Article Text

Statistics from Altmetric.com
We welcome the recent guidelines from the British Thoracic Society on the management of Mycobacterium tuberculosis infection and disease in patients with chronic kidney disease (CKD).1 We note the paucity of evidence (particularly from the UK) in this population regarding the use of interferon gamma release assays (IGRA) in screening patients for latent tuberculosis infection (LTBI).
We present data to show the first UK-based cohort comparing the tuberculin skin test (TST) and the two commercially available IGRA—T-SPOT.TB (Oxford Immunotec, Abingdon, UK) and Quantiferon-Gold-in-Tube (Cellestis, Carnegie, Australia)—in a population of inpatients with CKD. It involves the follow-up of 61 patients from a renal inpatient ward who were screened for LTBI following exposure to a staff member with smear-negative, culture-positive pulmonary tuberculosis in 2008.
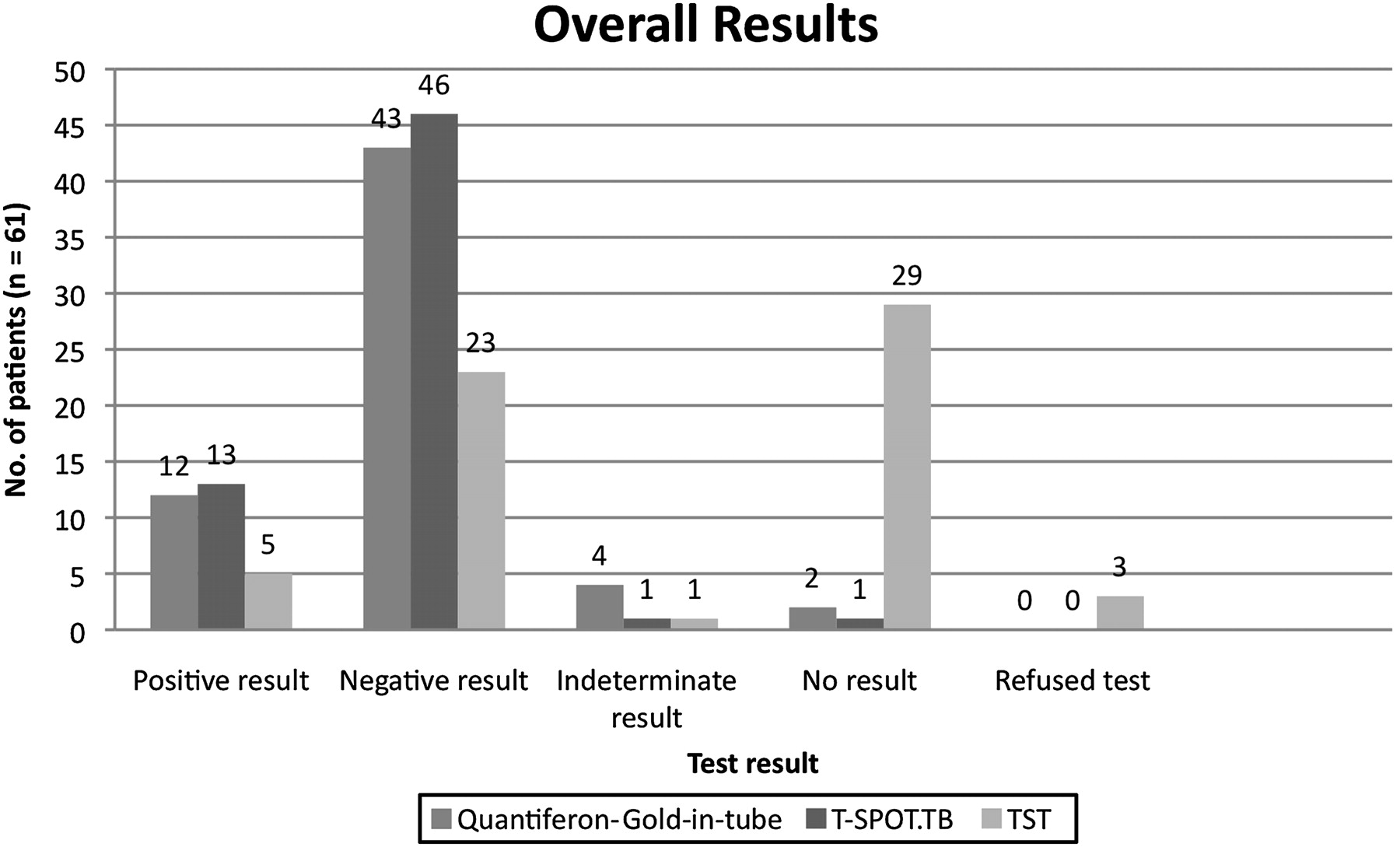
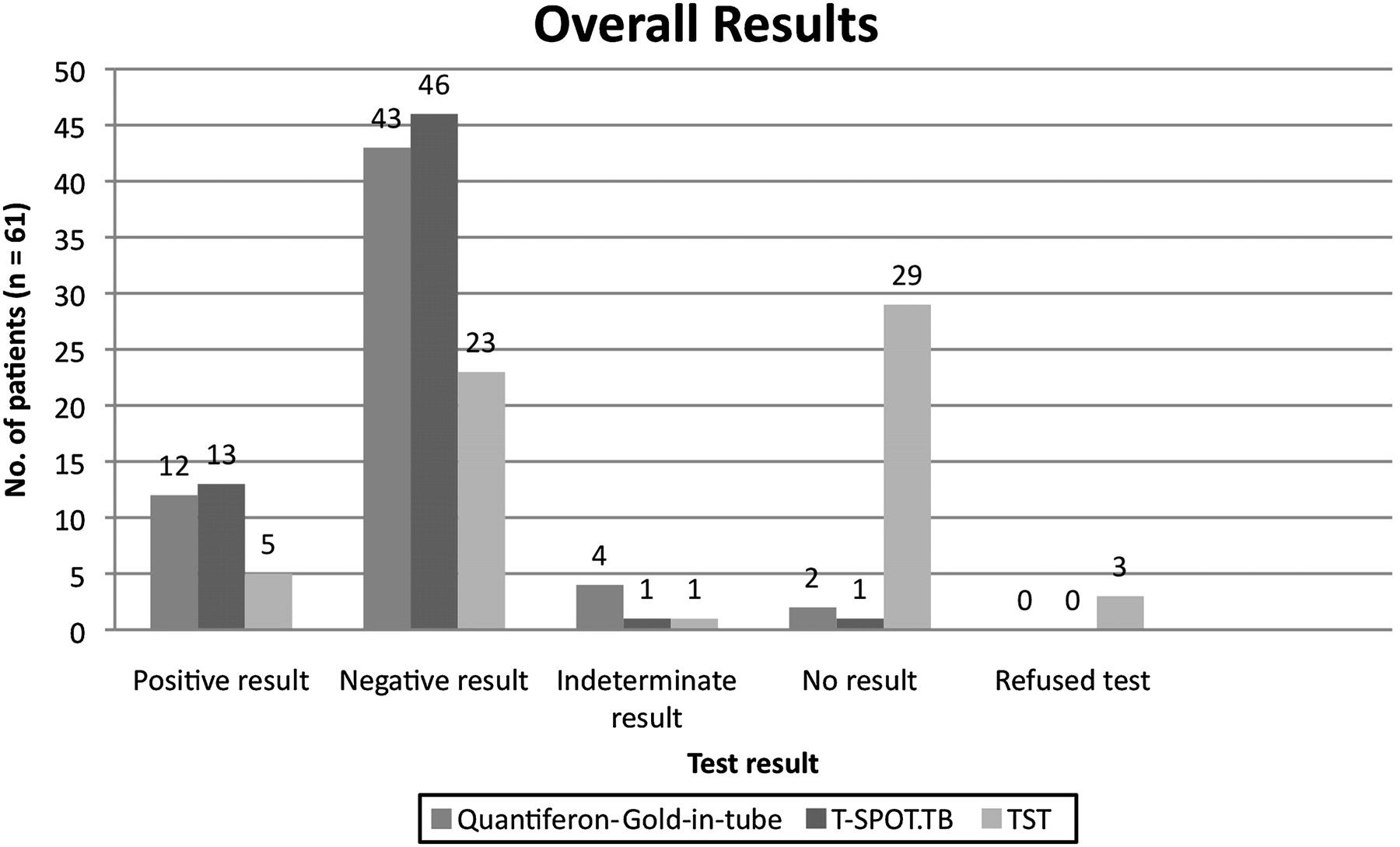
The mean age of the cohort was 62 years (range 28–88). Thirty patients were male. Eight patients were of Afro-Caribbean ethnicity, three middle eastern, one southeast Asian, 31 Caucasian and 18 from the Indian subcontinent. Forty-five patients were receiving haemodialysis; three patients had CKD stages II–IV; one patient had acute kidney injury; 12 patients were post-renal transplant; 29.5% were positive for at least one of the three tests; none of these had evidence of active disease. The results of each test are shown diagrammatically in figure 1. Of note, 48% of patients did not receive a completed TST despite standard follow-up by experienced tuberculosis nurses; 19.6% of the cohort had a positive Quantiferon-Gold-in-Tube test, 21.3% of the cohort had a positive T-SPOT.TB test and 8.1% of the cohort had a positive TST (≥15 mm if Bacillus Calmette–Guérin vaccinated; ≥5 mm if not). There were no significant associations between age, gender, diagnosis, or ethnicity and the likelihood of TST completion.
{kind=link}
Overall results comparing TST, T.SPOT.TB and Quantiferon-Gold-in-tube across the whole cohort.
Twenty-five patients had all three tests performed. Of this group, four patients had a positive TST, five patients had a positive Quantiferon-Gold-In-Tube and eight patients had a positive T-SPOT.TB (see supplementary table 1 and supplementary figure 2, available online only). χ2 tests (using Fisher's exact methods) were used to calculate associations between test modalities in this group: (1) T-SPOT.TB/Quantiferon-Gold-in-Tube: κ=0.694; p<0.002; (2) T-SPOT.TB/TST: κ=0.364; p=0.08; (3) Quantiferon-Gold-in-Tube/TST: κ=0.324; p=0.17.
When repeating the above analysis in the whole cohort (n=61), using positive test versus non-positive test as comparators, similarly significant associations were observed (see supplementary table 2, available online only).
On multivariate analysis, there were no significant associations with any of the three tests and gender, age, ethnic background or mode of renal replacement therapy. Length of exposure to the index case had no effect on the test results. (Mann–Whitney U test, p>0.1 for all three tests, comparing the median number of ‘exposed’ shifts for those with a positive test and those with a negative test).
In conclusion, these data support the growing body of evidence that IGRA appear more sensitive and accurate than the TST in detecting LTBI in this immunosuppressed group of patients.2–4 Importantly, they also provide evidence of the clinical utility of IGRA in contact tracing, and the difficulty of performing the TST, in large numbers of patients undergoing dialysis.
Supplementary materials
Web Only Data thx. 2010.149088
Files in this Data Supplement:
Footnotes
Linked articles 150102.
Competing interests None.
Provenance and peer review Not commissioned; not externally peer reviewed.
Linked Articles
- PostScript