Article Text

Abstract
Introduction Ischaemic heart disease (IHD) is a major cause of morbidity and mortality in COPD patients. Effective cardiovascular therapies may have significant impact in COPD populations. In particular, β-blockers have been shown to be safe and effective in COPD. We aimed to quantify the changing prevalence of emerging cardiovascular medications in this group over the last decade.
Methods We analysed the recruitment records of well-characterised patients enrolled into the London COPD Cohort from 1995 to 2010. Date of enrolment, comorbidities, medications, demographics, smoking history and spirometry results were analysed. Prescribing data reflects that of the patients' primary physicians.
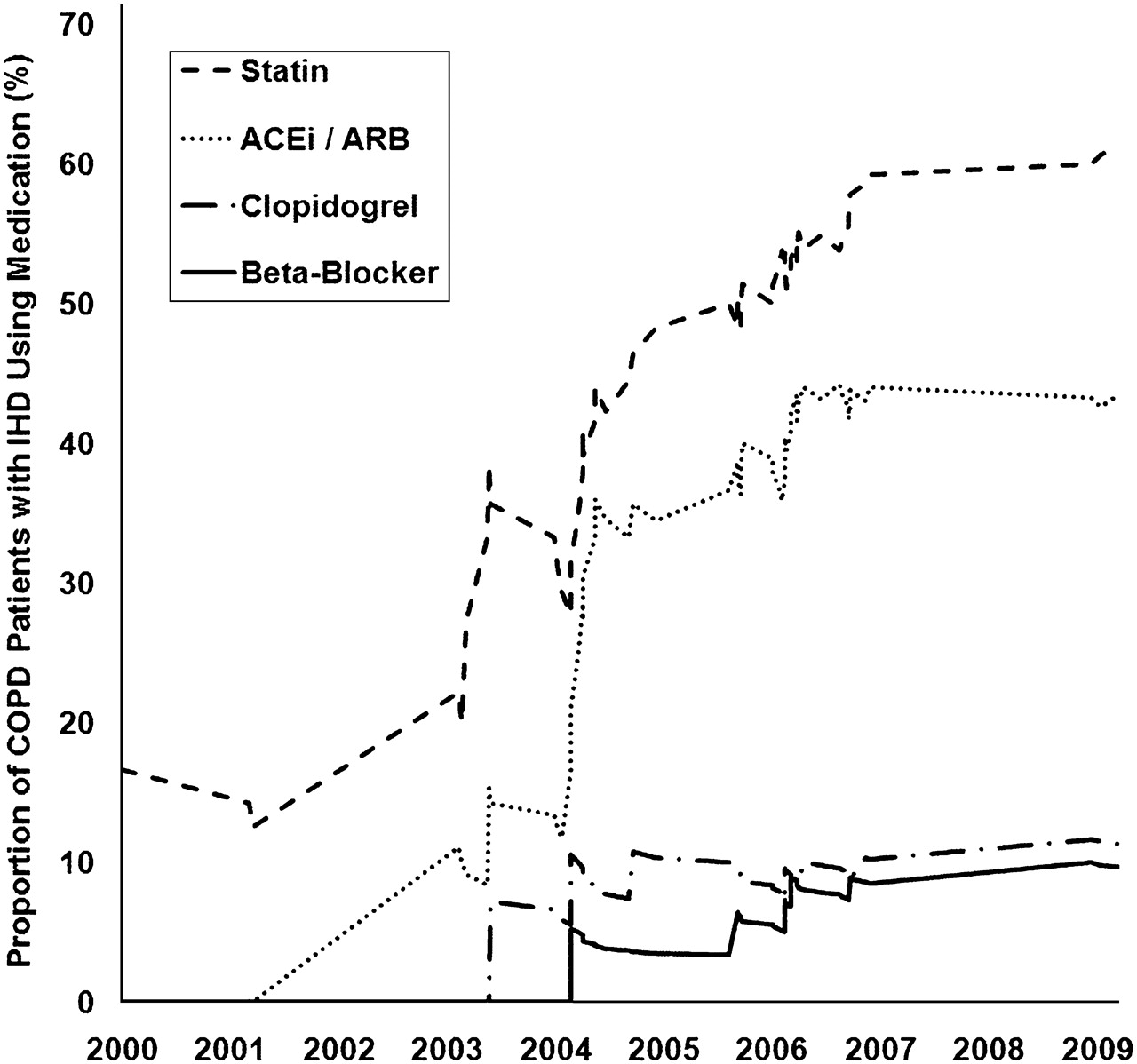
Results The mean±SD age of 386 COPD patients was 68.4±8.7 years, FEV1 was 1.22±0.55 l or 49.5±19.6% predicted. 57% were male, 24% were current smokers with a median (IQR) pack year history of 45 (25–65). 64 (17%) patients had IHD of whom half had a previous myocardial infarction, 4% had heart failure, 6% had a previous stroke, 5% had peripheral vascular disease (PVD), 9% had a tachyarrhythmia. The overall prevalence of at least one cardiovascular disease was 30%. 36% had hypertension, 8% had hypercholesterolaemia and 7% had diabetes. Common cardiovascular medications included statins (28%), aspirin (23%), calcium-channel blockers (21%), ACE-inhibitors (18%), loop diuretics (15%), thiazides (14%) and angiotensin receptor blockers (7%). β-blockers were indicated in 25% of patients (IHD ± heart failure ± tachyarrhythmia; 22% when those with the contraindication of PVD are excluded). The prevalence of β-blockers was only 5% overall and prescribed to only 8/84 (10%) in those with a clinical indication and no PVD (χ2 test, p=0.020). In the 64 patients with IHD, statins and angiotensin pathway drugs became more prevalent in the last decade of the study period (Abstract P264 figure 1) in keeping with emerging evidence of benefit. β-blockers did rise in prevalence as evidence of safety emerged, although to a much smaller extent than statins and angiotensin pathway drugs.

{kind=link}
The cumulative proportion of emerging cardiovascular medications in newly recruited COPD patients with ischaemic heart disease.
Conclusions Emerging cardiovascular medications have become more common in COPD patients reflecting greater recognition of cardiovascular risk. However, β-blockers were underused despite clear indications and evidence of safety and benefit in COPD. Measures are required to improve evidence-based prescribing to overcome historical beliefs.