Article Text

Abstract
Background The effect of inhaled corticosteroids (ICS) on fracture risk in patients with chronic obstructive pulmonary disease (COPD) remains uncertain. The aim of this study was to evaluate the association between ICS and fractures in COPD.
Methods MEDLINE, EMBASE, regulatory documents and company registries were searched up to August 2010. Randomised controlled trials (RCTs) of budesonide or fluticasone versus control treatment for COPD (≥24 weeks duration) and controlled observational studies reporting on fracture risk with ICS exposure vs no exposure in COPD were included. Peto OR meta-analysis was used for fracture risk from RCTs while ORs from observational studies were pooled using the fixed effect inverse variance method. Dose–response analysis was conducted using variance-weighted least squares regression in the observational studies. Heterogeneity was assessed using the I2 statistic.
Results Sixteen RCTs (14 fluticasone, 2 budesonide) with 17 513 participants, and seven observational studies (n=69 000 participants) were included in the meta-analysis. ICSs were associated with a significantly increased risk of fractures (Peto OR 1.27; 95% CI 1.01 to 1.58; p=0.04; I2=0%) in the RCTs. In the observational studies, ICS exposure was associated with a significantly increased risk of fractures (OR 1.21; 95% CI 1.12 to 1.32; p<0.001; I2=37%), with each 500 μg increase in beclomethasone dose equivalents associated with a 9% increased risk of fractures, OR 1.09 (95% CI 1.06 to 1.12; p<0.001).
Conclusion Among patients with COPD, long-term exposure to fluticasone and budesonide is consistently associated with a modest but statistically significant increased likelihood of fractures.
- Inhaled corticosteroids
- chronic obstructive pulmonary disease
- fractures
- meta-analysis
- COPD pharmacology
Statistics from Altmetric.com
Key messages
What is the key question?
Does long-term use of inhaled corticosteroids increase the risk of fractures in patients with chronic obstructive pulmonary disease (COPD)?
What is the bottom line?
Our meta-analysis shows that inhaled corticosteroid use is associated with a modest but statistically significant increase in the risk of fractures in patients with COPD.
Why read on?
The consistency and similarity of the point estimates across randomised trials and observational study designs, and the presence of a dose–response effect in the observational studies lends credibility to this clinically important association.
Background
The inhaled corticosteroids (ICS) fluticasone propionate and budesonide are widely used in the treatment of chronic obstructive pulmonary disease (COPD).1 The Global Initiative for Chronic Obstructive Lung Disease guidelines recommend ICS in combination with long-acting β2-agonists (LABAs) in moderate to severe COPD to reduce the frequency of exacerbations,2 and current formulations of ICS approved for use in COPD are fluticasone with salmeterol, and budesonide with formoterol. The potential benefits of ICS are counterbalanced by their systemic adverse effects such as pneumonia and their potential to negatively impact bone health.3 4
Prior evidence on the adverse skeletal effects of ICS has been inconsistent. Published evaluations of bone mineral density (BMD) with ICS exposure are limited by considerable losses to follow-up in three large randomised controlled trials (RCTs), with bone density data available only in selected participants.5–7 Two trials (one fluticasone, one budesonide) reported no significant adverse effect on BMD, perhaps due to inadequate statistical power.5 6 In the Towards a Revolution in COPD Health (TORCH) subset, patients on salmeterol had a small gain in spine BMD, as compared with patients receiving salmeterol/fluticasone in combination who had a marginal decrease.5 BMD at the hip fell by 1.7% for salmeterol patients, whereas it fell by 2.9% and 3.2% in the fluticasone and salmeterol/fluticasone groups, respectively.5 In contrast, inhaled triamcinolone (not approved for COPD and no longer marketed) was found to lower BMD significantly.7
A meta-analysis of observational studies found an increased fracture risk among participants with obstructive lung disease,8 whereas other trials5 and their meta-analysis reported no significant effect.9 Thus, the effect of the currently available ICS on the risk of fractures among patients with COPD remains unclear. Our objective was to ascertain systematically the risk of fractures associated with long-term use of ICS compared with control treatments in both trials and real-world studies in patients with COPD.
Methods
Inclusion criteria
Our inclusion criteria for RCTs were (1) parallel-group RCT of at least 24 weeks duration; (2) participants with COPD of any severity; (3) fluticasone or budesonide (which are licensed for use in COPD) as the intervention versus a control treatment, in which the comparison groups consisted of ICS versus placebo, or ICS in combination with a LABA versus a LABA alone; and (4) outcome data (including zero events) on fracture adverse events.
We also evaluated controlled observational studies (case–control, prospective cohort or retrospective cohort) reporting on the risk of fractures with any ICS exposure compared with those without ICS exposure in COPD. Eligible studies had to present ORs, RR/HRs or sufficient data to enable us to calculate the OR.
Exclusion criteria
We excluded trials of <24 weeks duration as we were interested in long-term fracture risk. We also excluded studies evaluating ICS use in acute exacerbations of COPD, or where mixed groups of participants (asthma/COPD) were enrolled but fracture outcomes were not separately reported for each group.
Search strategy
An electronic search (MEDLINE and EMBASE) was originally carried out in April 2009 as part of an earlier systematic review,10 and this search was updated in August 2010 (see the online Appendix 1 for search terms). We examined the websites of the US Food and Drug Administration, and European regulatory authorities, and the manufacturers' clinical trials register of fluticasone11 and budesonide.12 The bibliographies of included studies and Cochrane Systematic Reviews were also used to identify relevant articles.
Study selection
Two reviewers (YKL and RC) independently, and in duplicate, scanned all titles and abstracts that indicated the study was an RCT or observational study evaluating the use of ICS in patients with COPD, and further assessed eligibility after retrieving full text versions of potentially relevant articles.
Study characteristics
We used a prespecified protocol to record study characteristics, diagnostic criteria for COPD, dose and frequency of interventions, mean age, sex and spirometric data of participants, and previous ICS use . The design and relevant data sources, duration of follow-up, the number of study participants and their selection criteria were recorded for the observational studies.
Risk of bias assessment
Two reviewers independently assessed the reporting of blinding, allocation concealment, withdrawals and the loss to follow-up in RCTs. In accordance with recommendations on assessing adverse effects, we extracted information on participant selection, ascertainment of exposure and outcomes, and methods of addressing confounding in observational studies.13 Publication bias was assessed using a funnel plot.
Data extraction
Two reviewers independently extracted data (including zero events) on fractures (where available) from trial listings of ‘Adverse Events’ or ‘Serious Adverse Events’ in the results summaries from the clinical trials register and regulatory documents. In order to avoid duplication, we extracted fracture data based on unique study identifiers where listed. Unpublished reports were subsequently matched to journal manuscripts based on sample size, duration and intervention arms, and additional data extracted where necessary. Authors were contacted for data clarification where needed. Any discrepancies were resolved with 100% agreement after rechecking the source papers and further discussion among the three reviewers.
Statistical analysis
We pooled trial data using Review Manager (RevMan) version 5.1.1 (Nordic Cochrane Center, Copenhagen, Denmark) and calculated the Peto OR, using the recommended approach for meta-analysis of rare adverse events. In situations where the fixed effect model is valid, the Peto OR provides the best CI coverage and has greater statistical power in analysing rare events as compared with the random effects model.14 15 We assessed statistical heterogeneity using the I2 statistic, with I2 >50% indicating a substantial level of heterogeneity.16 If substantial statistical heterogeneity was found, we planned to explore sources of heterogeneity. Predefined sensitivity analyses were performed to check whether different control comparators and alternative statistical models (fixed effect with no continuity correction using StatsDirect software) would substantially change the findings.14 Posthoc sensitivity analyses were performed based on long-term trials of >12 months duration, and trials with clear reporting of methodological components such as randomisation, blinding and follow-up.
The number needed to harm (NNH) (and 95% CI) with ICS was calculated by applying the OR estimates to the control event rate in a large trial population using Visual Rx, version 2.0.17 Herein, the NNH is the number of patients who need to be treated with ICS for an additional patient to be harmed by a fracture.
ORs from the observational studies were pooled separately from the RCTs, using the inverse variance, fixed effect model. We assumed similarity between the RR and OR because fractures were rare events.18 We prespecified the choice of data for analysis, starting preferentially with: (1) current and/or recent users' versus remote users or non-users; (2) use within the past 6 months—1 year versus remote users or non-users; and (3) any exposure versus non-exposure. To estimate a dose–response trend as log ORs across different exposure levels, we used inverse variance-weighted least squares regression to pool studies that reported dose-specific risk estimates with one referent category. The adjusted OR and their CIs, and the dose of ICS as beclomethasone equivalents in each exposure level, were abstracted. We estimated the median dose for each exposure level when only dose ranges were available. We assumed that open-ended exposure levels would follow the same range pattern as the previous levels. The dose–response analysis was carried out in Stata 10.0.
Results
The flow chart of study selection is shown in figure 1. A total of 16 RCTs and seven observational studies fulfilled our inclusion criteria for the meta-anaysis.

Flow diagram of the process of article selection for meta-analysis. COPD, chronic obstructive pulmonary disease; ICS, inhaled corticosteroids.
Randomised controlled trials
Trial characteristics
Characteristics of the included trials are shown in table 1. There were a total of 17 513 participants with COPD, with 9143 on ICS compared with 8370 controls. The duration of the trials ranged from 24 to 156 weeks, with a mean of 90 weeks across studies.6 w1–w15 (Note that references prefixed with ‘w’ can be found in the online supplement.)
Characteristics of randomised controlled trials included in the analysis of fractures
Inhaled fluticasone was evaluated in 14 trials, while inhaled budesonide was used in two trials.6 w14 Trials tended to enrol participants with severe COPD, as the mean forced expiratory volume in 1 s (FEV1) of the participants was <50% for nine of the trials.w1 w3–w5 w7–9 w14 w15 There was a predominance of men (>50% male participants in every trial), with the mean ages typically in the 60–70 year range. Where reported, prior ICS use was noted in 25–50% of the participants, except for two trials with past ICS exposure for ∼20% of patients.w1 w5
Trial quality was variable (table 2). All the RCTs had blinding of participants and personnel. Discontinuation rates varied from no withdrawals to 53%, with some evidence of differentially higher losses in placebo arms.w2 w4 However, many of the patients who discontinued the assigned intervention appeared to remain available for follow-up, as the reported losses only ranged from none to 4.9%. Seven RCTs provided detailed descriptions regarding blinding, adequate sequence generation, allocation concealment and clear reporting of loss to follow-up, and were at low risk of bias.w1–w4 w8 w10 w15 The remaining nine RCTs were at unclear risk of bias owing to lack of clarity in reporting the methods of randomisation.6 w5–w7 w9 w11–w14 None of the trials was designed specifically to evaluate fractures, and the data on fractures were extracted from listings of adverse events, except for subsets of participants in two trials where bone outcomes were measured in detail.5 6 Five trials gave details on systemic corticosteroid use for COPD exacerbations, and four of the trials showed a significantly higher use of oral corticosteroid in the non-ICS intervention arms (online table I).
Risk of bias assessment and fracture outcomes in RCTs of inhaled corticosteroids in COPD
Main findings
Across the mean trial duration of 90 weeks, ICS use was associated with a significant increase in the risk of fractures (180 of 9143 (2.0%) vs 141 of 8370 (1.7%) for control); Peto OR 1.27 (95% CI 1.01 to 1.58; p=0.04) (figure 2). There was no evidence of statistical heterogeneity among the included trials (I2=0%).

Meta-analysis of odds of fracture with inhaled corticosteroid (ICS) exposure trials of patients with chronic obstructive pulmonary disease. LABA, long-acting β2-agonist.
Sensitivity analysis
Fixed effect meta-analysis based on the Mantel–Haenszel model (without a continuity correction) yielded similar findings of an increased OR 1.26 (95% CI 1.01 to 1.59; p=0.04) for fractures in RCTs of ICS in COPD.
The pooled Peto OR for seven trials with complete reporting of quality components was 1.23 (95% CI 0.97 to 1.55),w1–w4 w8 w10 w15 as compared with a Peto OR of 1.73 (95% CI 0.80 to 3.73) for nine trials where some aspects regarding the process of randomisation were not fully reported.6 w5–w7 w9 w11–w14
Restricting the pooled analysis to four long-term trials (each of 156 weeks duration)6 w2 w4 w12 yielded a pooled OR of 1.19 (95% CI 0.94 to 1.51) that is slightly lower than the overall pooled estimate. This may be due to higher quality studies, or change in risk with time. However, the reliability of fracture estimates from long-terms trials such as TORCH is limited by significantly higher oral corticosteroid exposure (online table 1) and withdrawals (with some crossover to ICS treatment) in the placebo arms.19
Publication bias
The funnel plot for fractures appeared to be symmetrical for the RCTs (online figure 1).
Number needed to harm
The NNH for fractures was estimated at 83 (95% CI 38 to 2107) over the 3 year ICS treatment period in the trial, based on the 5.1% fracture rates in the salmeterol and placebo arms for the TORCH trial.5
Observational studies
Details of the included studies and the risk of bias are shown in tables 3 and 4.w27–w33 There were five nested case–control studies,w28 w29 w31–w33 and two cross-sectional studies.w27 w30 Three of the studies were based in the USA,w28–230 while the other four were in Europe.w27 w31–w33 There was a predominance of females in three studies. Fluticasone and/or budesonide were among the ICS evaluated in all the studies, except for one study that evaluated beclomethasone and triamcinolone.w30 ICS exposure was estimated from dispensing records, and dosages were usually extrapolated from amounts dispensed. Some patients were identified through diagnostic codes for COPD in electronic databases, and the extent of misclassification is unclear. Four studies were funded by manufacturers of ICS.w28 w29 w32 w33
Characteristics of observational studies of inhaled corticosteroids (ICS) and fractures
Validity assessment and results of observational studies
Findings from the meta-analysis of observational studies according to exposure subcategories are shown in figure 3. The pooled estimate based on all seven studies, covering current or ever users versus non-users, showed an OR of 1.21 (95% CI 1.12 to 1.32; p<0.0001, I2=37%). There were five studies that reported on current users compared with no current exposure which yielded a pooled OR of 1.27 (95% CI 1.14 to 1.41; p<0.0001; I2=48%).w28–w30 w32 w33 Four studies reported on recent users compared with no recent exposure, with very similar findings of a pooled OR of 1.24 (95% CI 1.12 to 1.37; p<0.0001; I2=29%).w28 w29 w32 w33

Meta-analysis of odds of fracture with subcategories of inhaled corticosteroid exposure in observational studies of patients with chronic obstructive pulmonary disease.
Exclusion of the study that did not enrol fluticasone or budesonide usersw30 did not change the direction or magnitude of the fracture risk for current or ever users (OR 1.21; 95% CI 1.11 to 1.32; p<0.001) in a sensitivity analysis.
One study reported primarily on fluticasone, but provided some data on the category of ‘other ICS’ exposure involving beclomethasone and budesonide. Meta-analysis based on ‘other ICS’ category rather than ‘fluticasone exposure’ yielded a very similar OR of 1.20 (95% CI 1.11 to 1.29).w32
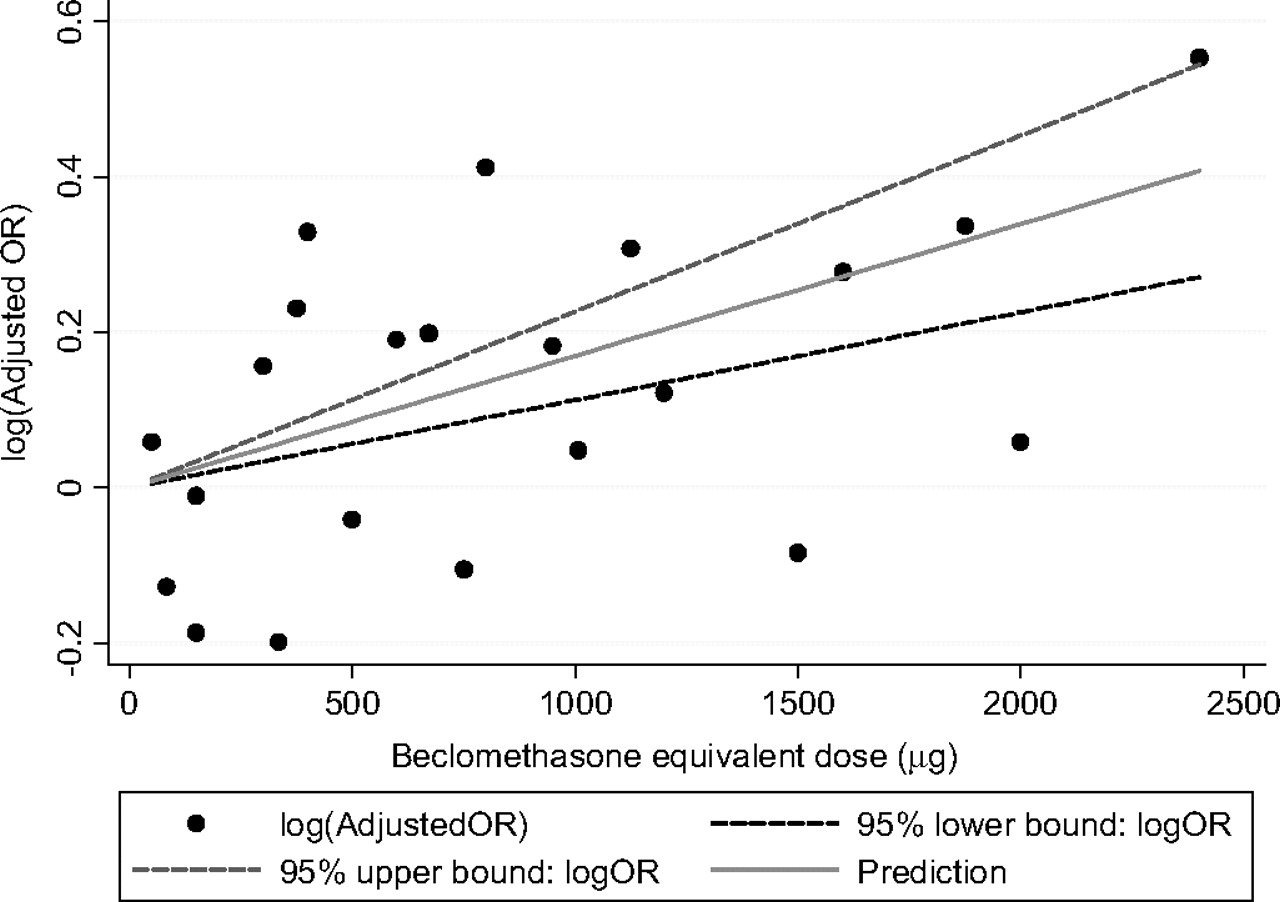
Dose–response meta-regression
Six observational studies were included in this analysis.w27–w29 w31–w33 Each 500 μg increase in beclomethasone dose equivalents was associated with a 9% increase in the likelihood of fractures, OR 1.09 (95% CI 1.06 to 1.12; p<0.001) (figure 4).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Meta-analysis of inhaled corticosteroids versus controls for fractures in observational studies.
Discussion
Our meta-analysis found consistent evidence on the adverse effects of the available long-term ICS (fluticasone and budesonide) treatment on fractures in patients with COPD. We found a relative increase of >20% in the likelihood of fractures in RCTs and observational studies, Although the pooled estimates from the RCTs are dominated by a single large trial, and the lower bounds of the 95% CIs lie very close to unity, the totality of the evidence should be considered. Here, the consistency and similarity of the point estimates across study designs, the absence of statistical heterogeneity and the presence of a dose–response effect in the observational studies strengthen the confidence in this association.
Comparisons with previous analysis
Our consistent findings from trials and observational studies in COPD should be distinguished from previous underpowered meta-analyses limited to published trials, or observational studies which included patients with conditions other than COPD. A meta-analysis of ICS in older adults found no consistent risk based on three COPD trials and several observational studies that enrolled patients who did not have COPD.20 Similarly, another meta-analysis reported no increase in fractures based on published data from three long-term trials.9 There are also two Cochrane reviews that reported inconclusive findings on the link between ICS and fractures.21 22 Another pooled analysis limited to five published case–control studies which included those with other respiratory conditions such as asthma reported a dose-related increased relative fracture risk of 12% per 1000 μg increase in beclomethasone equivalents.8 In contrast, our comprehensive meta-analysis of clinical trials included unpublished data with sufficient power to reliably detect a relatively precise estimate of the increase in the likelihood of fractures among 17 513 patients with COPD.
The precise mechanisms by which ICS increase the risk of fractures in patients with COPD are uncertain. Patients with COPD are already at high risk from osteoporosis and fractures, which may stem from co-morbidity (eg, susceptibility to falls), nutritional deficiencies, inflammatory markers, and prior corticosteroid exposure.23 A small portion of the ICS dose is systemically absorbed and systemic effects are recognised. At large doses, the adverse effects of ICS may come close to that of oral corticosteroids, known to cause increased bone resorption and decreased bone formation in a dose-dependent manner consistent with our dose–response analysis.24
Limitations
The lower limit of the 95% CI for fracture risk from RCT data is close to the threshold of the null effect, thus introducing an element of uncertainty. Moreover, the trial data originate mainly from unpublished, non-peer-reviewed company reports. Absence of information in RCTs regarding timing of fracture in relation to ICS use also precludes meta-regression of fracture risk according to exposure duration. Most of the RCTs did not use specific methods to define and record fractures, and it is possible that misclassification or underascertainment occurred, although this should not have a differential effect in a double-blind study. Many trial participants had previous ICS exposure prior to joining the trial, and we noted differential oral corticosteroid exposure in control arms (online table 1), thus attenuating observable differences between groups.19 While risk estimates from observational data were adjusted for concomitant medications, this was not so for the RCTs, and the extent of bisphosphonate use may affect the fracture risk.5
Data on budesonide are available from only two trials,6 and there are no head to head long-term trials of fluticasone versus budesonide in COPD. We did not specifically evaluate trials of flunisolide, triamcinolone or mometasone as they are not licensed for COPD. Most trial participants were male, and studies were based on older ICS devices, limiting applicability. Observational studies are susceptible to residual confounding.
Future research
Future studies should evaluate the precise location of the fractures (peripheral vs central, traumatic vs non-traumatic), and whether the risk varies by COPD severity. Studies should attempt to determine whether concomitant bone-protective drugs can ameliorate this risk of fractures associated with ICS, and should recruit a larger proportion of postmenopausal women. The risk of fractures associated with the newer formulations of ICS needs to be assessed. The dose–response relationships for efficacy and safety need detailed evaluation so that the lowest effective dose can be prescribed.
Implications for clinical practice
The relative increase of ∼27% in fracture risk should be weighted against the 20–25% relative reduction of COPD exacerbations, with a potential number needed to treat of 6 per year in preventing exacerbations.4 This contrasts with the fracture NNH of 83 over a 3-year period in the same trial population. Thus, the benefit/harm ratio may be less of a concern for patients with low underlying fracture risk but who have more severe COPD and are experiencing frequent exacerbations. However, as cumulative ICS exposure may be hazardous in older patients with multiple co-morbidities and low BMD, ICS treatment needs more careful consideration, and bone-protective drugs may be warranted.
Conclusions
Our findings suggest a dose-dependent increased risk of fractures associated with the long-term use of inhaled fluticasone or budesonide in patients with COPD. Clinicians should carefully consider the modest risk of fractures associated with ICS treatment, along with their adverse effects on other outcomes and balance this against the symptomatic benefits in reducing exacerbations.
References
Supplementary materials
Web Only Data thx.2011.160028
Files in this Data Supplement:
Footnotes
Funding SS is supported by the Johns Hopkins Clinical Research Scholars Program. This publication was made possible by Grant Number 1KL2RR025006-03 from the National Center for Research Resources (NCRR), a component of the National Institutes of Health (NIH), and NIH Roadmap for Medical Research. Its contents are solely the responsibility of the authors and do not necessarily represent the official view of the NCRR or NIH. Information on the NCRR is available at http://www.ncrr.nih.gov/. Information on Re-engineering the Clinical Research Enterprise can be obtained from http://nihroadmap.nih.gov/clinicalresearch/overview-translational.asp.
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.