Article Text

Abstract
Background Hospitalisations and their sequelae comprise key morbidities in the natural history of chronic obstructive pulmonary disease (COPD). A study was undertaken to examine the associations between lung function impairment and COPD hospitalisation, and COPD hospitalisation and mortality.
Methods The analysis included a population-based sample of 20 571 participants with complete demographic, lung function, smoking, hospitalisation and mortality data, with 10-year median follow-up. Participants were classified by prebronchodilator lung function according to the modified Global Initiative on Obstructive Lung Disease (GOLD) criteria. Hospitalisations were defined by the presence of a COPD discharge diagnosis (ICD-9 codes 490–496). Incidence rate ratios (IRR) of COPD admissions and hazard ratios (HR) of mortality with respective 95% CI were calculated, adjusted for potential confounders.
Results The prevalence of modified GOLD categories was normal (36%), restricted (15%), GOLD stage 0 (22%), GOLD stage 1 (13%), GOLD stage 2 (11%) and GOLD stages 3 or 4 (3%). Adjusted IRRs (and 95% CI) indicated an increased risk of COPD hospitalisation associated with each COPD stage relative to normal lung function: 4.7 (3.7 to 6.1), 2.1 (1.6 to 2.6), 3.2 (2.6 to 4.0), 8.0 (6.4 to 10.0) and 25.5 (19.5 to 33.4) for the restricted, GOLD stage 0, GOLD stage 1, GOLD stage 2 and GOLD stages 3 or 4, respectively. Hospitalisation for COPD increased the risk of subsequent mortality (HR 2.7, 95% CI 2.5 to 3.0), controlling for severity, number of prior hospitalisations and other potential confounders. The increase in mortality associated with admission was very similar across the modified GOLD stages.
Conclusions COPD severity was associated with a higher rate of severe exacerbations requiring hospitalisation, although severe exacerbations at any stage were associated with a higher risk of short-term and long-term all-cause mortality.
- Pulmonary disease
- chronic obstructive
- hospitalisation
- mortality
- epidemiology
- clinical epidemiology
- COPD epidemiology
- COPD exacerbation
Statistics from Altmetric.com
- Pulmonary disease
- chronic obstructive
- hospitalisation
- mortality
- epidemiology
- clinical epidemiology
- COPD epidemiology
- COPD exacerbation
Chronic obstructive pulmonary disease (COPD) is responsible for a significant medical and economic burden in the USA and is expected to be the third leading cause of worldwide mortality by the year 2020.1 In 2000 in the USA 726 000 people were hospitalised for an exacerbation of COPD, with people aged >65 years responsible for more than one-half of these.2 Almost 120 000 people in the USA died with COPD as the underlying cause of death in 2000.2 However, this number may actually be higher because many decedents with COPD have their deaths attributed to other causes,3 and serious comorbid conditions are common in this population.4–6
Acute exacerbations of COPD frequently result in hospital admission and account for a large proportion of the clinical, economical and social impact of this disease, including an increased risk of mortality. Impaired lung function has been identified as a risk factor of hospital admission due to a COPD exacerbation in several studies including different settings, designs and methods, and independent of respiratory symptoms, quality of life or blood gas exchange.7–12 Unfortunately, the limited sample size and/or the narrow variability in lung function has not allowed previous studies to quantify the increase in the risk of COPD admissions associated with a range of impaired lung function levels.
Previous studies of hospitalisations and outcomes have focused on in-hospital mortality,6 13 rehospitalisations and/or resource utilisation14–16 or mortality at short periods of time (≤2 years).16–19 In these studies the demographic data were limited,20 the range of lung function impairment was narrow and cohorts consisted of relatively small numbers of only previously-diagnosed patients with COPD. Additionally, the influence of COPD admissions and COPD severity stage on mortality risk has never been quantitatively assessed.
The goal of this study was to examine the associations between (1) lung function impairment and COPD hospitalisation, and (2) COPD hospitalisation and mortality in two large diverse population-based cohorts. This design allows us to determine the characteristics of the population admitted to hospital for severe COPD events and to profile the short- and long-term outcomes related to these events. Such information can identify higher risk subgroups for whom targeted interventions and monitoring may be warranted.
Methods
Study population
For this analysis we combined data from the Cardiovascular Health Study (CHS) and Atherosclerosis Risk in Communities (ARIC) cohorts, both of which were population-based NIH cohorts initiated in the late 1980s to study risk factors for the development and progression of heart disease and stroke. These cohorts included subjects of different ages (≥65 years for CHS and 45–64 years for ARIC) and had comprehensive evaluations including lung function and longitudinal follow-up. Combining these two cohorts into one larger study population provides data over a wider age range, better reflecting the US adult population.
The CHS cohort consisted of 5201 subjects selected using Medicare eligibility lists provided by the US Healthcare Financing Administration for four communities: Forsyth County, North Carolina; Pittsburgh, Pennsylvania; Sacramento County, California; and Washington County, Maryland from May 1989 to May 1990. Subjects completed a questionnaire (including information on respiratory symptoms and diagnoses, medical history and smoking status), clinical examination and underwent spirometric testing at baseline and 4 years. They were followed through to the end of 1999. Details of the CHS are published elsewhere.21
The ARIC study was initiated in 1987 as a longitudinal population-based study of the aetiology and clinical sequelae of atherosclerosis in 15 792 adults. Study protocols were approved for protection of human subjects. Participants were selected from the entire population by probability sampling from four US communities: Forsyth County, NC; Minneapolis, MN; Washington County, MD; and Jackson, MS (where only African Americans were sampled), and followed through 1998. Specific details of the ARIC study are published elsewhere.22
Our analysis was limited to CHS or ARIC participants who provided baseline information on respiratory symptoms and diagnoses, medical history and who underwent adequate pulmonary function testing at the baseline examination. There were no differences in age or gender between subjects included and those excluded because of missing data (n=216 in CHS, n=206 in ARIC).
Variables and instruments
In both studies, spirometry was conducted using a volume-displacement water-sealed spirometer. At least three acceptable spirograms were obtained from a minimum of five forced expirations. The best single spirogram was identified by computer and confirmed by a technician. Quality assurance was provided by the CHS Pulmonary Function Center for CHS and the ARIC investigators for ARIC, and the procedures followed contemporary American Thoracic Society guidelines.23 Several measures of lung function were used in this analysis: forced expiratory volume in 1 s (FEV1), forced vital capacity (FVC) and the FEV1/FVC ratio. We used the prediction equations derived from the Third National Health and Nutrition Examination Survey to define the predicted values of FEV1 and FVC.24 We defined a subject as having a respiratory symptom if they reported cough, phlegm, dyspnoea or wheeze.
A modification of the GOLD criteria was used to classify subjects according to their stage of COPD25 26: GOLD stages 3 or 4 (FEV1/FVC <0.70 and FEV1 <50% predicted), GOLD stage 2 (FEV1/FVC <0.70 and FEV1 ≥50 to <80% predicted), GOLD stage 1 (FEV1/FVC <0.70 and FEV1 ≥80% predicted), restricted (FEV1/FVC ≥70% and FVC <80% predicted), GOLD stage 0 (presence of respiratory symptoms in the absence of any lung function abnormality) and no lung disease (table 1). Bronchodilator response was not evaluated so classification is based on the ‘prebronchodilator’ level. Only the baseline pulmonary function data were used to stratify participants, and they remained in these groups for interpretation of prevalent risk and incident or recurrent events.
Characteristics of the study population from the Atherosclerosis Risk in Communities Study (ARIC) 1986–9 and Cardiovascular Health Study (CHS) 1989–90, with median follow-up of 10 person-years
Age, sex, race (white or black) and highest education level (<12 years, 12 years or >12 years) obtained were self-reported. Respondents with positive responses to the questions ‘Have you ever smoked cigarettes?’ and ‘Do you now smoke cigarettes?’ were classified as never, former or current smokers, respectively. A modification of the Baecke questionnaire was used to assess physical activity.27 28 We added the three components (work, leisure and sports indices) and divided the subjects into four quartiles of least to most active. Body mass index (BMI) was calculated as weight divided by height squared (kg/m2).29 Subjects were classified as having diabetes if they either reported a diagnosis of diabetes at baseline or had elevated fasting or post-glucose load glucose levels at the baseline examination. Subjects reporting a diagnosis of a previous myocardial infarction, stroke, heart failure, angina or transient ischaemic attacks were classified as having cardiovascular disease at the baseline examination.
Outcomes
Hospitalisation discharge data were searched and COPD events were defined as any hospitalisations occurring during follow-up that included a COPD or related condition (ICD-9 code 490–496) discharge code. Mortality data were obtained from death certificates. Only all-cause mortality was considered.
Statistical analysis
Data from the ARIC and CHS cohorts were pooled. A variable indicating study source (ARIC or CHS) was included as a potential confounder or effect modifier in all the analyses that follow. Characteristics of the study population were described as number and percentage. For each subject group, total person-years of follow-up and death rate (number of deaths/1000 person years) were calculated.
Kaplan–Meier curves of time to first COPD admission were plotted according to the modified GOLD stage and the stages were compared using the log rank test. The crude and adjusted associations between modified GOLD stage and COPD hospitalisation rate were assessed using zero-inflated negative binomial regression, and goodness of fit was tested. The following variables were tested as potential confounders: age (as a continuous), gender, education, race, smoking, physical activity, BMI (in four categories), diabetes and heart disease. Variables were included in the final model if they were independently related to the outcome or the exposure, or modified estimates for the remaining variables by at least 15%. Respiratory symptoms were not considered as potential confounders due to their overlap with the GOLD stage 0 definition.
Kaplan–Meier curves of time to death were plotted according to incident COPD hospitalisation status and compared using the log rank test. The crude and adjusted association between COPD hospitalisation and mortality were analysed by means of parametric tests using exponential distribution, adjusting for confounders, and including previous COPD hospitalisations as a time-varying exposure. The final model was further stratified according to modified GOLD stage.
All analyses were conducted with SAS Version 9.1 (SAS Institute), SUDAAN version 9.0 (RTI, Research Triangle Park, NC) and STATA release 10.0 (StataCorp LP, 2008).
Results
A total of 20 571 subjects (15 586 from ARIC and 4985 from CHS) were included: 56% women, mean age 59 years, with 35% former and 24% current smokers. The prevalence of modified GOLD categories was: normal (36%), restricted (15%), GOLD stage 0 (22%), GOLD stage 1 (13%), GOLD stage 2 (11%) and GOLD stages 3 or 4 (3%). The proportion of former and current smokers was higher in GOLD stages 1–4, while never smokers were more predominant in normal, restricted or GOLD stage 0 subjects. Clinical and demographic data describing the analysis cohort, including exacerbation and mortality rates, are shown in table 1.
A total of 1537 subjects (7%) had at least one COPD admission during follow-up. Among those hospitalised, the median rate of admission was 0.20/year (p25–p75: 0.10–0.44). Figure 1 shows that each of the GOLD stages, including GOLD 0 and restricted, had an increased risk of COPD admission compared with the normal group (p<0.001, log-rank test). After adjusting for potential confounders, the risk of an incident COPD hospitalisation (IRR and 95% CI) by COPD stage was 4.7 (3.7 to 6.1), 2.1 (1.6 to 2.6), 3.2 (2.6 to 4.0), 8.0 (6.4 to 10.0) and 25.5 (19.5 to 33.4) for the restricted, GOLD stage 0, GOLD stage 1, GOLD stage 2 and GOLD stages 3 or 4 categories, respectively (table 2).

Time to first hospitalisation for chronic obstructive pulmonary disease (COPD) by modified Global Initiative on Obstructive Lung Disease (GOLD) stage. Modified GOLD stages: normal (no lung disease), restricted (FEV1/FVC ≥0.70 and FVC <80% predicted), GOLD stage 0 (presence of respiratory symptoms in the absence of any lung function abnormality), GOLD stage 1 (FEV1/FVC <0.70 and FEV1 ≥80%), GOLD stage 2 (FEV1/FVC <0.70 and FEV1 ≥50% to <80% predicted) and GOLD stages 3 or 4 (FEV1/FVC <0.70 and FEV1 <50% predicted).
Crude and adjusted* risk (incidence rate ratio, IRR) of incident hospitalisations for chronic obstructive pulmonary disease
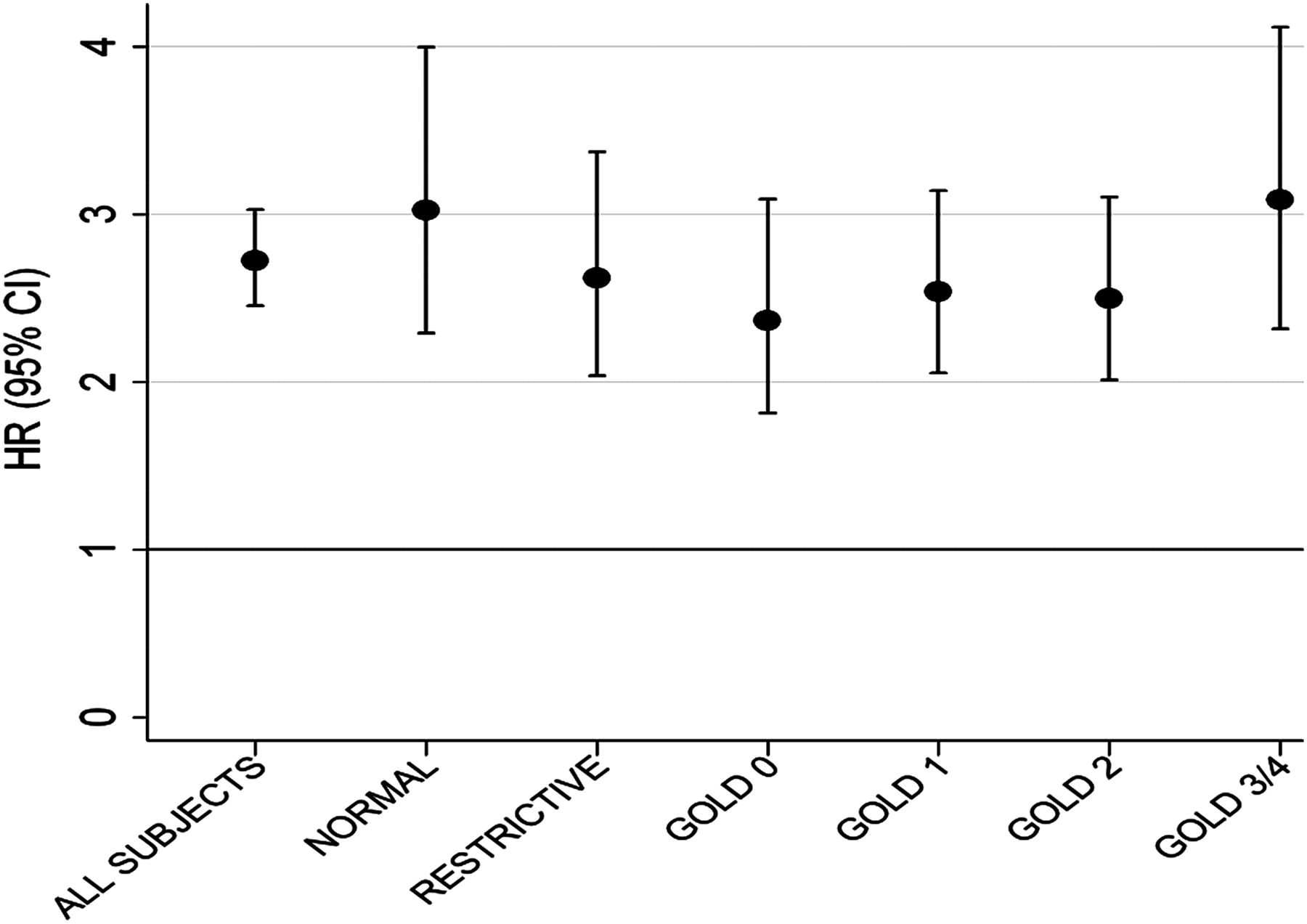
Figure 2 shows the risk of death in study subjects with and without a COPD-related admission. Having had a COPD admission increased the risk of all-cause mortality in the study sample (HR 14.3 (95% CI 13.0 to 15.7), p<0.001). This association was reduced but still remained statistically significant after adjusting for modified GOLD stages, previous COPD admissions (as a time-varying variable) and other confounders (table 3). The magnitude of the association between having a COPD admission and mortality was higher than the estimates for any of the modified GOLD stages except for GOLD stages 3 or 4 (table 3). Figure 3 shows that the increase in mortality associated with admission was very similar across the modified GOLD stages. All results were unchanged after stratifying according to study source (ARIC or CHS).
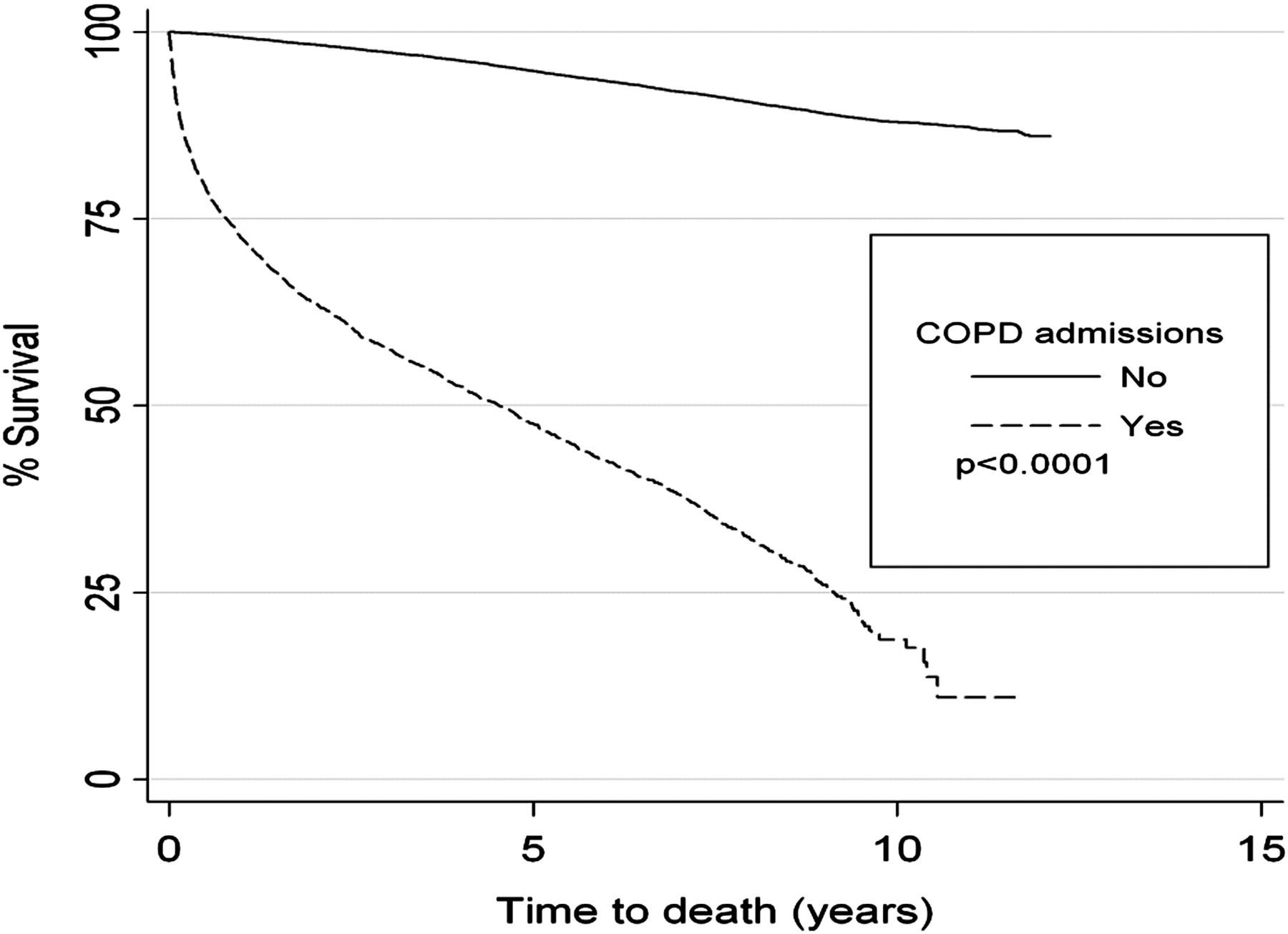
Time to death by having had at least one previous admission for chronic obstructive pulmonary disease (COPD).
Adjusted risk (HR) of all-cause mortality associated with incident hospitalisation for chronic obstructive pulmonary disease (COPD), controlling for COPD disease severity

{kind=link}
{kind=link}
{kind=link}
Risk of all-cause mortality over a median 10-year follow-up period associated with COPD hospitalisation (adjusted* HR and 95% CI), stratified by modified Global Initiative on Obstructive Lung Disease (GOLD) stage group. *Parametric survival regression model also adjusted for previous COPD admissions, age, gender, education, race, smoking, physical activity, body mass index, diabetes, heart disease and cohort (Atherosclerosis Risk in Communities Study/Cardiovascular Health Study). Modified GOLD stages: normal (no lung disease), restricted (FEV1/FVC ≥0.70 and FVC <80% predicted), GOLD stage 0 (presence of respiratory symptoms in the absence of any lung function abnormality), GOLD stage 1 (FEV1/FVC <0.70 and FEV1 ≥80%), GOLD stage 2 (FEV1/FVC <0.70 and FEV1 ≥50% to <80% predicted) and GOLD stages 3 or 4 (FEV1/FVC <0.70 and FEV1 <50% predicted).
Discussion
This analysis of large population-based cohorts had two key findings. The first was that the degree of lung function impairment at baseline was independently associated with the risk of subsequent COPD-related hospitalisations (figure 1, table 2). Of note, this finding was also observed in subjects who did not meet the traditional criteria for COPD—that is, those who had respiratory symptoms at baseline in the absence of lung function impairment (GOLD stage 0) and those who had a normal FEV1/FVC but an FEV1 or FVC <80% of their predicted value (restricted spirometry). The second and more novel finding was that a COPD-related hospitalisation at any level of baseline lung function impairment predicted subsequent mortality that was similar across the differing levels of lung function impairment (figure 3).
This population-based study offers unique information compared with others in the published literature by not requiring the presence of COPD or other lung function impairment for study entry.15 30 Thus, COPD-related hospitalisations could be measured in adults with ‘normal’ lung function at baseline and comprised 9% of the cohort with at least one COPD hospitalisation (table 1). If one combines this group with the GOLD stage 0 group and the restricted group, about 34% of the cohort in whom at least one incident COPD hospital admission occurred did not meet traditional spirometric definitions of COPD at baseline. There are several possible explanations for this finding. Some of these hospital admissions could represent misdiagnosis or miscoding of the underlying lung disease. Several studies have demonstrated poor documentation of lung function in hospitalised patients with a COPD diagnosis.31 Some of these hospital admissions could represent subtypes of COPD—for example, patients with normal flows but impaired diffusion and radiographic evidence of emphysema or those with evidence of air trapping but no airflow limitation.32 Other hospital admissions could represent incident cases: patients whose lung function rapidly declined over a very short period of time. While the traditional view of the natural history of COPD views accelerated loss of lung function as being 60–90 ml annually of FEV1, some patients have exhibited changes in their FEV1 that far exceed this level.33 34
Our analysis reported a 50% mortality rate within 5 years following a COPD hospitalisation (figure 2). These results are comparable to other studies which have observed a 23% mortality rate at 1 year,35 a 35.6% mortality rate at 2 years36 and a 51.1% mortality at 5 years15 in different populations. A novel finding in this analysis, however, is that the association between COPD-related hospitalisation and subsequent mortality was consistently increased, regardless of the level of baseline lung function. This finding highlights the importance of COPD-related hospitalisations as key sentinel events in the lives of patients with COPD which ultimately impacts the most important outcome of survival.
In COPD and other chronic diseases characterised by exacerbations, such as congestive heart failure, each severe event that results in a hospitalisation has the potential to be lethal during the acute event. Our results expand this concept, however, by suggesting that an increased risk of death persists after each acute event, irrespective of the number of previous events. The possible explanations of this finding include debilitation that results during and after the hospitalisation,37 development of additional comorbid disease38 or that hospitalisation represents a surrogate marker for a poor functional status that increases mortality risk.39
This study has a number of limitations. Lung function was classified based on prebronchodilator measurements as bronchodilators were not administered in the ARIC and CHS studies. This may have resulted in the misclassification of some study subjects. In addition, we only used the baseline lung function and respiratory symptoms to classify subjects, raising the possibility that these predictors may have changed over time. Hospitalisation codes were not independently validated, with the possibility of further misclassification.
Conclusion
This analysis of a population-based cohort shows that impaired lung function—including mild COPD (GOLD stage 1), restriction on spirometry and respiratory symptoms in the presence of normal lung function—is associated with an increased risk of COPD-related hospitalisation during follow-up. Furthermore, the presence of a COPD-related hospitalisation was independently associated with risk of death regardless of the baseline level of lung function impairment. These findings highlight the critical importance of these severe exacerbation events in the lives of our patients. Additional epidemiological studies are warranted to understand better the factors that increase mortality so dramatically after a COPD hospitalisation. Clinically, patients who have experienced a COPD-related hospitalisation have an increased risk of death after discharge and their disease needs to be treated as aggressively as other sentinel events, such as an acute myocardial infarction, in order to improve outcomes.
Acknowledgments
The authors thank the staff and participants in the Atherosclerosis Risk in Communities Study and the Cardiovascular Health Study for their important contributions.
References
Footnotes
Funding This study was funded by a research grant from GlaxoSmithKline. JG-A has a researcher contract from the Instituto de Salud Carlos III (CP05/00118), Ministry of Health, Spain. The Atherosclerosis Risk in Communities (ARIC) Study and Cardiovascular Health Study (CHS) are conducted and supported by the National Heart Lung and Blood Institute (NHLBI) in collaboration with the ARIC and CHS Investigators. This paper was not prepared in collaboration with investigators of the ARIC or the CHS and does not necessarily reflect the opinions or views of the ARIC investigators, CHS investigators or the NHLBI.
Competing interests DMM has served as a consultant to GlaxoSmithKline, Novartis, Pfizer, Forest, Astra-Zeneca and Boehringer-Ingelheim and has received research funding from GlaxoSmithKline, Novartis, Pfizer and Boehringer-Ingelheim. DPM was an employee of GlaxoSmithKline when this manuscript was developed. KJD is a current employee of GlaxoSmithKline. The other authors have no competing interests.
Provenance and peer review Not commissioned; externally peer reviewed.