Article Text

Statistics from Altmetric.com
- Aneurysm of pulmonary artery
- haemoptysis
- multidetector computed tomographic angiography (MDCTA)
- pulmonary tuberculosis
- Rasmussen's aneurysm
- imaging/CT MRI etc
- rare lung diseases
- tuberculosis
A 47-year-old woman with a past history of pulmonary tuberculosis presented to our institution with out-of-hospital cardiac arrest because of massive haemoptysis after severe coughing. On arrival, immediate cardiopulmonary resuscitation with chest compression, endotracheal intubation and intravenous epinephrine 1 mg with an interval of 3 min for asystole was performed. Twelve minutes later she was defibrillated twice with 150 joules and intravenous epinephrine of 1 mg with an interval of 3 min for ventricular fibrillation was given. Return of spontaneous circulation with a blood pressure of 181/98 mm Hg and a pulse rate of 80 beats/min was achieved 4 min later. Fluid replacement, blood transfusion, tranexamic acid and pitressin were given for persistent gushing of fresh blood from the endotracheal tube. It was suspected that the bleeding originated from the pulmonary or bronchial vessels. Laboratory evaluation revealed a white blood cell count of 13 100/mm3 with 43.2% segmented neutrophils and 50.4% lymphocytes, haemoglobin 8.5 g/dl and platelet counts of 134×103/mm3. Thoracic contrast-enhanced 64-slice multidetector computed tomographic angiography (MDCTA) demonstrated a vascular lesion 29 mm in diameter originating from a branch of the pulmonary artery (PA) with contrast media extravasations indicating a ruptured Rasmussen's aneurysm (figures 1 and 2). Pulmonary angiography with embolisation was attempted and a thoracic surgeon was consulted. However, cardiopulmonary resuscitation, defibrillation, fluid replacement, epinephrine and pitressin were prescribed for pulseless electrical activity and recurrent ventricular fibrillation. Four hours later the patient died after return of spontaneous circulation. Sputum culture 1 month later confirmed tuberculosis.

(A) Axial MDCTA image in lung window showing cavitary infection (black arrowhead) over left upper lobe. The culture result 1 month later confirmed tuberculosis infection. Severe pulmonary haemorrhage and haemoptysis are evident from the left upper lobe consolidation, blood clot in the bilateral main bronchi (arrows) and scattered faint airspace patches (white arrowhead) over the right lung. AAO, ascending aorta; DAO, descending aorta; MPA, main pulmonary artery. (B) Oblique sagittal MDCTA image showing a ruptured vascular lesion with contrast media extravasations (arrow) in the focal consolidation over the left upper lobe with cavitations and diffuse centrolobular airspace densities indicating pulmonary tuberculosis complicating a ruptured Rasmussen's aneurysm.
{kind=link}
{kind=link}
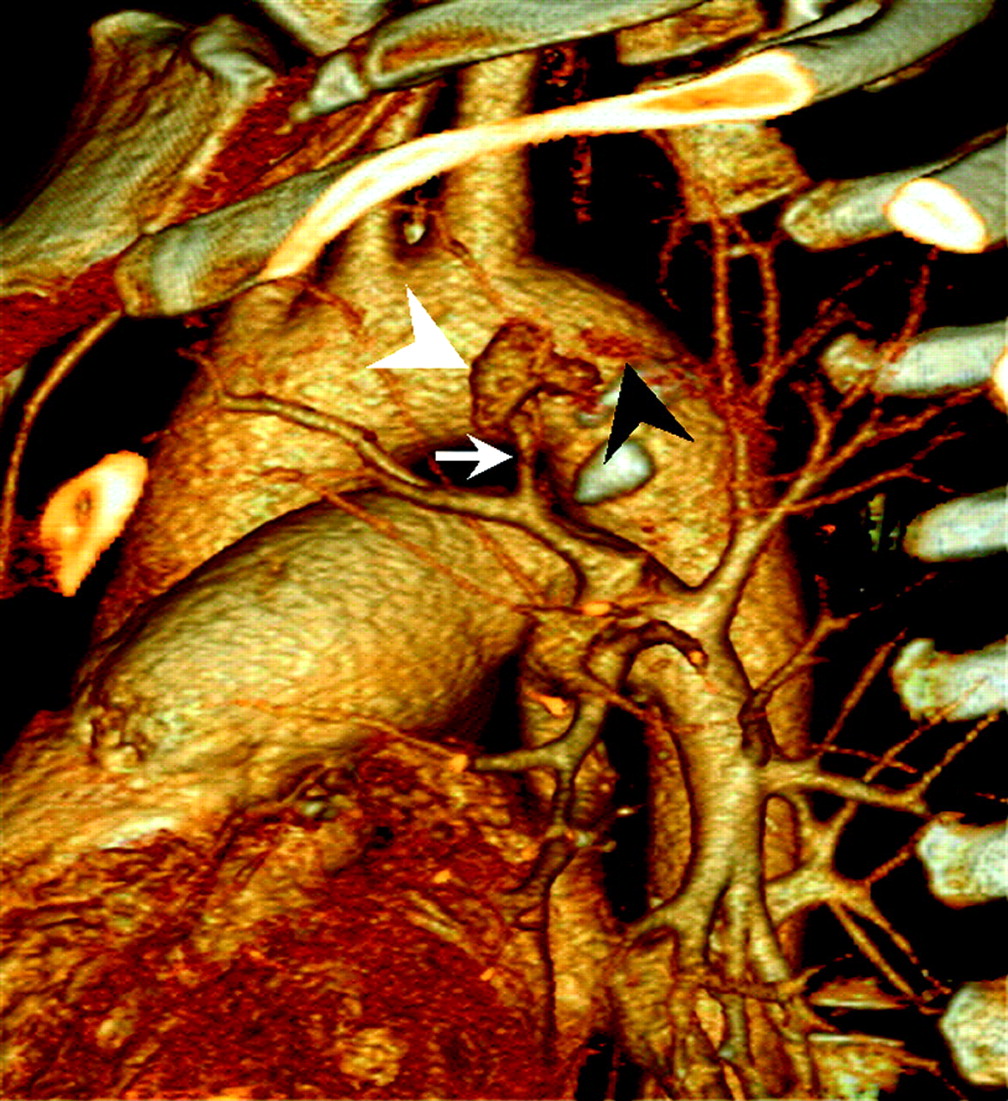
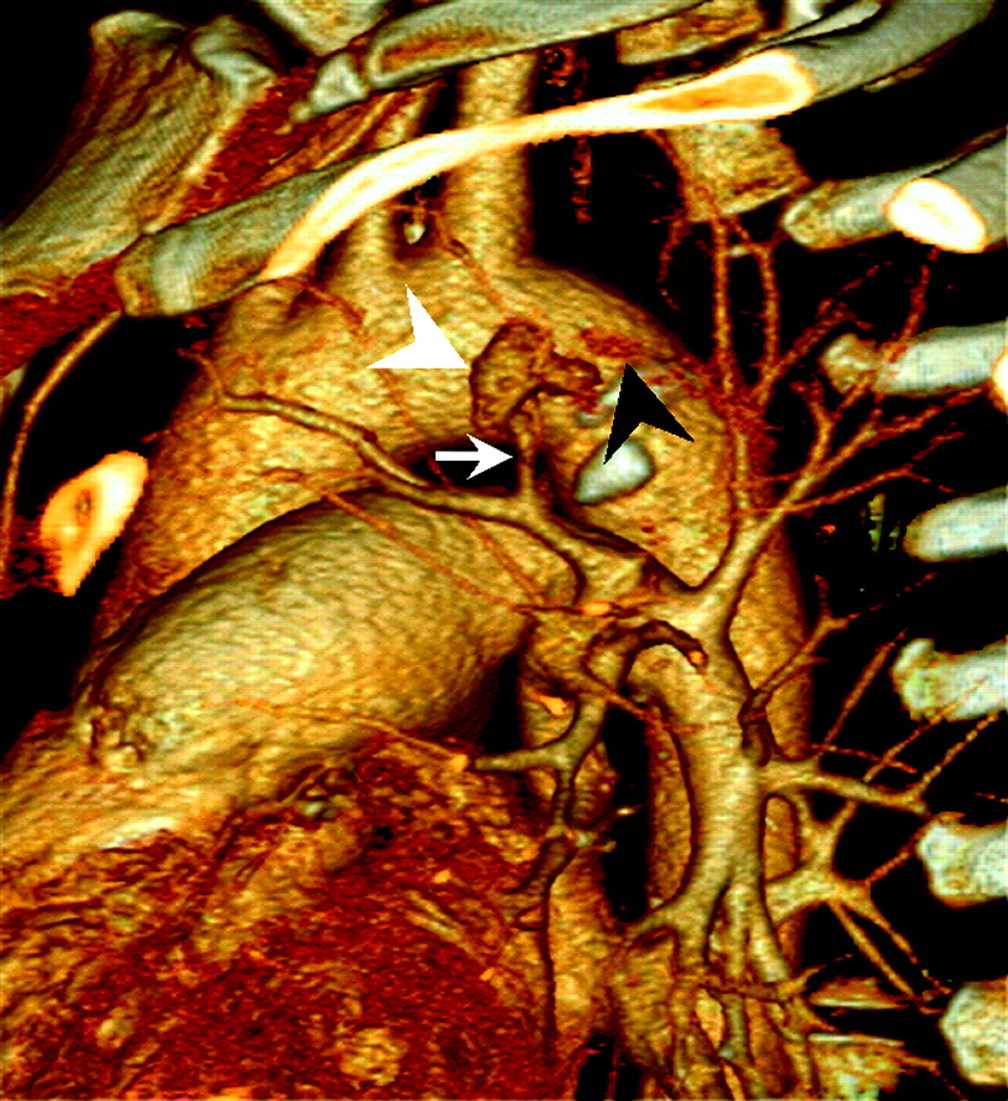
Oblique sagittal slab volume-rendering image clearly showing a Rasmussen's aneurysm (white arrowhead) originating from a small pulmonary artery branch (arrow) over the left upper lobe. Adjacent contrast medium extravasations (black arrowhead) indicate rupture of the aneurysm. With a 5 s MDCTA scan, tuberculosis infection, rupture of Rasmussen's aneurysm and severe pulmonary haemorrhage are all depicted.
Massive haemoptysis has a mortality rate of >50%. The prevalence of haemoptysis originating from the PA is <10%. Rasmussen's aneurysm has a prevalence of 5%.1 MDCTA can demonstrate the PA and pseudoaneurysm of PA in the adjacent cavity.1 2 The mortality rate for emergency surgery in unstable haemodynamic patients is high, so radiological endovascular embolisation of endovascular embolisation with coils is recommended first in these patients.1 2
Learning points
Massive haemoptysis is a life-threatening condition associated with a mortality rate of >50% and ruptured Rasmussen's aneurysm should be considered in patients with massive haemoptysis, especially if there is a history of pulmonary tuberculosis.1
Rasmussen's aneurysm is a rare phenomenon caused by weakening of the pulmonary artery wall from adjacent cavitary tuberculosis, with a prevalence of 5%.1
Mandatory radiological studies should include thoracic MDCTA and digital substrate angiography to differentiate between bleeding from pulmonary or bronchial origins.1 2
Surgical or angiographic interventions with endovascular embolisation is recommended in this life-threatening condition.1 2
Supplementary materials
Footnotes
Competing interests None.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.