Article Text

Abstract
Background Despite exacerbations of chronic obstructive pulmonary disease (COPD) being both common and often fatal, accurate prognostication of patients hospitalised with an exacerbation is difficult. For exacerbations complicated by pneumonia, the CURB-65 prognostic tool is frequently used but its use in this population is suboptimal.
Methods Consecutive patients hospitalised with an exacerbation of COPD were recruited. Admission clinical data and inhospital death rates were recorded. Independent predictors of outcome were identified by logistic regression analysis and incorporated into a clinical prediction tool.
Results 920 patients were recruited: mean (SD) age was 73.1 (10.0) years; 53.9% were female subjects; mean (SD) forced expiratory volume in one second was 43.6 (17.2) % predicted; and 96 patients (10.4%) died in hospital. The five strongest predictors of mortality (extended MRC Dyspnoea Score, eosinopenia, consolidation, acidaemia, and atrial fibrillation) were combined to form the Dyspnoea, Eosinopenia, Consolidation, Acidaemia and atrial Fibrillation (DECAF) Score. The Score, which underwent internal bootstrap validation, showed excellent discrimination for mortality (area under the receiver operator characteristic curve =0.86, 95% CI 0.82 to 0.89) and performed more strongly than other clinical prediction tools. In the subgroup of patients with coexistent pneumonia (n=299), DECAF was a significantly stronger predictor of mortality than CURB-65.
Conclusions The DECAF Score is a simple yet effective predictor of mortality in patients hospitalised with an exacerbation of COPD and has the potential to help clinicians more accurately predict prognosis, and triage place and level of care to improve outcome in this common condition.
- Pulmonary disease
- chronic obstructive
- hospitalisation
- hospital mortality
- prognosis
- COPD epidemiology
- COPD exacerbations
- emphysema
- long-term oxygen therapy
- lung physiology
- non-invasive ventilation
- respiratory muscles
- sleep apnoea
- systemic disease and lungs
- allergic alveolitis
- bronchiectasis
- cystic fibrosis
Statistics from Altmetric.com
- Pulmonary disease
- chronic obstructive
- hospitalisation
- hospital mortality
- prognosis
- COPD epidemiology
- COPD exacerbations
- emphysema
- long-term oxygen therapy
- lung physiology
- non-invasive ventilation
- respiratory muscles
- sleep apnoea
- systemic disease and lungs
- allergic alveolitis
- bronchiectasis
- cystic fibrosis
Key messages
What is the key question?
-
Can inhospital mortality in patients hospitalised with acute exacerbations of chronic obstructive pulmonary disease be predicted using a simple, robust prognostic tool?
What is the bottom line?
-
A simple predictive tool (the Dyspnoea, Eosinopenia, Consolidation, Acidaemia and atrial Fibrillation Score), using indices routinely available at the time of hospital admission, can accurately predict inhospital mortality in patients hospitalised with acute exacerbations of chronic obstructive pulmonary disease.
Why read on?
-
Application of the Dyspnoea, Eosinopenia, Consolidation, Acidaemia and atrial Fibrillation Score may assist clinical decision making with regard to: early supported hospital discharge; escalation of care; or early discussion of palliative care.
Introduction
In acute exacerbations of chronic obstructive pulmonary disease (AECOPD) requiring hospitalisation, inhospital mortality was 7.7% in the 2008 UK National COPD Audit.1 A robust clinical prediction tool, developed from a large prospective cohort of unselected admissions, could assist decisions regarding: location of care; early escalation of care; appropriateness for end-of-life care; and suitability for early supported hospital discharge and therefore could help to reduce morbidity and mortality and direct the most efficient use of resources.
In stable COPD, prognostic indices have been thoroughly investigated and tools predicting mortality risk, such as the BODE Score,2 are well established. However, prognostic research in exacerbations requiring hospitalisation has been limited, and there appears to be little common ground between predictors of mortality in stable disease and during AECOPD.3 Furthermore, none of the prognostic tools developed in stable disease have been tested on hospitalised patients, and most require clinical measurements not routinely available at hospital admission. Of the prognostic tools proposed for use in AECOPD requiring hospital admission, most were derived in highly selected,4–7 rather than unselected,8 ,9 patients.
AECOPD are often complicated by radiographic consolidation; for example, in two large UK national audits, this was reported in 16% of all admissions1 and in more than 34% of patients receiving ventilatory assistance.10 We are aware that practice varies over whether such individuals are included under the diagnosis of AECOPD, but most studies of prognosis in AECOPD requiring hospitalisation have not excluded patients with complicating consolidation.4 ,5 ,8 ,9 ,11 Furthermore, CT scanning in AECOPD often shows consolidation not visible by plain radiography12 ,13 and the severity of airway obstruction and spectrum of pathogens in pneumonic and non-pneumonic exacerbations are similar.14 Pneumonic AECOPD are not simply treated as pneumonia, but require specific management of the AECOPD, including controlled oxygen therapy, corticosteroids, nebulised bronchodilators and, if respiratory acidaemia is present, non-invasive ventilation.15 We have, therefore, followed the practice of not excluding such patients.
Currently, in patients hospitalised with AECOPD complicated by consolidation, the CURB-65 (Confusion, Urea, Respiratory Rate, Blood pressure, Age > 65) community acquired pneumonia prognostic score16 is often used to risk assess and guide antibiotic therapy.17 However, we have recently shown the use of CURB-65 in patients with AECOPD and consolidation to be suboptimal,18 and a clinical prediction tool that can accurately risk stratify all patients with AECOPD is needed.
Methods
Consecutive patients admitted to one of two neighbouring acute hospitals, representing diverse catchment areas, were recruited between December 2008 and June 2010. Approval was granted by the local National Health Service Research Ethics Committee who advised that individual patient consent was not required.
Inclusion criteria were: primary diagnosis of AECOPD supported by spirometric evidence of airflow obstruction (forced expiratory volume in one second (FEV1)/forced vital capacity (FVC) <0.70) when clinically stable; age ≥35 years; smoking history of ≥10 cigarette pack years; and admission from the primary residence. Criteria for exclusion were: previous inclusion in the study; domiciliary ventilation; comorbidity expected to limit survival to <12 months (principally metastatic malignancy); or a primary reason for admission other than AECOPD. Patients were managed at the discretion of their treating physicians.
Data collection
Socio-demographic and clinical data were collected on admission (online supplementary table E1). Stable-state dyspnoea was assessed using the extended Medical Research Council (MRC) dyspnoea (eMRCD)18 Score (online supplementary table E2); this subdivides patients too breathless to leave the house unaided (traditional MRCD 5) into those able independently to manage washing and/or dressing (eMRCD 5a) and those requiring assistance with both (eMRCD 5b). We have shown in the same population reported here that the inhospital death rate for eMRCD 5b (33.1%) is substantially higher than eMRCD 5a (17.3%) and that the eMRCD Score is more strongly associated with inhospital mortality than the traditional score.18 Details of comorbidity and maintenance medications were obtained from the clinical notes. The first haematological, biochemical and arterial blood gas results (and inspired concentration of oxygen, if documented) performed by the time of, or requested at, initial senior physician review (performed at least twice daily) were recorded. The presence of new consolidation on a chest radiograph at the time of a senior physician review was recorded. The presence of atrial fibrillation was confirmed by ECG at the time of hospital admission. Patients who died in hospital were identified from hospital records.
Statistical methods
For variables with <20% missing, data were assumed to be missing at random and missing values were imputed using the expectation-maximisation algorithm (EM analysis).19 Univariate analyses were performed with and without imputed data and final conclusions were unchanged. Proportions, means with SD or medians with inter-quartile ranges were used to characterise the patient sample. Bivariate comparisons (table 1) were performed using Student t test (parametric data), Mann–Whitney U test (non-parametric data) and χ2 test (categorical data). Multicollinearity between potential predictor variables was assessed and managed according to recommendations by Field.20
Population description and comparison between survivors and those who died inhospital
To develop a predictive tool, variables univariately associated (p <0.10) with mortality were dichotomised or categorised and retained for multivariate testing. Cut-off points were identified using the following hierarchy: visual inspection of the receiver operator characteristic (ROC) curve; a clinically relevant cut-off; or a median split. Variables with <10% of the population in one group were excluded. Eligible variables were regressed against inhospital mortality using backward stepwise methodology. Goodness-of-fit was assessed by Hosmer–Lemeshow statistic,21 and analysis of studentised residuals and leverage values identified and evaluated outliers.20
For pragmatic reasons, the five independent predictors with the largest regression coefficients were included in the final clinical prediction tool. Scores for each predictor were assigned relative to the regression coefficient.22 Performance of the tool was assessed by measuring the area under the ROC curve (AUROC). Internal validation of the tool was assessed by calculating the AUROC of 10 000 bootstrapped samples.23 Two dummy prognostic models were developed using: all significant independent categorical predictors of mortality and a ‘full’ model containing all significant independent predictors in their original form (ie, with variables on a continuous scale where appropriate). Last, the AUROC between the two dummy prognostic models and the developed clinical prediction tool were compared.24 Statistical analyses were performed by the authors, using SPSS V.15 for Windows and SigmaPlot 11 (Systat Software Inc, San Jose, CA, USA). Exact methods were used for categorical data and a two-sided p value <0.05 was taken as statistically significant.
Results
In all, 920 patients were recruited and entered in the study. All eligible patients were included and none were lost to follow-up. Imputation of missing data by EM analysis was performed for: serum glucose (19.3% missing); frequency of AECOPD in the previous year (15.2%); spirometry within 2 years of admission (14.3%; of whom all had spirometry confirming airflow obstruction, performed at an earlier date); serum albumin (7.3%); admission arterial blood gas (6.3%); body mass index (BMI) (4.3%); potassium (1.4%); and respiratory rate, temperature, sodium, haemoglobin, white cell count, eosinophil count, urea and C reactive protein (all <1% missing).
The mean age of the patients was 73.1 (SD 10.0) and 53.9% were female subjects (table 1). Most patients had severe airflow obstruction (mean FEV1 % predicted 43.6, SD 17.2); mean BMI was normal (24.6 kg/m2, SD 6.3) although 16.7% were underweight (BMI <18.5 kg/m2). Approximately a third of patients had radiographic evidence of consolidation. Comparison between the patients admitted to the two study hospitals (online supplementary table E3) showed a minor difference between average FEV1 (44.8 vs 42.1% predicted) but otherwise the populations were similar.
Overall, 257 patients (27.9%) had acidaemic respiratory failure (pH <7.35 and paCO2 >6 kPa) during their hospital stay (present at admission in 178 patients). Of these, 195 patients (21.6%) received non-invasive ventilation; four required immediate intubation and ventilation; and 58 either improved with medical therapy or were not ventilated for clinical reasons. Of the 51 patients with severe dyspnoea (eMRCD 5b) who met the criteria for assisted ventilation (pH <7.35 and paCO2 >6 kPa), 44 received it and seven were not ventilated, but instead received end-of-life care.
In total, 96 (10.4%) died during their hospital stay: 86 from respiratory disease and 10 from non-respiratory disease. Significant differences between survivors and non-survivors are shown in table 1.
Using the methods described above, the following categorical variables were entered in a backward stepwise logistic regression analysis: age ≥80 years; living independently; ≥3 hospital admissions in the previous year; eMRCD (groups 1–4 combined and used as reference category); FEV1 <50% predicted; diastolic blood pressure ≤60 mm Hg; respiratory rate ≥30/min; temperature <37°C; BMI <18.5 kg/m2; recent weight loss ≥5%; pH <7.3; potassium ≥5 mmol/l; urea ≥7 mmol/l; creatine ≥100 μmol/l; albumin <36 g/l; glucose ≥8 mmol/l; haemoglobin <12 g/dl; neutrophil count ≥9 ×109/l; C reactive protein ≥50 mg/l; eosinophil count <0.05 ×109/l; long-term oxygen therapy; atrial fibrillation; cerebrovascular disease; purulent sputum; acute confusion; ineffective cough; and radiographic consolidation.
The resulting regression model (table 2) accounted for 42% of the variance in the outcome variable (Nagelkerke R2 =0.42) and was a satisfactory fit to the data (Hosmer–Lemeshow statistic =0.39). No regression assumptions were violated by our model and none of the small number of statistical outliers significantly influenced the model. For comparison, the full regression model including all variables in their original form is shown in online supplementary table E4. Except for low BMI, all independent categorical predictors (table 2) were also significant predictors in the full model (online supplementary table E4).
Independent categorical predictors of inhospital mortality
In order to develop a simple and easy to use tool, the strongest five categorical variables were selected and relative weights assigned according to the regression coefficient (B). Table 3 shows calculation of the Dyspnoea, Eosinopenia, Consolidation, Acidaemia and atrial Fibrillation (DECAF) Score.
The DECAF Score
The area under the DECAF Score ROC curve for predicting inhospital mortality was 0.86 (95% CI 0.82 to 0.89) (figure 1), and the bootstrapped AUROC was 0.86 (0.82 to 0.89), indicating good internal validity. Compared with the DECAF Score, there were small but statistically significant differences between (a) the AUROC for a dummy categorical tool (using all the variables listed in table 2) (0.89 vs 0.86, p=0.038) and (b) the AUROC for the full regression model using all variables in their original form (online supplementary table E4) (0.90 vs 0.86, p<0.001). The DECAF Score performed strongly in each participating hospital (AUROC =0.88 vs 0.84, p=0.27) and if the population was stratified according to FEV1 (AUROCFEV1 <50% =0.857 vs AUROCFEV1 ≥50% =0.850, p=0.91). Inhospital and 30-day death rates, and sensitivity and specificity for inhospital mortality, for the DECAF Score are shown in table 4.
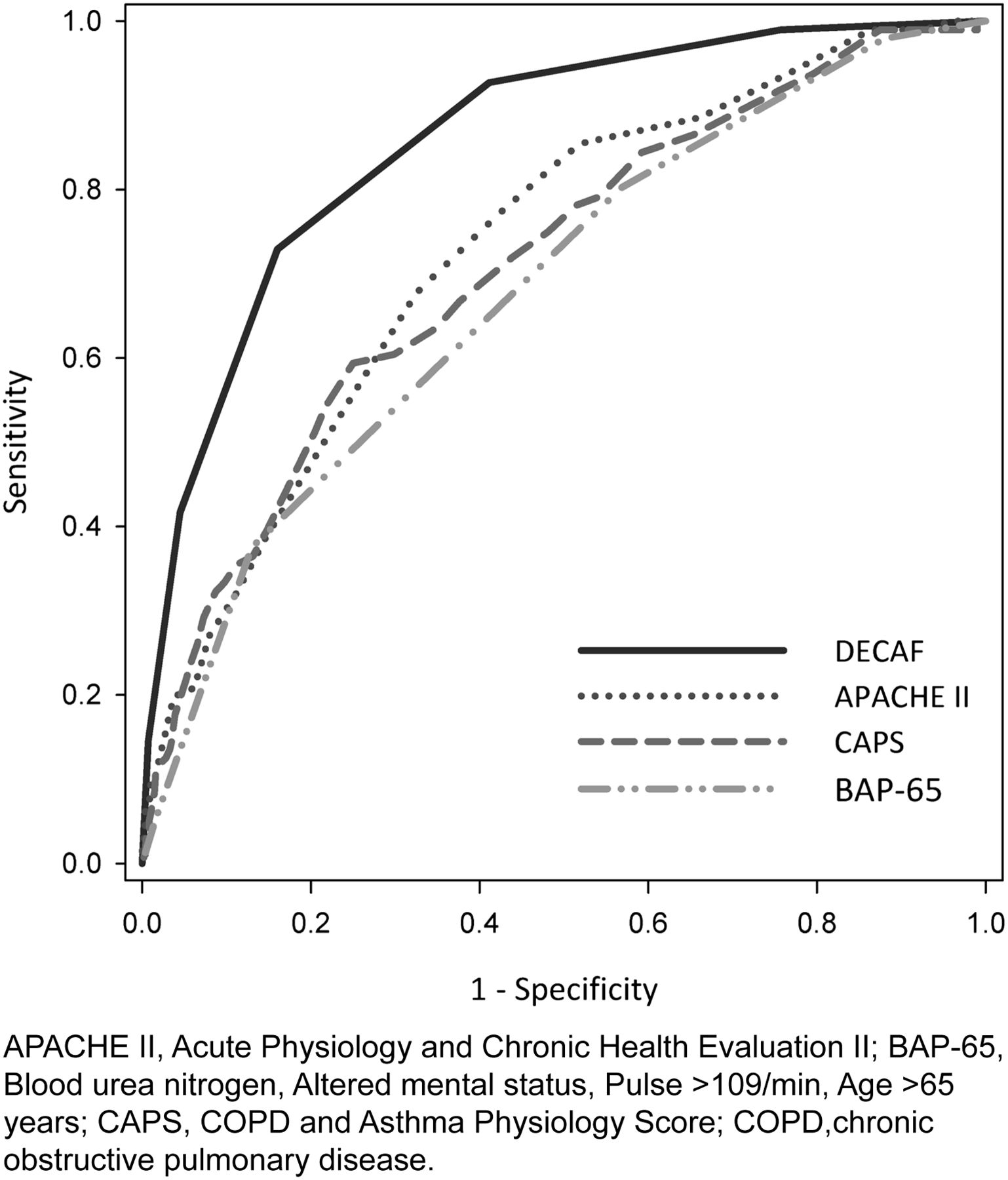
Receiver operator characteristic curve showing discrimination of Dyspnoea, Eosinopenia, Consolidation, Acidaemia and atrial Fibrillation (DECAF) Score for inhospital mortality in the total population.
DECAF Score and inhospital mortality
In our cohort, the DECAF Score performed significantly better for the prediction of inhospital mortality than: the Acute Physiology and Chronic Health Evaluation (APACHE) II prognostic index25 (AUROC =0.73, DECAF vs APACHE II p<0.001); the COPD and Asthma Physiology Score5 (AUROC =0.71, p<0.001); and the BAP-65 (elevated Blood urea nitrogen, Altered mental status, Pulse >109/min, Age >65 years) Score8 (AUROC =0.68, p<0.001) which have all been proposed as useful predictive instruments in AECOPD (figure 1).4 ,5 ,26
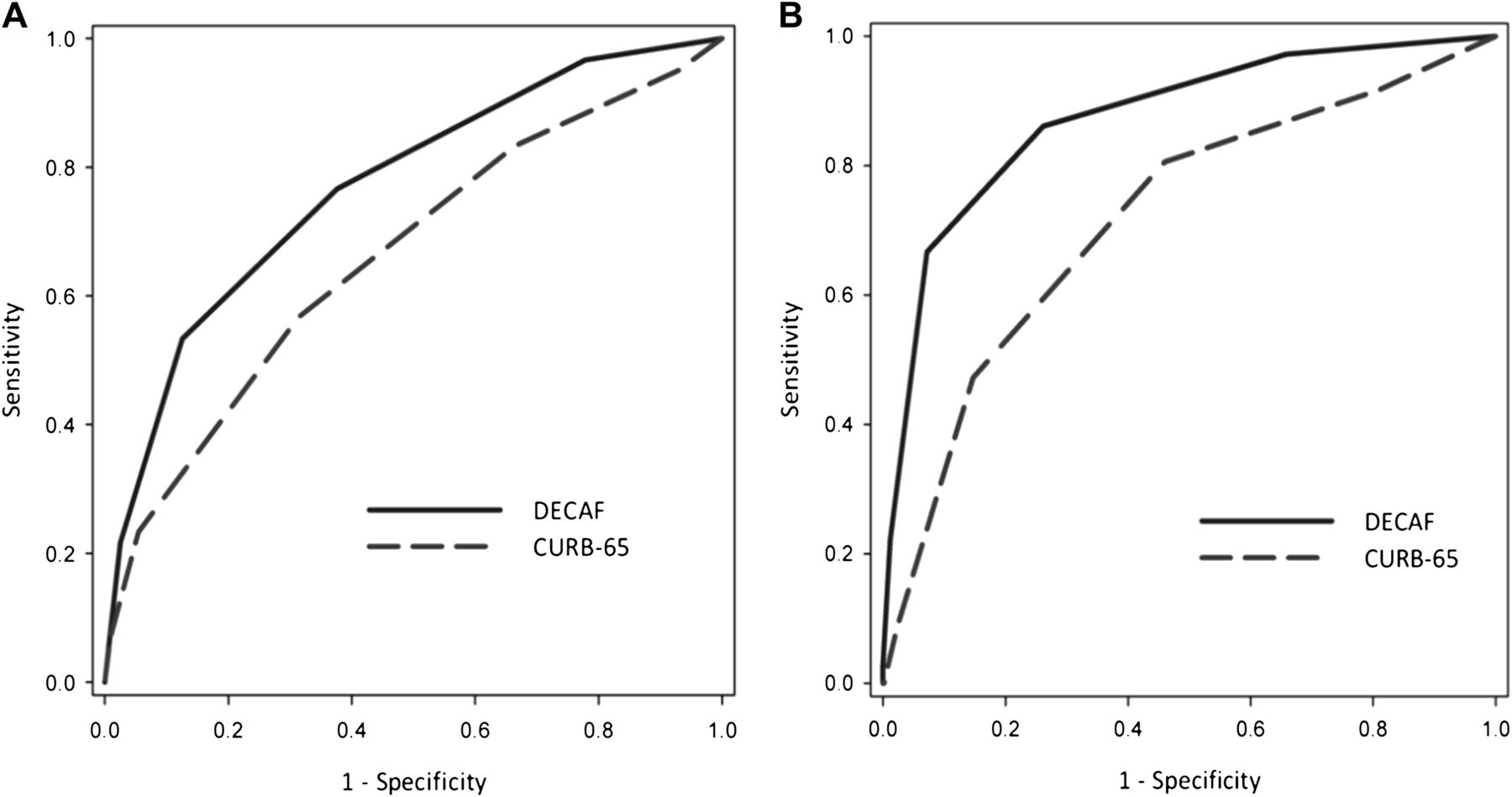
DECAF was a significantly stronger predictor of inhospital mortality than CURB-65 for both patients with (AUROC =0.77 vs 0.66, p=0.003, n=299) (figure 2, panel A) and without (AUROC =0.87 vs 0.72, p=0.002, n=621) (figure 2, panel B) consolidation. As CURB-65 was introduced to predict 30-day mortality, we also assessed the use of DECAF for predicting 30-day mortality. The AUROC of DECAF for the prediction of 30-day mortality was 0.82 (0.78 to 0.86) and, in the subgroup with consolidation, it was a stronger predictor than CURB-65 (AUROC =0.75 vs 0.64, p=0.003).
{kind=link}
{kind=link}
Receiver operator characteristic curve showing discrimination of Dyspnoea, Eosinopenia, Consolidation, Acidaemia and atrial Fibrillation (DECAF) Score and CURB-65 for inhospital mortality for patients with (n=299, panel A) and without (n=621, panel B) consolidation.
Discussion
In patients hospitalised with AECOPD, a simple prognostic tool, incorporating clinical and laboratory information available routinely on admission, accurately predicted inhospital mortality, and performed more strongly than other proposed prognostic scores. In the subgroup of patients with consolidation complicating AECOPD, the DECAF Score was a stronger predictor of mortality than CURB-65.
Our study conclusions are strengthened by the prospective recruitment of a large number of sequential patients; in particular, the two institutions reflect different catchment areas (urban and rural) with different structures of care and a wide range of socio-economic status represented and our inclusion criteria ensured a broad spectrum of patients with AECOPD were recruited. Furthermore, performance of the tool on internal validation was strong and, although external validation is necessary, our findings support the generalisability of the conclusions. Allowing for the difference in proportions with consolidation in our study (32.5%) and the UK national audit (16%), the death (non-pneumonic AECOPD = 5.8%, pneumonic AECOPD = 20.1%) and readmission rates of our patients were in line with UK national data. Practice regarding the inclusion of patients with pneumonic AECOPD under the diagnosis of AECOPD does, however, vary between hospitals and, therefore, we suggest that in future national audits, mortality data should be stratified by the presence or absence of complicating consolidation.
We are aware that comparisons between other prognostic tools and the DECAF Score in its derivation cohort may introduce bias in favour of the DECAF tool. However, the large number of patients included, the generalisability of our methodology and the size of the differences in prognostic performance suggest that the stronger performance of DECAF compared with the other tools assessed is likely to be valid.
We acknowledge certain limitations in the way the data were obtained, but the study was designed to reflect the ‘real life’ clinical situation. Clinical information was gathered by medical, nursing and research staff using standard protocols, and the presence or absence of consolidation was recorded by the admitting medical team. To ensure generalisability, we included all eligible patients and did not interfere with management provided by the attending physicians. We recognise that severe disability is likely to have been an important consideration in determining the management of individual patients. However, our findings do not appear to be explained by early introduction of palliative care, or limiting the level of care, in this population because, even among patients with the most severe limitation (eMRCD 5b), most of those potentially eligible for assisted ventilation received it. Although missing data were relatively few, data had to be imputed for a small number of variables. To ensure that imputation using EM analysis did not bias our results, univariate analyses were repeated using the original dataset and the conclusions were unchanged.
Compared with the DECAF Score, there were small but statistically significant improvements in discrimination when comparing dummy prognostic tools based on either all independent categorical predictors (table 2) or all independent predictors in their original form (online supplementary table E4). However, we consider that these minor improvements are outweighed by the ease with which the simpler DECAF tool can be clinically applied. Roche et al 9 derived a predictive tool from 794 patients attending an emergency department with AECOPD. Their prognostic score showed good discrimination for inhospital mortality (AUROC =0.79) but included subjectively assessed signs of clinical severity. The DECAF Score performed more strongly in our population than the tool described by Roche et al in its derivation cohort and, furthermore, the prognostic indices included in the DECAF Score are objective with little potential for variable interpretation.
Many of the indices independently associated with higher mortality in table 2 are consistent with previously published research in AECOPD: increasing age;9 ,27 dyspnoea severity;9 low BMI;11 low pH;11 ,28 long-term oxygen therapy prescription;28 cough effectiveness;29 and coexistent consolidation.14 Both cardiovascular and non-cardiovascular chronic comorbidities have been associated with higher inhospital mortality in AECOPD,30 but, to our knowledge, this is the first study to report in an unselected population of AECOPD requiring hospitalisation that both atrial fibrillation and cerebrovascular disease are independently predictive of mortality. Holland et al 31 reported that eosinopenia (<0.04 ×109/l) was associated with a higher inhospital mortality in AECOPD, but the study population was small (n=65) and the role of confounders was not evaluated. Our results show that eosinopenia is a strong independent predictor of inhospital mortality. Of note, this finding is not due to a better prognosis among patients with eosinophilia, as patients with confirmed or suspected asthma were excluded, and only a small proportion had an elevated eosinophil count (>0.4 ×109/l, n=55) at admission; if the latter are excluded from analysis, our conclusions remain unchanged (results not shown). It is also noteworthy that Holland et al 31 excluded individuals who had recently received oral corticosteroids, and in our study, there was no significant difference in eosinophil count between patients receiving either long-term inhaled (p=0.38) or oral (p=0.51) corticosteroids and those not in receipt of these therapies. Furthermore, it has previously been shown in an animal model that eosinopenia accompanies the response to acute infection and inflammation,32 independent of adrenal glucocorticosteroids,33 and may be a useful marker of sepsis in patients who are receiving intensive care.34 ,35 In AECOPD, the strong prognostic influence of eosinopenia may reflect the severity of the accompanying acute inflammatory response.
In community acquired pneumonia, the CURB-65 prognostic tool16 effectively predicts mortality within 30 days of admission. However, although complicating consolidation is common in AECOPD, and CURB-65 is often used in this situation, we have recently shown, in the population reported here, that its performance is suboptimal.18 Compared with CURB-65, the DECAF Score was a stronger predictor of both inhospital and 30-day mortality, and in pneumonic AECOPD, CURB-65 had only moderate performance.
The DECAF Score shows promise for the risk stratification of patients hospitalised with AECOPD. ROC analysis suggests that it has at least ‘good’ performance and is a stronger prognostic score than the CURB-65, APACHE or COPD and Asthma Physiology Score predictive tools. The death rates for each grade of the DECAF Score (table 4) suggest the following risk categories: DECAF 0-1 (‘low risk’; inhospital mortality =1.4%); DECAF 2 (‘moderate risk’; mortality =8.4%); and DECAF 3–6 (‘high risk’; mortality =34.6%). Our findings suggest that more than half of the patients hospitalised with AECOPD can be classified as low risk of both inhospital and 30-day mortality and might therefore potentially be suitable for early supported discharge (ESD) schemes. Use of the DECAF Score might, therefore, increase access to ESD schemes as current evidence36 suggests approximately 25% of patients hospitalised with AECOPD are deemed eligible for ESD. There is no evidence that this finding reflects a low threshold for admission in our population as, compared with the 2008 UK National COPD Audit,1 a higher proportion of our patients required ventilation and the overall mortality, after correction for the relative proportions with consolidation, was similar in the two studies. On the other hand, a high DECAF Score might be used as a guide to early escalation of care, or, where appropriate, to early discussion of end-of-life care.
In conclusion, our results suggest that a simple clinical prediction tool, incorporating indices routinely available at the time of hospital admission, can accurately stratify patients hospitalised with AECOPD into clinically relevant risk categories and could therefore assist clinicians managing this frequently fatal condition.
Acknowledgments
The authors acknowledge the following for their help with the study: Dr Nick Steen, biostatistician, Newcastle University; the respiratory and acute care physicians at the North Tyneside General Hospital and Wansbeck General Hospital; Dr Gbenga Afolabi, Respiratory Physician; Ms Elizabeth Norman and the Respiratory Specialist Nursing Team, North Tyneside General Hospital; the North Tyneside General Hospital Teaching and Research Fellow programme; Breathe North; and the National Institute of Health Research, through the Comprehensive Local Research Network.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
-
Funding The Breathe North Appeal and the Northumbria Healthcare NHS Foundation Trust Teaching and Research Fellow Programme.
-
Competing interests None.
-
Ethics approval Ethics approval was provided by the County Durham and Tees Valley NHS Research Ethics Committee II.
-
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Airwaves