Article Text

Abstract
Background Approximately 10% of patients with chronic obstructive pulmonary disease (COPD) have co-existing diabetes mellitus, conferring an adverse prognosis. Metformin is a valuable first-line treatment for diabetes. However, its rare association with lactic acidosis limits its use among patients at risk of hypoxia. This may deter some practitioners from prescribing it to patients with significant co-existing COPD. It is unknown whether the benefits of metformin outweigh its risks in this context. We therefore sought to determine the effects of metformin on survival and length of stay in a high-risk cohort of diabetic patients hospitalised for COPD exacerbations.
Methods The medical records of diabetic patients hospitalised for COPD were reviewed retrospectively. Length of hospital stay and all-cause mortality were compared according to the presence or absence of metformin therapy.
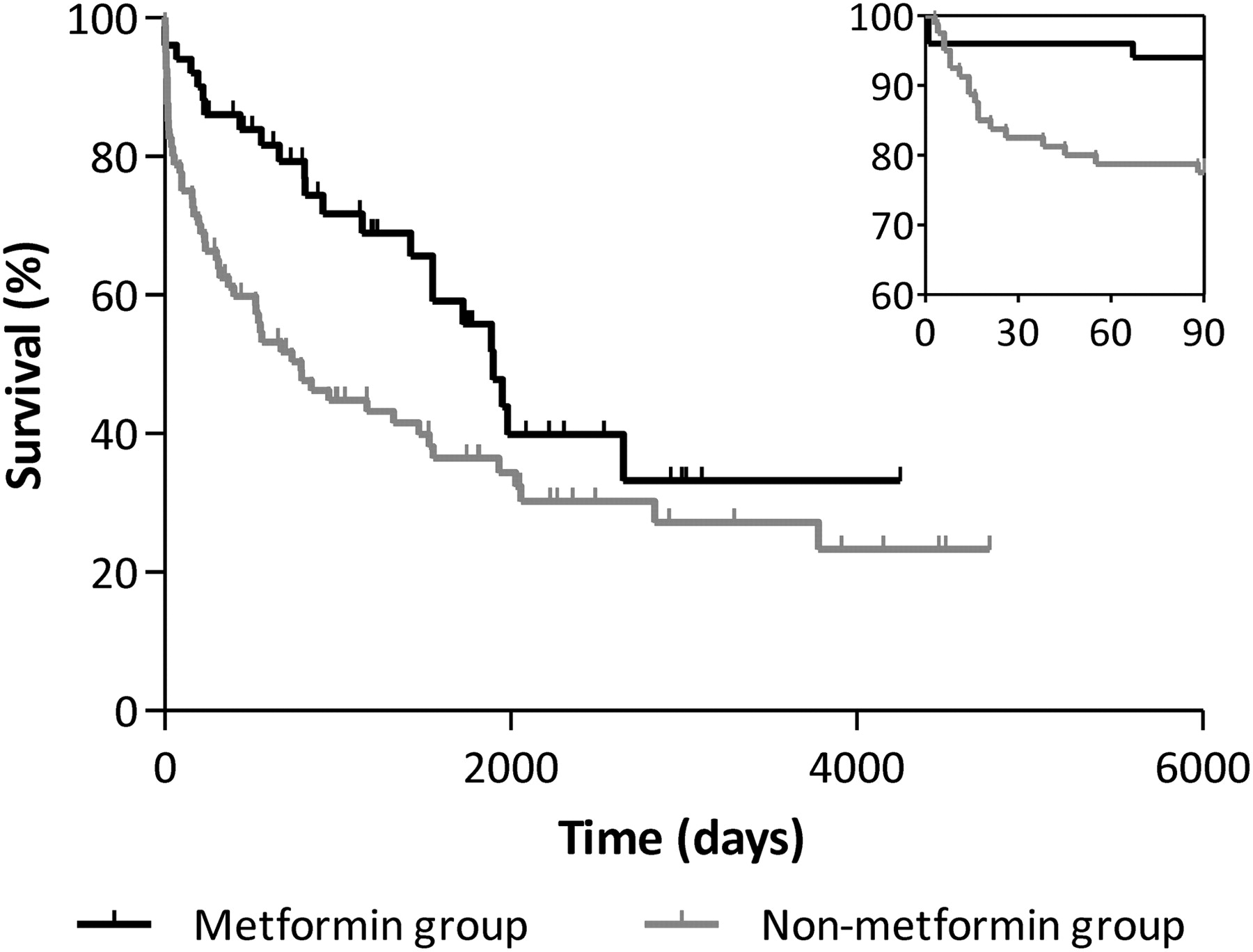
Results 130 patients were included, of whom 51 (39%) were prescribed metformin. Patients on metformin had a shorter hospital stay (median 7 vs 9 days respectively; p=0.004). Survival at 90 days was significantly better in the metformin group than in the non-metformin group (94% vs 78% respectively; p=0.015; Abstract P259 figure 1 inset). This persisted over the longer term, with overall median (95% CI) survival of 5.2 years (4.3 to 6.1) in the metformin group and 2.2 years (1.0 to 3.3) in the non-metformin group (HR 0.57; 95% CI 0.35 to 0.94; Abstract P259 figure 1). This difference remained significant in a multivariate model, adjusting for potential confounding effects of age, weight, acute illness severity (APACHE-II score) and comorbidity burden. Among patients prescribed metformin, vs those not, the median (IQR) plasma lactate concentration was 1.45 mmol/l (1.10–2.05) vs 1.10 mmol/l (0.80–1.50), respectively (p=0.012).
{kind=link}
Kaplan–Meier curves for all-cause mortality, divided according to metformin use (p=0.024, log-rank test). Inset: survival curves at 90 days (p=0.015, log-rank test).
Conclusion Diabetic patients hospitalised for COPD exacerbations who were prescribed metformin were discharged earlier and survived longer than those not prescribed metformin. Lactate concentration was higher among patients on metformin, although the difference was small. Our results suggest that the drug's benefits may outweigh its rare association with lactic acidosis. Whether this reflects beneficial effects on diabetes- or COPD-related endpoints; other associated conditions; or the effect of unmeasured confounders, is unknown. We are now investigating this within the context of a randomised controlled trial (ISRCTN66148745).