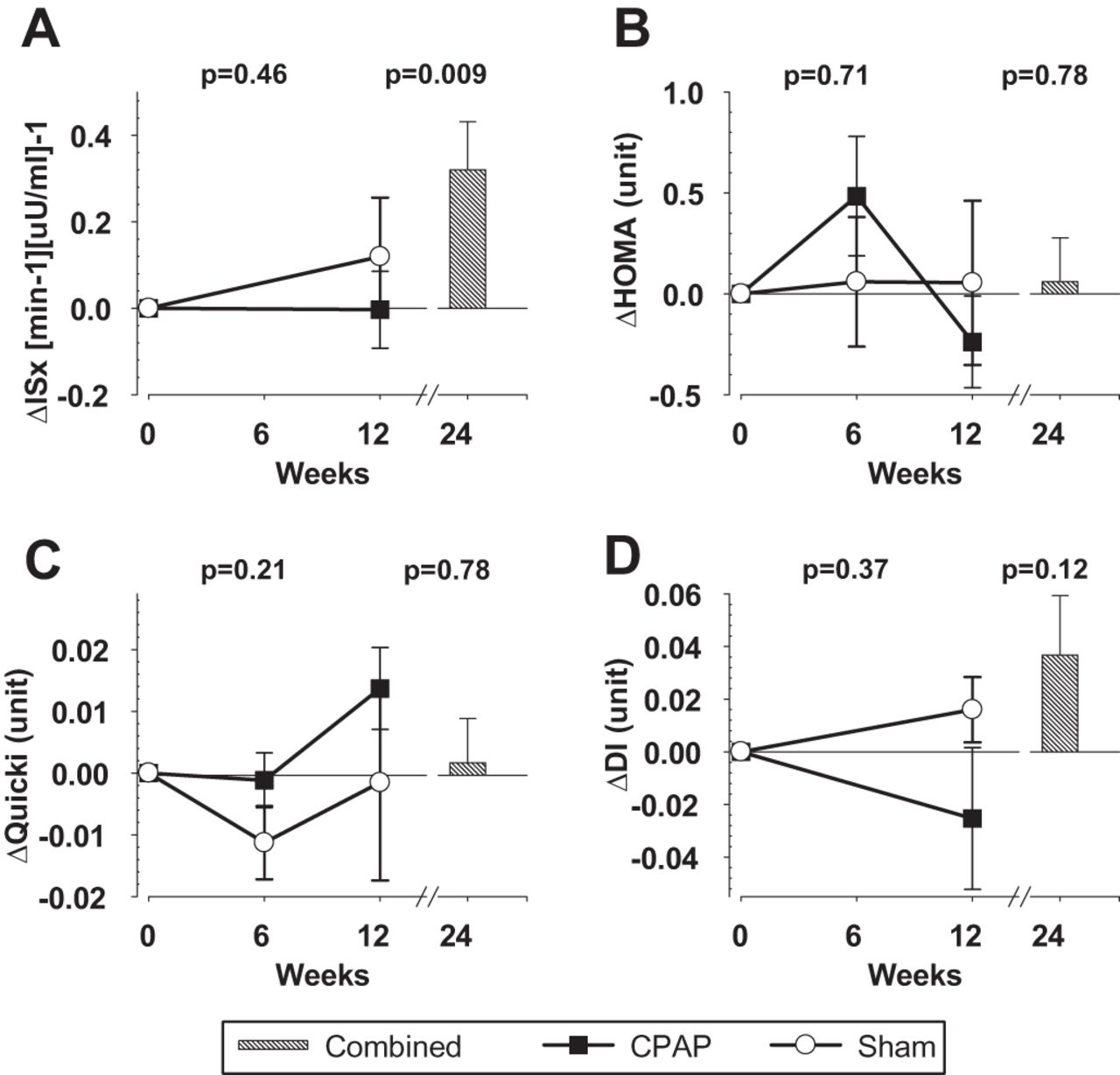
There were no significant changes in ISx, DI, HOMA, QUICKI, fasting glucose, insulin, adiponectin or leptin over the first 12 weeks within or between treatment groups (figures 3 and 4). At week 24, the entire pooled group improved in ISx, as measured by minimal model analysis (figure 3A). These improvements were due to a significant increase in those initially randomised to real CPAP (p=0.02), rather than sham (p=0.20) (table 3), and there was no between-group difference (p=0.32). There were no other significant changes in metabolic parameters (figures 3 and 4).
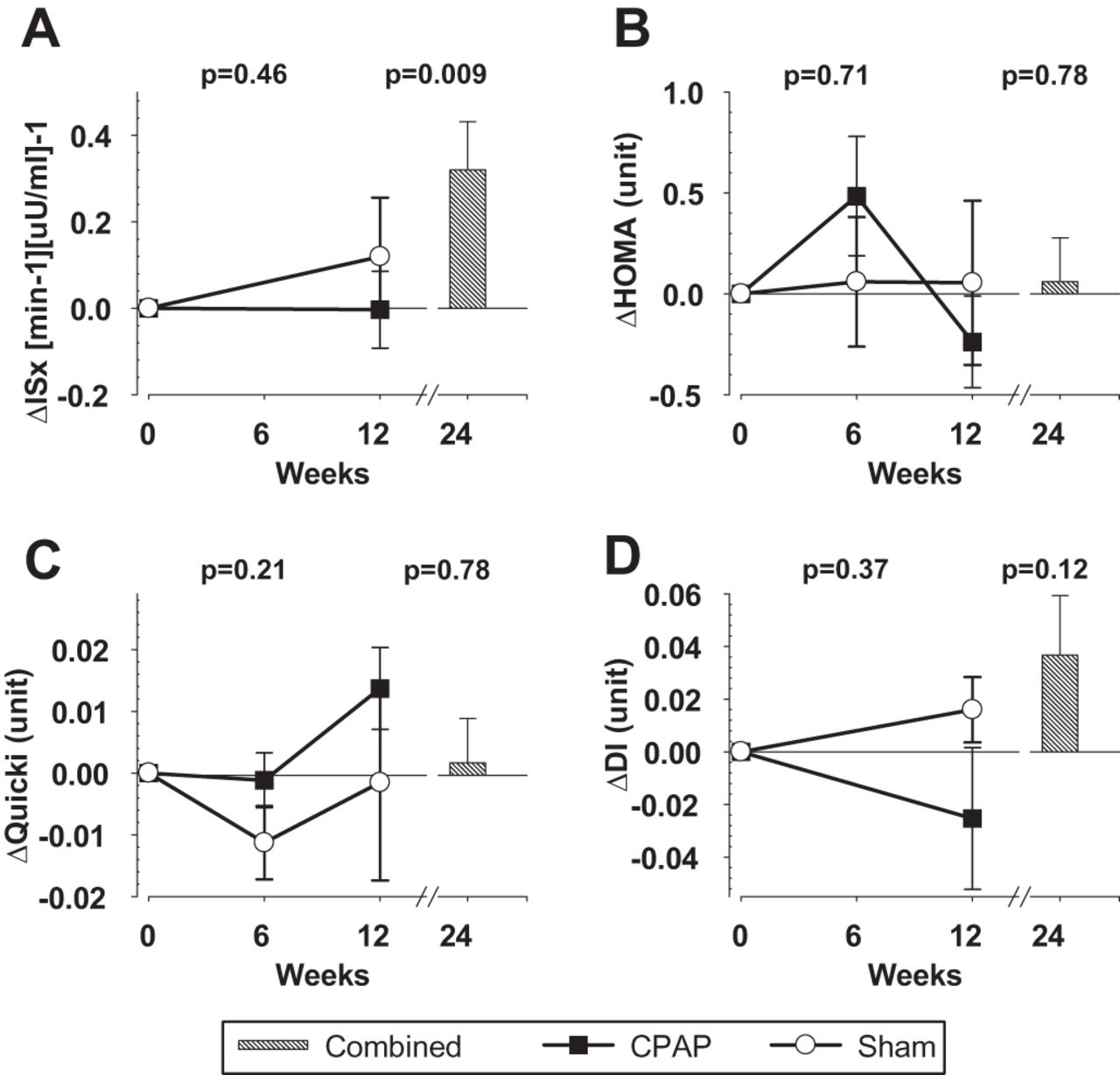
Plot of mean and SE of the mean for (A) insulin sensitivity as measured by minimal model analysis (ISx), (B) insulin resistance as measured by the homeostatic model (HOMA), (C) insulin sensitivity measured by the quantitative insulin sensitive check index (QUICKI) and (D) disposition index. The left-hand plot (line graph) shows the mean change at week 12 (and week 6 in plots B and C) from baseline for the real continuous positive airway pressure (CPAP) (filled circles) and sham CPAP (open circles) groups. The p value above this graph denotes the between-group difference as determined by linear regression (mixed model analysis for plots B and C). The right-hand plot (vertical bar graph) is the pooled mean change at week 24 from baseline in all participants regardless of initial treatment allocation. The p value above this graph denotes the significance of the change as determined by Student's t test.

Plot of mean and SE of the mean for (A) fasting insulin, (B) fasting blood glucose, (C) serum adiponectin concentrations and (D) serum leptin. The left-hand plot (line graph) shows the mean change at weeks 6 and 12 from baseline for the real continuous positive airway pressure (CPAP) (filled circles) and sham CPAP (open circles) groups. The p value above this graph denotes the between-group difference as determined by mixed model analysis. The right-hand plot (vertical bar graph) is the pooled mean change at week 24 from baseline in all participants regardless of initial treatment allocation. The p value above this graph denotes the significance of the change as determined by Student's t test.
At week 12, real CPAP treatment significantly improved OSA parameters compared with sham CPAP (figure 5). The average nightly AHI as measured by the CPAP device, over the entire 12-week period, was 3.1 events/h in the real CPAP group (not available for sham group). The change in total sleep time was not different between groups, but rapid eye movement (REM) and non-REM sleep significantly increased and decreased respectively with real CPAP compared with sham (table 2). There were no between-group differences in the changes in subjective sleepiness (table 2). At week 24, OSA parameters had improved from baseline in all participants regardless of initial treatment allocation (figure 5 and table 3).

Plot of mean and SE of the mean for (A) apnoea hypopnoea index (AHI), (B) oxygen desaturation index (ODI), (C) minimum saturation level (min sats) and (D) the per cent of total sleep time that the arterial oxygen saturation was <90% (SpO2T90). The left-hand plot (line graph) shows the mean change at week 12 from baseline for the real continuous positive airway pressure (CPAP) (filled circles) and sham CPAP (open circles) groups. The p value above this graph denotes the between-group difference as determined by linear regression. The right-hand plot (vertical bar graph) is the pooled mean change at week 24 from baseline in all participants regardless of initial treatment allocation. The p value above this graph denotes the significance of the change as determined by Student's t test.
Changes from baseline in real CPAP and sham CPAP groups and the between-group differences
Whole and within initial treatment group changes from baseline to week 24
We next assessed whether CPAP compliance, baseline age, AHI, BMI, waist circumference or sleepiness influenced treatment outcomes (namely, change in VAF, ISx and liver fat). We dichotomised age by the median, compliance by 4 h/night, AHI by 30 events/h, BMI by 30 kg/m2, waist circumference by 102 cm and ESS by 10 units and examined the interaction terms between treatment and the dichotomised variable in a series of regression analyses. CPAP compliance did not influence the treatment effect on VAF (interaction term, p=0.87), ISx (p=0.62) or liver fat (p=0.97). Age, AHI, BMI, waist circumference and ESS also did not influence the treatment effect on VAF (interaction terms all p>0.19), ISx (all p>0.18) and liver fat (all p>0.43). Analogous analyses using CPAP compliance, age, AHI, BMI, waist circumference and ESS as a continuous variable did not alter the significance of any of the between-group associations in regression analyses (all p>0.35). This indicates that these variables examined continuously did not influence the CPAP treatment effect either. Finally, there were no correlations between CPAP compliance and the change in VAF (r=−0.07, p=0.64, figure 6) or liver fat (r=0.005, p=0.98) and ISx (r=−0.02, p=0.91). Similar figures were obtained for liver fat and ISx (not shown).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Correlation between continuous positive airway pressure (CPAP) use and the change in visceral abdominal fat (VAF) at week 12. The r and p values are derived from Pearson's correlations.
At weeks 12 and 24 there was a significant correlation between change in BMI with the change in leptin concentrations in the whole group regardless of initial treatment allocation (week 12: r2=0.33, p=0.0008; week 24: r2=0.55, p=0.0001). There was no such correlation between BMI and adiponectin.
Discussion
This is, to our knowledge, the first randomised sham-controlled trial of the effect of CPAP treatment for OSA on VAF and liver fat, and the largest and longest trial of CPAP on ISx to date. We demonstrated that 12 weeks of CPAP did not improve VAF, liver fat or ISx compared with sham CPAP. Small long-term improvements in ISx, but not VAF or liver fat, were observed but only in those who received a total of 6 months of CPAP treatment, albeit in a non-randomised phase. Furthermore, both the actual and standardised mean changes from baseline in VAF at 24 weeks were small. These data suggest that reducing visceral adiposity cannot be achieved with CPAP alone and that other interventions to reduce VAF will be required. This is important because reducing abdominal adiposity, rather than overall adiposity, is now recognised as the more metabolically relevant target. At present, lifestyle modification programmes to enforce total weight loss would seem to be the most likely strategy to ensure regional changes in adiposity and such programmes have been successfully applied in those with OSA.30–32 Pharmaceutical methods could still be used in conjunction with lifestyle modification, but available options are becoming increasingly limited and the safety of any new drug would need to be firmly established in the OSA population.33
Our finding that CPAP does not alter VAF after at least 3 months of CPAP treatment is consistent with uncontrolled studies, including the longest (8 months) and largest (n=113) to date.12–14 In contrast, a recent 3-month randomised sham-controlled study,34 as well as a 3-month10 and 6-month11 uncontrolled study have shown that CPAP reduces VAF. Our study is more than twice as large and of equal or longer treatment duration as the two uncontrolled and non-randomised studies which previously reported that CPAP decreases VAF.10 ,11 Furthermore, the recently published randomised sham-controlled CPAP study showed that CPAP reduced VAF, total body weight and metabolic syndrome.34 A reduction in total body weight alone would be expected to reduce VAF and metabolic syndrome. This finding that 3 months of CPAP can reduce total body weight has never previously been reported in any randomised sham-controlled trial and requires replication in other cohorts.
There was also no effect of CPAP on liver fat, which is in contrast to a previous uncontrolled study that showed 2–3 years of CPAP treatment can significantly decrease liver fat, but only in the subgroup of CPAP adherers (n=6) in whom other lifestyle modifications undertaken in conjunction with CPAP could have plausibly reduced liver fat.15 Furthermore the changes observed in this highly selected patient group may not be comparable to a general OSA population.
We found that CPAP therapy did not alter total body fat at any time, but significantly increased lean (muscle) mass at 6 months in all participants irrespective of initial treatment allocation. Our total body findings are consistent with an uncontrolled study showing that 8 months of CPAP did not alter total body fat but did significantly increase lean muscle mass.12 Increased lean body mass can have positive metabolic benefits if persistent over time and of sufficient magnitude. Potential improvements include increased exercise capacity, basal metabolic rate and ISx. Such improvements would occur even without changes in total or regional body fat.
The ISx findings are consistent with all previous randomised sham-controlled trials investigating 6–12 weeks of CPAP therapy.16 ,17 ,34 ,35 Although one sham-controlled trial showed improvement in ISx after just 1 week,14 a recent meta-analysis of randomised controlled studies36 (which included that trial) is consistent with our findings of no CPAP effect on ISx. Since the randomised controlled portion was of 1-week duration, that study was not designed to determine whether the improvement in ISx is maintained longer term. In contrast, we did not assess acute changes in ISx, so it remains possible that CPAP could acutely and transiently improve glucose metabolism.
Small long-term improvements in ISx were observed in those who received a total of 6 months of CPAP treatment, although there were no between-group differences. Other uncontrolled trials investigating the effect of CPAP on glucose metabolism of at least 6 months' duration are available11 ,37–40 and report conflicting changes. Of these, only one formally measured ISx and this also showed an improvement.40 Our data, together with the published literature, suggest that CPAP therapy exceeding 3 months is required to improve ISx. We acknowledge that these longer-term analyses are uncontrolled and therefore a randomised controlled study of sufficient duration is needed to prove this.
Our findings indicate that CPAP treatment does not change adiponectin levels and this finding is consistent with two previous randomised sham-controlled trials.16 ,41 We also did not observe a change in leptin after CPAP, but did find a significant correlation between the change in BMI and leptin levels. This suggests that the association between OSA and leptin is mediated through obesity, as previously suggested.42 Our results are also consistent with some43 ,44 but not other studies.45 ,46 Additionally there was no between-group difference in subjective sleepiness observed, however our participants were only mildly sleepy at baseline. Other randomised sham-controlled trials have also reported similar mild sleepiness at baseline.47 ,48
A strength of this study is the inclusion of a sham-control arm. A control group, blinded to treatment allocation, is important as participants enrolled in a study may alter behaviours, such as diet and exercise, as they are aware they are being monitored. These lifestyle changes could well alter many of the markers of metabolic function which were our primary outcomes. For these reasons, a sham control was considered essential.
The CPAP adherence observed in this study is comparable to other sham-controlled studies.16 ,17 ,47 CPAP adherence has been defined as the use of more than 4 h per night, five nights per week, which is equivalent to approximately 3 h per night. Our adherence rate was 3.6 h per night in the treatment arm. Our study was designed as a practical, intention-to-treat study that in turn could be generalisable to the greater OSA population. We did not include subjects based on their compliance nor did we include a run-in treatment arm to exclude the non-adherers which has been the case in other mechanistic studies.35 Our aim was to represent the general OSA population which we believe we have done as our rates are comparable to those of ‘real life’ CPAP studies that investigate methods to increase adherence.49 Additionally our rates (3.6 h/night) are comparable to those reported by another 3-month sham-controlled study (3.3 h/night) investigating ISx.16 Interestingly, CPAP use increased by 1.1 h in those who initially received sham treatment, but was not significantly increased in those who initially received CPAP therapy. This illustrates the importance of recruiting CPAP-naïve individuals into a parallel rather than crossover study, as we have done here. A sham control is critical since placebo effects on subjective measures such as sleepiness were detected and have also previously been reported.48 Not only is our CPAP compliance comparable with other studies, but we also showed that CPAP compliance per se (as well as age, BMI, waist circumference and sleepiness) did not influence the treatment effect. Furthermore, the change in VAF that can be expected is small and demonstrating such a change would require a study of 5000 men assuming 80% power and two-sided α of 0.05 (post hoc analysis). Such a sham-controlled randomised controlled trial would be difficult to perform.
In conclusion, this study demonstrated that CPAP alone does not reduce visceral adiposity, even in the longer term. Obese men with severe OSA will most likely require weightloss interventions in conjunction with CPAP treatment to achieve this. Although 3 months of CPAP treatment did not improve ISx, longer-term treatment may produce beneficial changes but this requires further investigation.
Acknowledgments
We would like to thank Jonathan Poh, George Dungan, Frances Clements, Kerri Melehan and the sleep physicians and technicians at the Woolcock Institute of Medical Research and Royal Prince Alfred Hospital, Sleep Disorders Unit. We would also like to thank the men who participated in the study. We thank Bill Hardy, Phillips-Respironics, for the supply of manufactured sham devices.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Download Supplementary Data (PDF) - Manuscript file of format pdf
Footnotes
-
Linked article Yes.
-
Funding Supported by the National Health and Medical Research Council of Australia (NHMRC) through a project grant (512498), a Centre for Clinical Research Excellence in Interdisciplinary Sleep Health (571421) and fellowships to CH, RK, CP, RRG and PYL (512057, 633161, 571179, 202916 and 511929, respectively). Sham machines were provided by Phillips Respironics.
-
Competing interests None.
-
Ethics approval Ethics approval was provided by Sydney South West Area Health Service Human Research and Ethics Committee (RPAH Zone).
-
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Airwaves
- Correction