Article Text

Abstract
Rationale The influence of COPD exacerbation on the endothelium is not completely understood. Circulating endothelial microparticles (EMPs) are membrane vesicles in circulating blood that are shed by activated or apoptotic endothelial cells.
Objective To compare EMP numbers in stable COPD patients with those during and after exacerbation.
Methods We examined the EMP numbers in 80 stable COPD patients, 27 patients with exacerbated COPD, and 20 healthy non-COPD volunteers. EMPs were defined as CD144+ MPs (VE-cadherin EMPs), CD31+/CD41− MPs (PECAM EMPs), CD146 MPs (MCAM EMPs) and CD62E+ EMPs (E-selectin EMPs) as analysed by FACS. Von Willebrand factor (vWF) expression was utilised to identify the origins of the EMPs.
Results VE-cadherin, PECAM and E-selectin EMP numbers were significantly higher in the stable COPD patients than in the non-COPD volunteers, and they were significantly higher in the patients with exacerbated COPD than in the stable COPD patients. The majority of these increased EMPs were vWF-negative, indicating a pulmonary capillary origin. Baseline E-selectin EMP levels were significantly higher in COPD patients who experienced frequent exacerbations than in those who did not have frequent exacerbations (p<0.001). Twenty-eight days after the onset of exacerbation, E-selectin EMP levels returned to those observed in stable COPD patients, whereas PECAM EMP levels remained high. MCAM EMP numbers were not elevated in stable or exacerbated-COPD patients.
Conclusions Endothelial damage, mainly in pulmonary capillaries, occurs during exacerbation and continues even after clinical symptoms disappear. Higher baseline E-selectin EMP levels may indicate COPD patients who are susceptible to exacerbation.
- Chronic obstructive pulmonary disease
- endothelial microparticles
- exacerbation, E-selectin
Statistics from Altmetric.com
Key messages
What is the key question?
-
The influence of COPD exacerbation on the endothelium is not completely understood. We evaluated the influence of COPD exacerbation on the endothelium by measuring circulating EMPs, which are markers of endothelial damage in patients with vascular disorders.
What is the bottom line?
-
Pulmonary capillary-derived VE-cadherin, PECAM and E-selectin EMPs were significantly increased in stable COPD patients when compared with non-COPD volunteers, and were further significantly increased in exacerbated COPD patients. The baseline E-selectin EMP levels in COPD patients who frequently underwent exacerbation were significantly higher than those in COPD patients who did not have frequent exacerbation. Although the clinical symptoms of exacerbation disappeared after treatment, PECAM EMP levels remained high.
Why read on?
-
The monitoring of EMP numbers is useful for evaluating endothelial damage in COPD patients, and for identifying patients who are susceptible to exacerbation.
Introduction
Exacerbation of COPD appears to accelerate the decline in lung function1 and increase the risk of death in COPD patients.2 Thus, frequent exacerbations play a key role in disease prognosis,3 and preventing exacerbation is a key component of COPD management strategies.4 In recent years, increased evidence has demonstrated that endothelial damage is closely connected to the pathophysiology of COPD. Abnormalities in the endothelium have been recognised in both the pulmonary and systemic vasculatures in COPD.5–8 Several animal studies have suggested that endothelial injury in the pulmonary vasculature is the underlying mechanism of alveolar destruction.9 Furthermore, endothelial damage is speculated to occur during exacerbation. Inflammatory responses, such as platelet aggregation, are upregulated during exacerbation, which is speculated to lead to further endothelial damage in COPD.10 Impairment of endothelial function in systemic arteries, such as the forearm arteries, during exacerbation has also been reported.11 However, the influence of COPD exacerbation on the endothelium is not completely understood.
Circulating endothelial microparticles (EMPs) are shed membrane vesicles (100 nm–1 μm in diameter) in circulating blood that originate from activated and apoptotic endothelial cells.12 ,13 The number of EMPs increases in patients with vascular disorders, such as acute coronary disease,14 ,15 renal failure16 and metabolic diseases,17 and it reflects endothelial damage occurring in these patients. In addition, the number of EMPs is a sensitive marker of pulmonary capillary endothelial damage induced by smoking in healthy active smokers.18 We hypothesised that the number of EMPs is elevated in stable COPD patients and becomes further elevated during exacerbation.
EMPs are defined according to the expression of endothelial membrane-specific antigens, such as VE-cadherin (CD144), PECAM-1 (CD31), MCAM (CD146) and E-selectin (CD62E). These markers do not colocalise, and their expression changes according to physiological conditions. VE-cadherin localises to adherence junctions, whereas PECAM-1 and MCAM are located outside of adherence junctions.19 E-selectin is rapidly inducible on activated endothelial cells after inflammatory stimuli, whereas, VE-cadherin, PECAM-1 and MCAM are constitutively expressed on endothelial cells.20 We decided to examine the number of EMPs in stable and exacerbated COPD patients, and to evaluate the correlations between these molecules and disease progression.
Some of the results from this study have been previously presented in abstracts.21
Methods
Additional methodological details are provided in the supplementary data.
Patient population
Eighty COPD patients in stable condition (no exacerbation within the previous 3 months prior to sample collection), 27 COPD patients with exacerbation (COPD patients who experienced exacerbation of their COPD) and 20 healthy non-COPD volunteers were enrolled in this study. All subjects provided written informed consent, and the study was approved by the Ethics Committees at Tohoku University School of Medicine and the Japanese Red Cross Ishinomaki Hospital, Japan. This study was registered in the University Hospital Medical Information Network Clinical Trials Registry Clinical Trial (Trial Number: UMIN000005168). All patients had dyspnoea, chronic cough or sputum production and smoking history. Airflow limitation was determined by spirometry and defined as a postbronchodilator FEV1/FVC <0.70, and severity was classified in accordance with the Global Initiative for Chronic Obstructive Lung Disease (GOLD) criteria.22 Patients diagnosed with respiratory disorders other than COPD, such as asthma or bronchiectasis were excluded.23 All subjects had ceased smoking for more than 2 months before the enrolment. We excluded subjects with conditions known to be associated with an increase in circulating EMPs, including chronic renal failure,16 metabolic diseases, such as diabetes mellitus24 and hyperlipidaemia17 and vasculitis.25 We also excluded COPD patients with past histories of cardiovascular disease within 1 year prior to sample collection.
Exacerbation criteria
Exacerbation was diagnose based on the presence of an increase in any two major symptoms (dyspnoea, sputum purulence and sputum quantity), or an increase in one major and one minor symptom (wheeze, sore throat, cough and nasal congestion/discharge) for at least two consecutive days according to previously accepted criteria.1 ,26 We defined an exacerbation as deterioration in respiratory symptoms requiring treatment with antibiotics and/or systemic corticosteroids. The severity of exacerbation was assessed according to the criteria modified from Anthonisen and colleagues27; severe exacerbation was defined as the occurrence of all three major symptoms, moderate exacerbation as the occurrence of two of these three major symptoms and mild exacerbation as the occurrence of one major and one minor symptom.
Blood sampling
Peripheral blood was collected from a peripheral vein into heparinised tubes. Samples were centrifuged to isolate platelet-free plasma as previously described.28
Characterisation of EMPs
EMP subpopulations were determined by flow cytometry in platelet-free plasma according to the expression of membrane-specific antigens. Four EMP phenotypes were defined in the following manner: VE-cadherin EMPs: CD144+ (FITC) MPs, PECAM EMPs: CD31+ (FITC)/CD41- (PE) MPs, MCAM EMPs: CD146+ (PE) MPs and E-selectin EMPs: CD62E+ (PE) MPs. Alveolar capillaries are negative for von Willebrand factor (vWF) (supplemental figure 1), whereas, arterioles and venules in the lungs and endothelial cells in other organs are positive for vWF.29 ,30 We defined EMPs derived from pulmonary capillary endothelial cells as vWF-negative (vWF: APC) EMPs.
Pulmonary function tests
Spirometry measurements were conducted by a well-trained technician following the ATS/ERS guidelines after inhalation of a bronchodilator before sample collection.31 Pulmonary function testing was performed in duplicate. The best FEV1 and FVC values were recorded from acceptable manoeuvres.32
Visual assessment of low-attenuation areas (LAA) by chest CT imaging
We assessed LAA using high-resolution CT according to the Goddard classification.33 LAA was scored for the right and left sides of the upper, middle and lower lung fields. Zero represented no abnormality, 1 designated up to 25%, 2 up to 50%, 3 up to 75% and 4 indicated almost total involvement. The possible scores ranged from 0 to 24. The assessment was independently performed by two chest physicians (HK and MY) in a blinded fashion.
Statistical analysis
All data are presented as the median±IQR (25th–75th IQR). Difference in the distribution of the sexes between non-COPD volunteers and stable COPD patients were analysed using the χ2 test. Differences in age, body mass index, lung functions, LAA scores, physiological parameters, PaO2, traditional risk factors or inflammatory markers between the two groups were analysed using Mann–Whitney U test. The Kruskal–Wallis test was used to compare EMP numbers among the four GOLD stages. The differences in EMP numbers between stable COPD without frequent exacerbation and before exacerbation were also analysed by Mann–Whitney U test. Statistical significance of changes in EMP numbers from each time points of sample collection (before exacerbation, 1 day, 7 days and 28 days after the onset of exacerbation) was assessed by Wilcoxon signed-rank test. Correlations between EMP numbers and age, body mass index, pack-years smoking index, lung functions, LAA scores, leucocyte counts, CRP or PaO2 were calculated using Spearman nonparametric methods. Multivariable linear regression analysis was performed, with log-transformed EMPs as the dependent outcome, to evaluate the impacts of patient characteristics on EMP numbers. Multivariable logistic regression analysis was used to identify independent factors associated with frequent exacerbation history. p Values <0.05 were considered significant. All analyses were performed using the SAS system (V.8.2, SAS Institute).
Results
Characteristics of the subjects
The characteristics of the COPD patients in stable condition and the healthy non-COPD volunteers are shown in table 1. The blood pressure, total cholesterol and fasting glucose levels of all of the subjects were at normal levels. There were significant differences in the spirometric pulmonary function between the non-COPD volunteers and the COPD patients. The body mass index in COPD patients tend to be lower than that in non-COPD volunteers, but this difference is not significant. We evaluated the severity of emphysema in nine non-COPD volunteers and 74 stable COPD patients. The LAA score was significantly higher in COPD patients than in non-COPD patients, and there was a significant correlation between the LAA scores and the FEV1.0/FVC ratio (r=−0.53; p<0.001), as well as with the FEV1 (r=−0.47; p<0.001) and predicted FEV1.0% (r=−0.50; p<0.001). Eleven COPD patients had no smoking history. We examined their backgrounds and found that all these patients were passive smokers who had never smoked but had lived with family members who were active smokers.
Characteristics of 80 COPD patients in stable condition and 20 healthy non-COPD volunteers
Comparison of EMP numbers between the healthy non-COPD volunteer group and the stable COPD group
When compared with the non-COPD volunteers, the VE-cadherin, PECAM and E-selectin EMP numbers were significantly higher in the stable COPD patients. However, their MCAM EMP numbers were not higher (p=0.163) (figure 1).
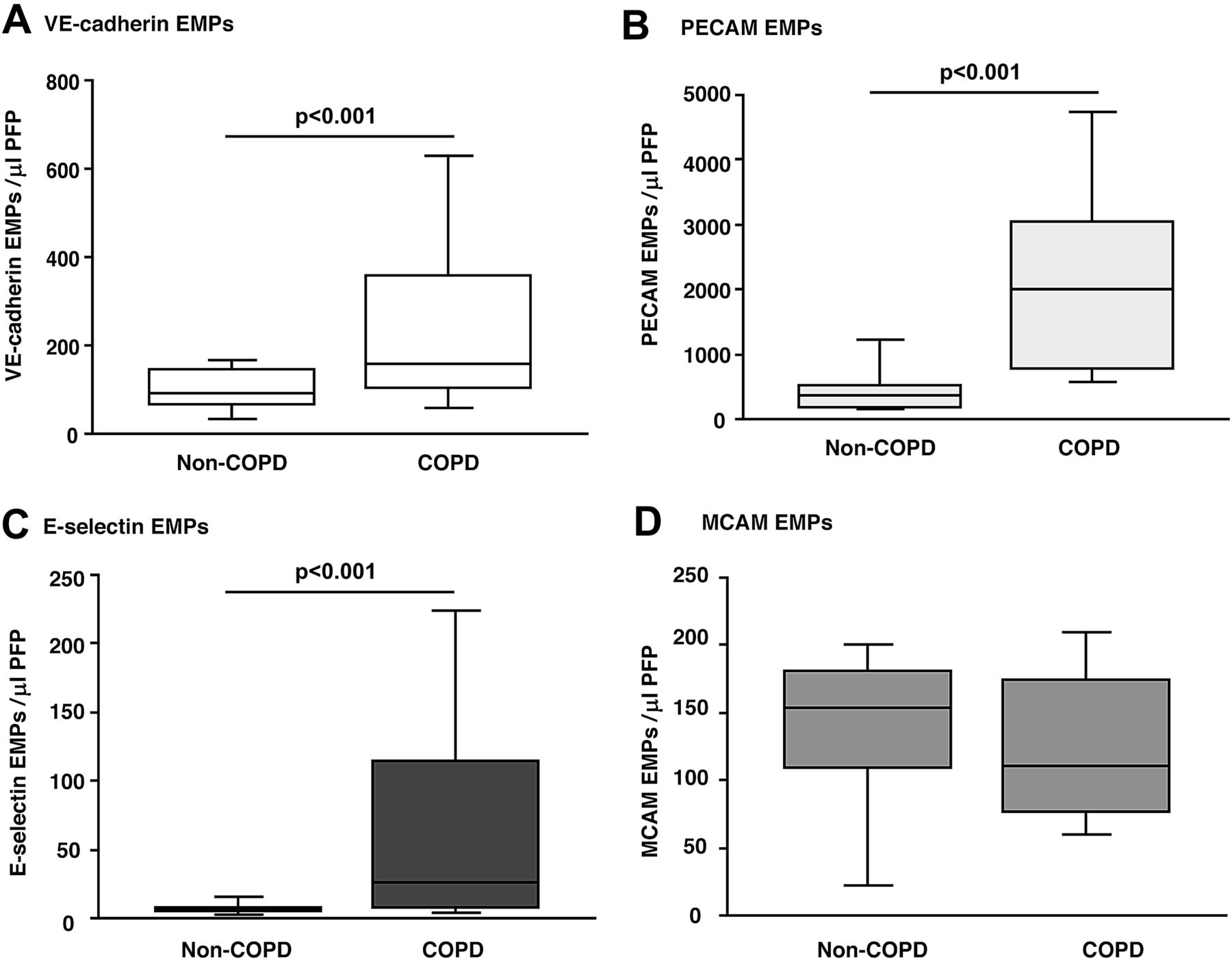
Comparison of the EMP numbers between healthy non-COPD volunteers and stable COPD patients. (A) VE-cadherin EMPs, (B) PECAM EMPs, (C) E-selectin EMPs, (D) MCAM EMPs.
Associations between EMP number and continuous variables in non-COPD volunteers and stable COPD patients
Table 2 shows the correlations between EMP numbers and different continuous valuables. VE-cadherin, PECAM and E-selectin EMPs were all significantly correlated with the three lung function parameters (figure E3), the LAA scores or body mass index. Following the results of the univariable analysis, multivariable linear regression analysis was performed to identify parameters significantly associated with numbers of VE-cadherin EMPs, PECAM EMPs and E-selectin EMPs (tables 3–5). The FEV1/FVC ratio was the only independent parameter (VE-cadherin EMPs; |r|=0.68, p<0.001, PECAM EMPs; |r|=0.58, p<0.001, E-selectin EMPs; |r|=0.60, p<0.001).
Relationships between EMP numbers and various variables in non-COPD volunteers and stable COPD patients (univariable analysis)
Multivariable linear regression analysis (80 stable COPD patients and 20 healthy non-COPD volunteers)
Comparison of EMP numbers among COPD stages as defined by the Global Initiative for Chronic Obstructive Lung Disease (GOLD)
There were no significant differences in age, body mass index, leucocyte counts, PaO2 at sample collection, CRP, SAA, D-dimer or Pack-years smoking index between the patients in different GOLD stages (supplementary online Table E2). There were significant differences in the distribution of VE-cadherin, PECAM and E-selectin EMP numbers among the GOLD stages, with the numbers of these three EMPs increasing according to disease stage progression (figure 2).

Comparison of the EMP numbers among GOLD stages. (A) VE-cadherin EMPs, (B) PECAM EMPs, (C) E-selectin EMPs.
Comparison of EMP numbers between patients with exacerbated COPD and stable COPD
We compared EMP numbers between GOLD stage II COPD patients in stable condition (n=26) and those with exacerbation (n=17) matched for age, body mass index and smoking history (table 6). Eight patients with exacerbated COPD were classified into severe exacerbation, another eight were moderate exacerbation and one was mild exacerbation. Sixteen exacerbations were bacterial associated and one exacerbation was virus associated. Antibiotics were administered to 16 patients, and systemic corticosteroid was administered to 10 patients. Seven patients were given supplemental oxygen during exacerbation. Duration of exacerbations ranged from 4 to 14 days (median, 7 days). VE-cadherin, PECAM and E-selectin EMPs were significantly higher in patients with exacerbated COPD than in patients with stable COPD (VE-cadherin; p<0.001, PECAM; p=0.004, E-selectin; p<0.001). The majority of the increased VE-cadherin, PECAM and E-selectin EMPs were vWF-negative in both the stable and the exacerbated COPD patients (figure 3).
Multivariable linear regression analysis (80 stable COPD patients and 20 healthy non-COPD volunteers)
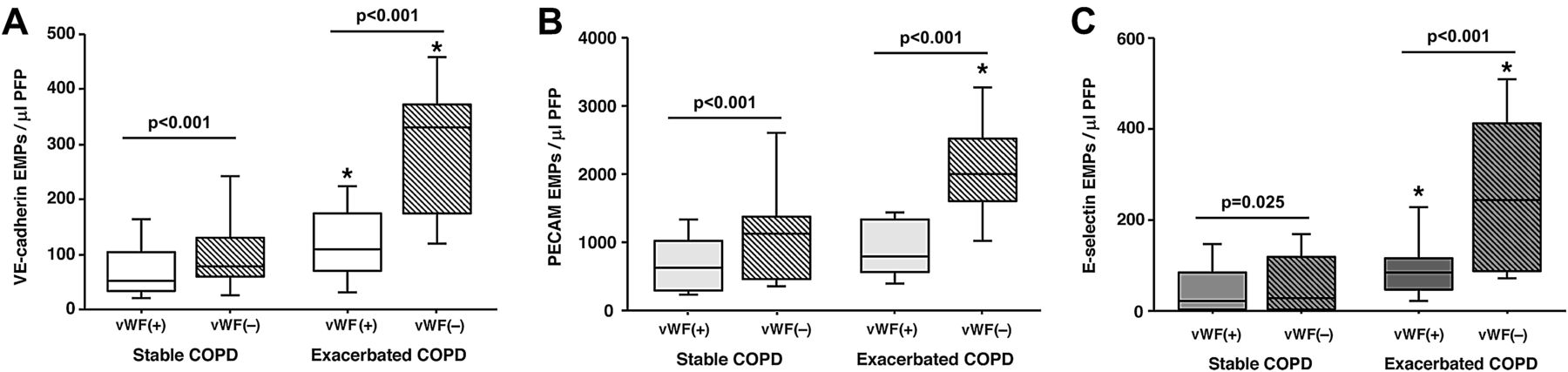
Comparison of the EMP numbers in stable GOLD stage II patients and those with exacerbation. (A) VE-cadherin EMPs, (B) PECAM EMPs, (C) E-selectin EMPs. *, p<0.05 vs. stable COPD.
Time course of EMP numbers in COPD patients during exacerbation
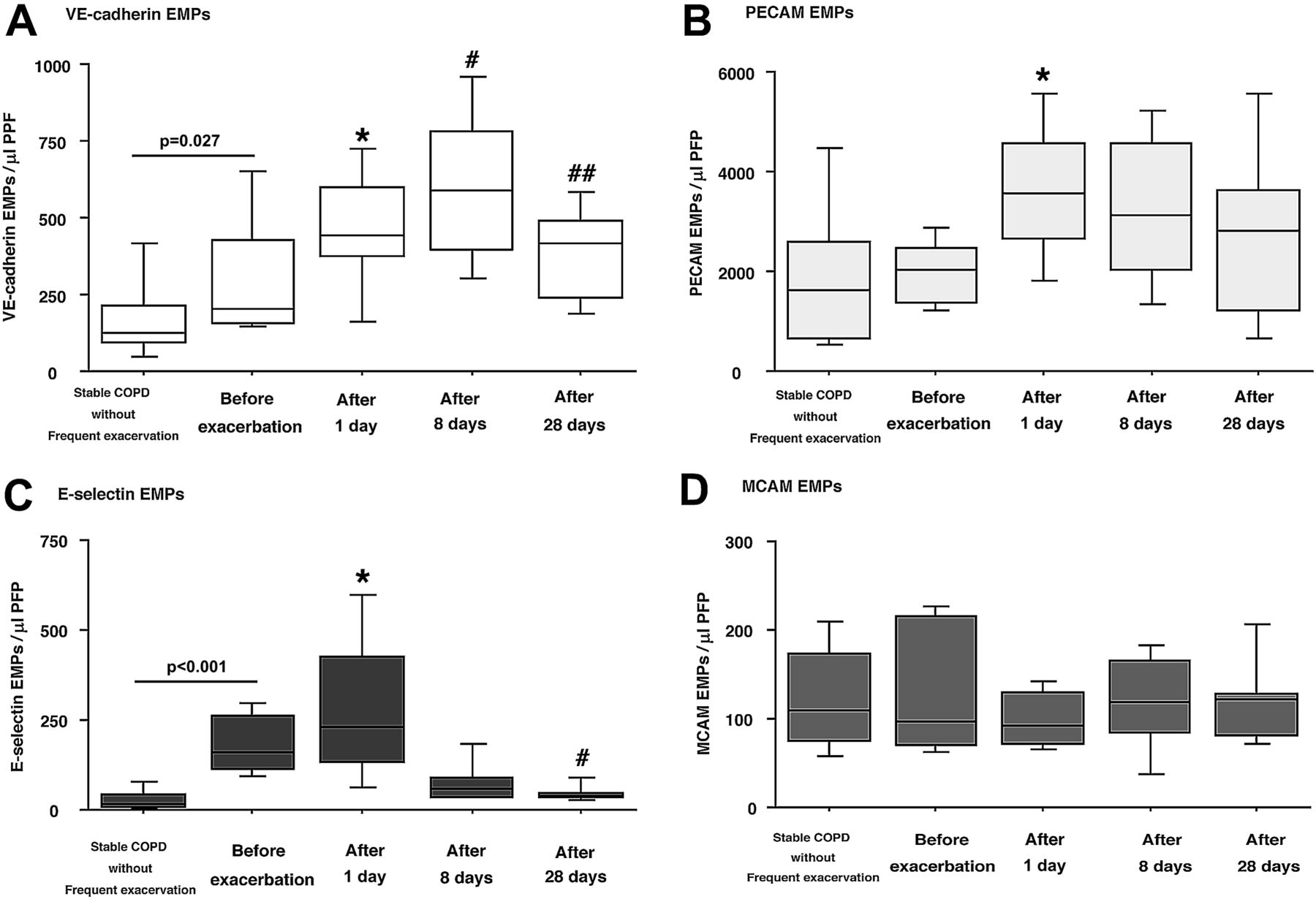
We compared the EMP numbers before and 1, 8 and 28 days following the onset of exacerbation in 18 COPD patients who underwent exacerbation (GOLD stage I, n=2; stage II, n=9; stage III, n=3 stage IV, n=4). Twelve patients with exacerbated COPD were classified into severe exacerbation, five were moderate exacerbation and one was mild exacerbation. Fifteen exacerbations were bacterial associated and the three exacerbations were virus associated. Antibiotics were administered to 15 patients, and systemic corticosteroid was administered to 14 patients. Ten patients were given supplemental oxygen during exacerbation. NPPV was used in one patient during exacerbation. Duration of exacerbations ranged from 5 to 14 days (median, 8.5 days). All 18 patients had a history of frequent exacerbation, and their E-selectin levels in stable condition were significantly higher than those in stable COPD patients without a history of frequent exacerbation (p<0.001). VE-cadherin EMPs were significantly higher one day after the onset of exacerbation when compared with the level before exacerbation (p=0.042). These EMPs continued to increase, peaked on day 8 (p=0.012 vs day 1), and were significantly lower by day 28 (p=0.027 vs day 8). PECAM EMP numbers were also significantly higher on day 1 (p=0.018) and remained elevated even at day 28 (p=0.123 vs day 1). E-selectin EMP numbers were significantly higher on day 1 (p=0.027) and returned to levels similar to those of stable COPD patients without a history of frequent exacerbation on day 28 (p=0.018 vs day 1). MCAM EMP numbers did not change during or after exacerbation (figure 4).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Time course for the EMP numbers before, during and after exacerbation. (A) VE-cadherin EMPs, (B) PECAM EMPs, (C) E-selectin EMPs, (D) MCAM EMPs. Values shown at ‘Stable COPD’ are the means of 61 stable COPD patients without histories of frequent exacerbation. *p<0.05, vs Before the onset of exacerbation. #p<0.05, versus 1 day after the onset of exacerbation. ##p<0.05, vs 8 days after the onset of exacerbation.
Parameters for patients with a history of frequent exacerbation in stable COPD
We analysed the relationships between various parameters and having a history of frequent exacerbation (table 7). We defined patients with frequent exacerbation as those who had two or more episodes of exacerbation every year. There were 19 patients with histories of frequent exacerbation in the cohort of 80 stable COPD patients. A univariable analysis showed that leucocyte counts; GOLD stage IV; and VE-cadherin, PECAM and E-selectin EMP levels in stable condition patients were significantly related to frequent exacerbation. In a multivariable logistic regression analysis, only the E-selectin EMP level was significantly associated with frequent exacerbation (OR 1.018, 95% CI 1.006 to 1.031, p=0.003). E-selectin EMP levels were significantly higher in patients with a history of frequent exacerbation than in patients without (191.0±103.5 vs 13.8±36.1, p<0.001).
Multivariable linear regression analysis (80 stable COPD patients and 20 healthy non-COPD volunteers)
Characteristics of GOLD II COPD patients during exacerbation or in stable condition
Univariable and multivariable logistic regression analyses for independent variables of COPD patients significantly associated with frequent exacerbation
Specific events in 80 stable COPD patients during 1-year follow-up after sample collection
Among 80 stable COPD patients, one patient died due to respiratory failure induced by exacerbation. In two patients, acute coronary syndrome developed and was treated with percutaneous coronary intervention. Thirty-nine exacerbation episodes happened in 21 patients including all 19 patients with history of frequent exacerbation.
Discussion
To evaluate the endothelial damage induced by exacerbation in COPD patients, we compared circulating EMP numbers and subtypes in patients in stable condition and during and after exacerbation. In this study, we found that VE-cadherin, PECAM and E-selectin EMPs were significantly more numerous in the stable COPD patients than in the healthy non-COPD volunteers, and their numbers further increased in the exacerbated phase. The main population of increased EMPs was vWF-negative, indicating particles of pulmonary capillary origin. Furthermore, baseline E-selectin EMP levels were significantly higher in COPD patients with a history of frequent exacerbation than in those without such a history. From these results, we conclude that endothelial damage, mainly in pulmonary capillary venules, occurs during exacerbation, and higher E-selectin EMP levels may predict the COPD patients who are susceptible to exacerbation.
The population of EMPs found to be increased varied according to the patient's condition. For example, VE-cadherin EMPs were still increasing 8 days after the onset of exacerbation (figure 4A), whereas, PECAM EMPs and E-selectin EMPs had already started declining at this time point (figure 4B,C). Different stimuli induce the expression of different molecules on endothelial cells, and thus, different subtypes of EMPs are released.34 VE-cadherin is localised to adherence junctions, whereas, PECAM-1 and MCAM are located mainly outside of the adherence junctions19 suggesting that the release of VE-cadherin EMPs may reflect the structural destruction of the endothelium. Therefore, particular combinations of increased EMP subtypes may become a reliable marker for predicting the type and site of inflammation.
E-selectin EMP levels that were increased by exacerbation decreased far less than the baseline level and reached the average levels of stable COPD patients. When endothelial cells are activated, E-selectin are unregulated on the cell surface20 and E-selectin EMPs are released,34 suggesting that inflammatory stimuli activate and injure endothelial cells during exacerbation. In addition, increased E-selectin EMP levels in COPD patients may indicate the presence of inflammation even in the stable condition. Furthermore, this increase indicates the silent progression of an injury or susceptibility to exacerbation.
Most of the PECAM EMPs originated from pulmonary capillaries during exacerbation (figure 3B). PECAM EMPs are reported to be released from apoptotic endothelial cells.34 In addition, 90% of these PECAM EMPs were Annexin-positive in this study (data not shown). A sustained high PECAM EMP level, despite a low E-selectin level after exacerbation, may reflect continued injury and apoptosis in the pulmonary capillaries.
A high E-selectin EMP level indicates the silent progression of an injury or susceptibility to exacerbation. In addition, high VE-cadherin and PECAM EMP levels indicated severe airflow limitation in this study (supplemental figure E3). Endothelial abnormalities have been recognised in both the pulmonary and systemic vasculature in COPD.5–7 Therefore, high EMP levels may indicate a role for endothelial damage in COPD progression. Because quicker responses can be seen in circulating EMP levels compared with an annual FEV1 decline, monitoring EMP levels is valuable for estimating COPD progression, and can be a useful index for drug discovery.
The plasma EMP levels were elevated in response to early development of emphysema in healthy smokers.18 Because COPD is a heterogeneous disease characterised by various combinations with small airway disease and emphysema, the relationships between the severity of emphysema and the numbers of EMP are also of great interest. In this study, LAA scores had significant correlations with VE-cadherin EMPs, PECAM EMPs and E-selectin EMPs. However, in multivariable regression analysis, the LAA score was not a significant independent factor, and only the FEV1/FVC ratio was a significant independent factor. Similarly, the other group also reported that the EMP number had significant correlation with FEV1/FVC ratio, not LAA in healthy active smokers.18 It is well known that the pulmonary capillary bed is significantly reduced in emphysematous regions. In addition, the main populations of the increased EMPs in COPD were pulmonary capillary derivation (figure 3). Therefore, these results indicated that the EMP numbers in COPD patients with severe emphysema might be influenced by the reduced pulmonary capillary bed.
Different from the other three EMP phenotypes, circulating MCAM EMPs did not change before or during exacerbation (figure 4D). Similarly, other groups have reported that MCAM EMPs do not reflect endothelial damage induced by INFß-1, although PECAM EMPs do.35 MCAM is also expressed on a subset of T- and B-lymphocytes, NK cells36 and pericytes.37 Therefore, circulating MCAM MPs may originate from cells other than endothelial cells.
There are limitations in this study. First, we could not evaluate the relationships between cardiovascular events and EMP numbers in COPD patients because we excluded COPD patients with cardiovascular disease. Additional effects of cardiovascular disease on the distribution of subtypes of circulating EMPs are a question for future studies. Second, we did not evaluate the other lung diseases, such as pulmonary fibrosis, or the effect of pulmonary hypertension. EMPs may increase in a range of lung diseases; therefore, increases in circulating EMPs in this study may not be specific in COPD. Further studies will be necessary to clarify this issue.
In conclusion, endothelial damage, mainly in the pulmonary capillary vasculature, occurs during exacerbation, and continues even after clinical symptoms disappear. Higher baseline levels of E-selectin EMPs suggest the presence of pulmonary inflammation and may predict COPD patients who are susceptible to exacerbation. The diagnosis of COPD exacerbation and its degree are mainly based on clinical symptoms; however, clinical parameters are not specific and are difficult to quantify. Monitoring the number and the combination of circulating EMPs is useful for evaluating the patient's condition and can be a useful indicator for the effectiveness of medications.
Acknowledgments
We are grateful to Dr Hideki Ota (Department of Diagnostic Radiology, Tohoku University Graduate School of Medicine) and Professor Takuhiro Yamaguchi (Biostatistics, Tohoku University Graduate School of Medicine) for their advice on this work.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online Supplement 1
- Data supplement 2 - Online figure 1
- Data supplement 3 - Online figure 2
- Data supplement 4 - Online figure 3
- Data supplement 5 - Online figure 4
Footnotes
-
Funding This work was supported by a grant from the Japan Society for the Promotion of Science (No. 22390163) to HK.
-
Competing interests None.
-
Patient consent We used a patient consent form approved by the Ethics Committees at Tohoku University School of Medicine and the Japanese Red Cross Ishinomaki Hospital, Japan. All consents were signed by the patients.
-
Ethics approval The Ethics Committees at Tohoku University School of Medicine and the Japanese Red Cross Ishinomaki Hospital, Japan.
-
Provenance and peer review Not commissioned; externally peer reviewed.