Article Text

Abstract
Background Anaerobic bacteria are increasingly regarded as important in cystic fibrosis (CF) pulmonary infection. The aim of this study was to determine the effect of antibiotic treatment on aerobic and anaerobic microbial community diversity and abundance during exacerbations in patients with CF.
Methods Sputum was collected at the start and completion of antibiotic treatment of exacerbations and when clinically stable. Bacteria were quantified and identified following culture, and community composition was also examined using culture-independent methods.
Results Pseudomonas aeruginosa or Burkholderia cepacia complex were detected by culture in 24/26 samples at the start of treatment, 22/26 samples at completion of treatment and 11/13 stable samples. Anaerobic bacteria were detected in all start of treatment and stable samples and in 23/26 completion of treatment samples. Molecular analysis showed greater bacterial diversity within sputum samples than was detected by culture; there was reasonably good agreement between the methods for the presence or absence of aerobic bacteria such as P aeruginosa (κ=0.74) and B cepacia complex (κ=0.92), but agreement was poorer for anaerobes. Both methods showed that the composition of the bacterial community varied between patients but remained relatively stable in most individuals despite treatment. Bacterial abundance decreased transiently following treatment, with this effect more evident for aerobes (median decrease in total viable count 2.3×107 cfu/g, p=0.005) than for anaerobes (median decrease in total viable count 3×106 cfu/g, p=0.046).
Conclusion Antibiotic treatment targeted against aerobes had a minimal effect on abundance of anaerobes and community composition, with both culture and molecular detection methods required for comprehensive characterisation of the microbial community in the CF lung. Further studies are required to determine the clinical significance of and optimal treatment for these newly identified bacteria.
- Cystic fibrosis
- anaerobe
- infection
- molecular detection
- exacerbation
- bacterial infection
- bronchiectasis
- cystic fibrosis
Statistics from Altmetric.com
- Cystic fibrosis
- anaerobe
- infection
- molecular detection
- exacerbation
- bacterial infection
- bronchiectasis
- cystic fibrosis
Chronic bacterial pulmonary infection with recurrent infective exacerbations results in an irreversible decline in lung function in patients with cystic fibrosis (CF) and early death.1 Routine bacterial culture methods identify the aerobic bacteria Pseudomonas aeruginosa, Staphylococcus aureus and Burkholderia cepacia complex2 as the principal pathogenic bacteria in adult CF pulmonary infection.
The observation that anaerobic conditions exist in the lungs of patients with CF3 has prompted the search for infection in CF mucus by obligate anaerobes. Studies using molecular detection by PCR and terminal restriction fragment length polymorphism analysis (T-RFLP) suggest that anaerobes are present in CF sputum and are part of a highly diverse and metabolically active polymicrobial community.4–7 In a recent study we used strict anaerobic bacteriological culture techniques and detected a spectrum of potentially pathogenic anaerobic species including Prevotella, Veillonella and Actinomyces in high numbers (up to 9×107 cfu/g sputum) from 42/66 (64%) sputum samples collected from patients with clinically stable CF.8 Subsequent culture9 10 and molecular-based9 11 12 studies have also detected anaerobes in lower airway secretions from adults and children with stable CF, indicating that anaerobes may contribute at all stages of CF lung disease. Anaerobic bacteria are therefore potentially significant pathogens in CF lower respiratory tract infection and their role in disease progression may have been underestimated.8 11
If anaerobic bacteria are active and contribute to infection and inflammation in the CF lung, their presence in high numbers may require a change in the antibiotics used for treatment of pulmonary exacerbations to ensure an optimal outcome for the patient. In this study we assessed both aerobic and anaerobic bacterial community composition at initiation and completion of standard antibiotic treatment of an acute exacerbation. Furthermore, to evaluate the effect of antimicrobial therapy on these diverse organisms, we studied longitudinal changes in bacterial load and diversity during exacerbation and when clinically stable. Given that the majority of bacterial species are refractory to culture,13 we also compared the use of both aerobic and anaerobic culture and culture-independent molecular techniques for determining microbial community composition.
Methods
Patient selection and collection of samples
During a 12-month period (February 2006 to January 2007), patients who had a pulmonary exacerbation in the previous year were recruited to the study either during an outpatient visit if they were clinically stable or on admission to the hospital for antibiotic treatment of an exacerbation. Subsequent samples were collected when these patients presented with an exacerbation or at their next routine outpatient visit, respectively. ‘Clinically stable’ was defined as no change in symptoms, forced expiratory volume in 1 s (FEV1) within 10% of best value in the previous 6 months and no new antibiotics started. Exacerbations were defined according to the criteria of Fuchs et al.14 For patients with an exacerbation, samples were collected at initiation of antibiotics (24 h before to a maximum of 48 h after the first dose of intravenous antibiotics) and at completion of antibiotic treatment (24 h before to a maximum of 48 h after last dose of intravenous antibiotics).
Spontaneously expectorated sputum was collected and transported within 15 min to the laboratory for processing in an anaerobic cabinet. All samples were divided with one aliquot immediately processed for culture and the second aliquot frozen and stored at −80°C for subsequent molecular detection at the University of North Carolina at Chapel Hill.
Bacterial culture detection
Culture and subsequent detection of isolates in sputum samples was performed as previously described8 with all bacteria detected quantified by total viable count (TVC) and identified by PCR and sequencing of 16S ribosomal genes, a frequently used alternative to phenotypic methods of bacterial identification.15
Molecular detection
Detailed procedures for molecular-based bacterial detection are provided in the online supplement. Briefly, DNA was extracted from frozen (−80°C) sputum samples and subjected to both quantitative real-time PCR (qPCR) analysis to determine total bacterial load and terminal restriction fragment length polymorphism analysis (T-RFLP) to assess bacterial diversity and for classification of bacterial taxa.16 17 For qPCR, samples were analysed in duplicate at three different concentrations using a previously published16 set of universal primers and TaqMan probe that amplify a conserved fragment of the bacterial 16S ribosomal RNA (rRNA) gene. For T-RFLP analysis, the 16S rRNA gene was PCR amplified using Bac8f and Bac926r primers fluorescently labelled at the 5′ end. The resulting PCR products were digested in two separate reactions with the restriction endonucleases HaeIII and HhaI and the length of labelled terminal fragments was determined by capillary electrophoresis.
Patient characteristics
For each patient, sex, age, weight, lung function (FEV1) and serum inflammatory markers (C reactive protein (CRP), white cell count (WCC)) were obtained at each time point. Information on intravenous antibiotics for treatment of an acute exacerbation was also collected.
Statistical analysis
A detailed description of the statistical methods is provided in the online supplement. Briefly, participant characteristics before and after antibiotic treatment were compared using paired samples t test or Wilcoxon signed rank tests as appropriate. Kappa statistics were calculated to measure agreement between the presence or absence of bacteria detected by culture and T-RLFP. Viable counts were compared at each time point and before and after antibiotic treatment using Wilcoxon signed rank tests. Comparison between three time points simultaneously were made using the Friedman test. The log10 qPCR was compared before and after treatment using a paired samples t test.
Results
Patient characteristics and sputum samples
Twenty-three patients were enrolled and sputum samples were collected at initiation and completion of intravenous antibiotic treatment. The mean age was 24.9 years (range 18–41). Three of the patients were treated twice for an exacerbation during the course of the study resulting in a total of 26 matched pairs of initiation/completion of treatment samples. Sputum was also collected from 13 of these patients (mean age 27.0 years (range 19–41)) when clinically stable, with seven samples collected before exacerbation, five samples collected after exacerbation and one sample collected between treatment of two separate exacerbations. The mean time interval between collection of stable and exacerbation sputum samples was 155 days (range 19–281) and 137 days (range 15–231) for samples collected after exacerbation.
Patient characteristics are presented in table 1. The mean duration of intravenous antibiotic therapy was 13 days (range 7–24), with all patients improving clinically. Lung function (FEV1) increased significantly by an average of 0.4 l and CRP and WCC decreased significantly following antibiotic treatment of an exacerbation by medians of 7.6 μg/dl and 2.5×109/l, respectively (table 1). Owing to the wide range of antibiotic regimens used to treat exacerbations (see table 1 in online supplement) and the small sample size, we were unable to determine if there was a relationship between use of specific antibiotics and change in anaerobic bacterial load following treatment. Patients primarily received oral azithromycin or inhaled colistin or tobramycin as chronic maintenance treatment. Similarly, owing to the small sample size, we were unable to determine if there was any correlation between antibiotic prophylaxis and presence/absence of any particular bacterial species.
Patient characteristics at the start and completion of antibiotic treatment for an exacerbation and when stable
Bacterial culture and identification of isolates
The predominant aerobic pathogens were present in high abundance (up to 5×108 cfu/g sputum) in 24/26 samples at the start of treatment (P aeruginosa, 16; B cepacia complex, 8), 22/26 at completion of treatment (P aeruginosa, 15; B cepacia complex, 7) and 11/13 stable samples (P aeruginosa, 9; B cepacia complex, 2) (see figure 1a in online supplement and table 2). Only one patient (patient 19), who experienced two exacerbations during the study period, had neither P aeruginosa nor B cepacia complex cultured in the sputum at all five time points. Furthermore, P aeruginosa was cultured from one patient (patient 7) when stable and at initiation of antibiotic treatment but not at completion of treatment. Similarly, B cepacia complex was cultured from one patient (patient 3) at initiation but not at completion of antibiotic treatment. With these exceptions, the patients had the same aerobic bacteria in sequential sputum samples (see figure 1a and table 3 in online supplement).
Bacteria detected by culture and molecular analysis (terminal restriction fragment length polymorphism, T-RFLP) in sputum samples (n=64) collected from adult patients with cystic fibrosis
Anaerobic bacteria were detected in high numbers (up to 3×107 cfu/g sputum) in samples from all patients prior to commencing antibiotic therapy with up to five different species detected per sputum sample (see figure 1a in online supplement). Of the anaerobes detected, Veillonella species (14 samples) and Prevotella species (6 samples) were predominant. At completion of antibiotic treatment, anaerobic bacteria were detected by culture in 23/26 samples, with Veillonella (14 samples) and Prevotella (7 samples) again most prevalent. Anaerobic bacteria were also detected in all 13 samples from stable patients, with Veillonella (2 samples), Actinomyces (3 samples) and Prevotella (2 samples) species being the most common. Streptococci, which grew under either aerobic or anaerobic conditions, were detected by culture in 12 and 7 initiation and completion of treatment samples, respectively. Overall, culture results showed that, although the composition of the bacterial community varied between patients, it remained relatively stable within the majority of individuals despite antibiotic treatment, with similar numbers and genera of aerobic and anaerobic species detected at each sampling time point (see figure 1 and online table 3).
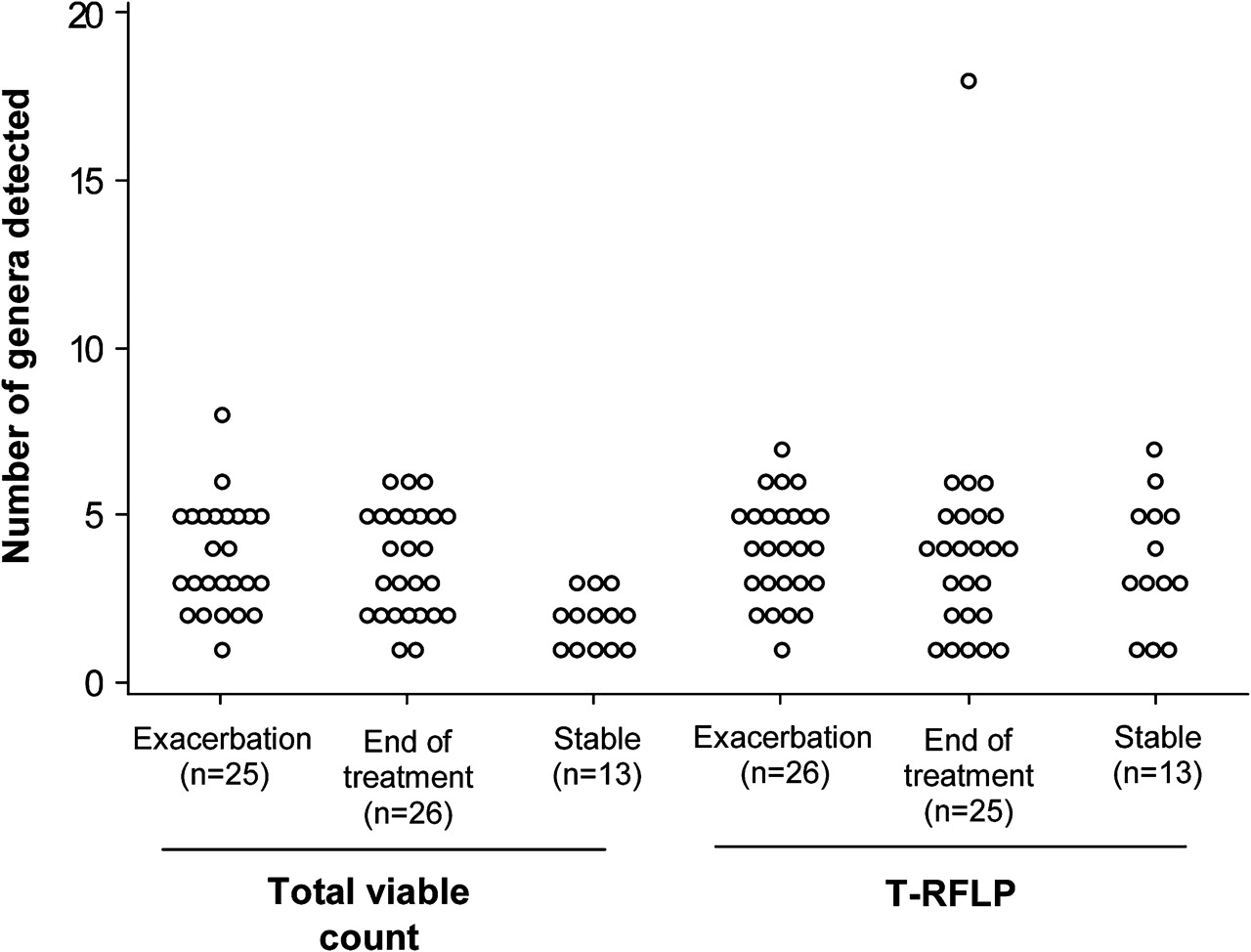
Number of genera detected by culture and terminal restriction fragment length polymorphism analysis (T-RFLP) in sputum samples collected from adult patients with cystic fibrosis at initiation (Exacerbation) and completion of intravenous antibiotic treatment (End of Treatment) for an exacerbation and when stable (Stable).
Culture-independent T-RFLP detection of microbial community composition and comparison with total viable counts from culture data
The composition of the bacterial community was also analysed in 64 sputum samples by T-RFLP (see online figure 1b and online table 3). In general, all samples contained numerous terminal restriction fragments indicating that bacterial diversity within sputum samples was greater than detected by culture. In order to compare culture and T-RFLP results, T-RFLP patterns for each sample were compared with the patterns generated from 16S rRNA gene clones (see table 2 in online supplement) representing 22 genera frequently detected in CF sputum. Based on this comparison, organisms belonging to the 22 genera were predicted to be present a total of 251 times among the 64 samples (figure 1 and table 2).
The predominant aerobic pathogens (Pseudomonas and Burkholderia) detected by culture were predicted by T-RFLP to occur in the corresponding patient samples (see figure 1b in online supplement). Strict anaerobes were predicted by T-RFLP in 22/26 admission samples, 20/25 completion of treatment samples and 9/13 stable samples with up to eight different anaerobic genera detected in a single sputum sample. Similar to the culture results, Veillonella and Prevotella were frequently detected. In addition, a number of anaerobic genera were detected exclusively by T-RFLP in multiple samples including Granulicatella (45/64), Porphyromonas (6/64) and Pasteuriaceae (5/64). Consistent with the culture-based results, molecular detection also showed that the composition of the bacterial community remained relatively stable in the majority of patients with similar T-RFLP patterns generated (see figure 1b in online supplement) and similar numbers and genera of both aerobic and anaerobic species detected. Individual spectra taken at different time points from the same patient were comparable, demonstrating the reproducibility of the method (see figure 2 in online supplement).
The agreement between the presence or absence of bacteria from the T-RFLP spectra and TVCs from culture was relatively good for aerobic bacteria such as P aeruginosa (κ=0.74) and B cepacia complex (κ=0.92) but poor for Streptococcus (κ=0.05) and anaerobic genera such as Veillonella (κ=0.14) and Prevotella (κ=0.00).
Comparison of aerobe and anaerobe viable counts and effect of antibiotic treatment on bacterial abundance
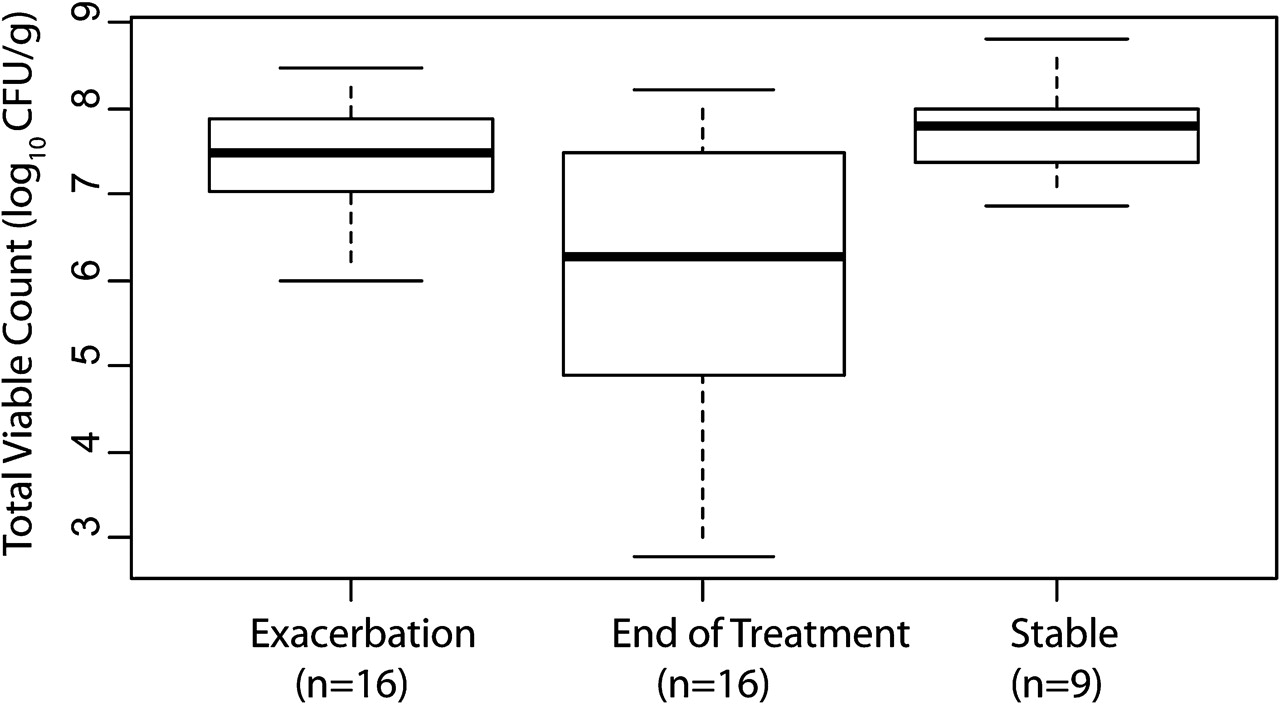
Aerobic bacteria, cultured under the conditions used, were present in significantly greater numbers than anaerobes in samples at initiation of antibiotic treatment (median difference in TVC 4.9×107 cfu/g (95% CI 1.8×107 to 14.5×107); p<0.001, Wilcoxon signed rank test) and when patients were stable (median difference in TVC 3.8×107 cfu/g (95% CI 1.1×107 to 7.8×107); p=0.01) but less so at completion of antibiotic treatment (median difference in TVC 1.3×107 cfu/g (95% CI −0.01×107 to 6.2×107); p=0.07; figure 2). There was also a decrease in TVC with antibiotic treatment for aerobic bacteria (median decrease in TVC 2.3×107 cfu/g (95% CI 6.5×107 to 12.8×107); p=0.005, corresponding to a median percentage reduction of 85%) and some evidence of a similar reduction for anaerobic bacteria (median decrease in TVC 3×106 cfu/g (95% CI 0.3×106, 7×106); p=0.046, corresponding to a median percentage reduction of 51%; figure 2). Comparison of numbers (Friedman test) for the 13 patients in which three samples (stable, initiation and completion of antibiotic treatment) were collected revealed evidence of a difference in the aerobic (p=0.016) but not the anaerobic bacteria (p=0.15) between the three groups. To generate a more taxa-specific view of bacterial species in which abundance changed with antibiotic treatment, viable counts for individual species were compared at the different time points. P aeruginosa TVC decreased from 6.7×107 cfu/g before antibiotic treatment to 2.5×107 cfu/g after antibiotic treatment for the 16 matched sample pairs in which P aeruginosa had been detected on admission for treatment (median decrease in TVC 2.0×107 cfu/g (95% CI 0.5×107 to 6.8×107); p=0.01, corresponding to a median percentage reduction of 89%; figure 3). No differences in TVC were apparent for any other species.

Total viable counts/g sputum of aerobic and anaerobic bacteria cultured from sputum samples collected from adult patients with cystic fibrosis at initiation (Exacerbation) and completion of IV antibiotic treatment (End of Treatment) for an exacerbation and when stable (Stable). CFU, colony-forming unit.
{kind=link}
{kind=link}
{kind=link}
Comparison of total viable counts/g sputum for Pseudomonas aeruginosa. CFU, colony-forming unit.
In addition to quantifying bacterial load with TVC, we also used qPCR, a low-cost highly sensitive and reproducible molecular technique targeting the conserved 16S rRNA gene.16 While this method does not distinguish between bacterial species, there was evidence of a decrease in total bacterial concentration with antibiotic treatment (see figure 3 in online supplement) with the log10 qPCR value on average 0.53 (95% CI 0.13 to 0.94) higher at initiation compared with end of treatment (p=0.01, paired sample t test).
Discussion
In this study we used both aerobic/anaerobic culture and molecular (T-RFLP) techniques to investigate microbial community diversity and abundance in sputum from patients with CF at the initiation and completion of antibiotic treatment for an acute exacerbation and when clinically stable. Multiple anaerobic species were detected by both methods, further confirming and expanding upon the findings of previous studies4–8 10 11 18–20 which have reported that a highly diverse polymicrobial community exists within the CF lung. Furthermore, both methods demonstrate that the composition of the bacterial community remained relatively constant in the majority of patients before and after antibiotic treatment and when clinically stable, and that there was similarity in the composition between exacerbation and stable states. In a previous study of patients with stable CF we also demonstrated persistence of anaerobic species in multiple samples from the same patients.8 Unfortunately, owing to the small sample size, we were unable to determine if there was a correlation between the presence or absence of particular species and it is important that future studies with larger patient numbers address this issue. These results provide further evidence that patients with CF with established lung disease are chronically colonised by a range of bacterial species, including anaerobes, which persist despite antibiotic treatment.
Although the composition of the bacterial community remained relatively constant, our quantitative culture results suggest that changes in bacterial abundance can be detected following antibiotic treatment, with this effect being more pronounced for aerobes than anaerobes. This finding was confirmed by qPCR which showed a decrease in bacterial 16S rRNA gene copies/g sputum following antibiotic treatment. Furthermore, our results also suggest that P aeruginosa was more susceptible to current antibiotic therapy than other members of the microbial community as it was only the genus in which there was a significant decrease in abundance with antibiotic treatment. This may be because antibiotic treatment in the majority of patients was targeted against P aeruginosa and that the antibiotics primarily used (tobramycin and ceftazidime) have poor in vitro activity against anaerobic bacteria.10 21 Our findings are consistent with previous reports which showed that a decrease in bacterial load in sputum following antibiotic treatment is associated with clinical improvement.22–25 Exacerbations were treated with a wide range of antibiotic regimens, so we were uable to determine if there was a relationship between the use of specific antibiotics such as meropenem—which has excellent in vitro activity against anaerobes cultured from CF sputum8 10—and the change in anaerobic bacterial load following treatment.
There was relatively good agreement between T-RFLP and culture detection methods for the identification of the more abundant aerobic pathogens, P aeruginosa and B cepacia complex. This finding confirms the results of previous studies which also reported excellent congruence between aerobic culture and bacterial rRNA gene detection methods.7 11 However, in contrast to the findings for aerobic bacteria, there was poor agreement between T-RFLP and TVC culture data for anaerobes which were present in greater diversity and lower abundance. These findings suggest that these very different methods are similarly effective at detecting abundant organisms but both are required to capture the full spectrum of less abundant and potentially difficult to culture anaerobes. As our identification prediction involves a number of bacterial taxa that are poorly characterised and under-represented in 16S rRNA gene sequence databases, we restricted our identification to the genus level. Future identification of anaerobic bacteria to species level may be important when assessing the potential pathogenicity of any anaerobes present. This further emphasises both the importance of culture in the detection of anaerobic bacteria and that the two methods are complementary in the data they provide. T-RFLP assignments that had no corresponding culture assignment may have been due to the presence in the samples of bacteria which were not cultured by the methods employed. Furthermore, bacterial genera predicted by T-RFLP were limited to those organisms for which reference patterns were available. Inclusion of additional reference spectra would therefore increase the range of bacterial genera identified by T-RFLP. However, more expensive methods such as deep sequencing26 and microarrays (eg, 16S rRNA PhyloChip27) may allow more comprehensive characterisation of CF lung microbial communities.
In the present study, streptococci from the Streptococcus milleri group (SMG) and the S viridans group were identified in 19 samples by culture, with streptococci detected by T-RFLP in 47/64 samples. This was not unexpected given that our study focused on anaerobic bacteria and that we did not use selective media or incubation conditions to optimise the culture detection of streptococci. Previous studies have similarly shown that streptococci from the SMG may not be detected by routine CF microbiology protocols.28 A case report study29 and a more recent longitudinal study28 have both shown a beneficial clinical response to treatment of the predominant SMG organism during exacerbations, suggesting that streptococci may also contribute to a polymicrobial community of bacteria that are CF respiratory pathogens. Culture protocols in subsequent studies should therefore be amended to optimise the detection and quantitation of these organisms.
The potential pathogenic role of bacteria such as anaerobes and streptococci in CF pulmonary infection remains unclear. However, some of these anaerobic bacteria have been shown to be pathogenic in other lung diseases30–32 and preliminary studies by our group have shown that they are also present in the lungs of patients with non-CF bronchiectasis.33 Ultimately, the clinical relevance of anaerobic bacteria in the CF lung can only be addressed by clinical trials in which patients receive antibiotics targeted against aerobic bacteria only versus antibiotics targeted against both aerobes and anaerobes. Subsequent determination of the reduction in bacterial load combined with analysis of pulmonary function and markers of inflammation could establish whether anti-anaerobe treatment resulted in improved clinical outcome for patients. However, some antibiotics with putative antimicrobial activity against anaerobic bacteria are not effective in vitro against anaerobes isolated from CF sputum.8 10 Antibiotic regimens used in such trials would therefore need to take account of the distinctive sensitivity patterns of anaerobes present in the CF lung.
In conclusion, our results show that we can detect changes in bacterial abundance within the microbial community following antibiotic treatment but that these changes are only large enough to be detected individually for P aeruginosa. They also show that aerobic/anaerobic culture and molecular detection methods are both required for comprehensive characterisation of the microbial community in the CF lung. Molecular methods are sensitive and accurate and provide a more complete view of the bacterial communities present and may also be useful to direct improved species-specific culture methods. However, they do not remove the need for culture detection which is more quantitative and provides the opportunity to perform antibiotic sensitivity testing which can subsequently be used to target antibiotic treatment. Further larger studies of polymicrobial CF lung infection, including alteration of current antibiotic treatment in CF to treat these newly identified bacteria, are urgently required to elucidate more fully their clinical significance and improve treatment strategies and outcome for patients with CF.
Acknowledgments
The authors acknowledge the technical assistance of Mr Gerry McGrillen (School of Pharmacy, Queen's University Belfast). We also wish to acknowledge Professor John Moore (Belfast Health and Social Care Trust) for helpful discussions in respect of this study.
References
Supplementary materials
Web Only Data thx.2010.137281
Files in this Data Supplement:
Web Only Data thx.2010.137281
Files in this Data Supplement:
Web Only Data thx.2010.137281
Files in this Data Supplement:
Web Only Data thx.2010.137281
Files in this Data Supplement:
Footnotes
Linked article 157875.
MMT, JSE and MCW contributed equally to this study.
Funding Supported by a UK Cystic Fibrosis Trust grant (PJ533) and a grant from the US National Institutes of Health (HL084934). MMT was supported by a Health and Social Care Research and Development, Public Health Agency, Northern Ireland-funded UK National Institute for Health Research Career Scientist Award.
Competing interests None.
Ethics approval This study was conducted with the approval of the Office for Research Ethics Northern Ireland.
Provenance and peer review Not commissioned; externally peer reviewed.