Article Text

Abstract
Background The COPD (chronic obstructive pulmonary disease) assessment test (CAT) is a recently introduced, simple to use patient-completed quality of life instrument that contains eight questions covering the impact of symptoms in COPD. It is not known how the CAT score performs in the context of clinical pulmonary rehabilitation (PR) programmes or what the minimum clinically important difference is.
Methods The introduction of the CAT score as an outcome measure was prospectively studied by PR programmes across London. It was used alongside other measures including the St George's Respiratory Questionnaire, the Chronic Respiratory Disease Questionnaire, the Clinical COPD Questionnaire, the Hospital Anxiety and Depression score, the Medical Research Council (MRC) dyspnoea score and a range of different walking tests. Patients completed a 5-point anchor question used to assess overall response to PR from ‘I feel much better’ to ‘I feel much worse’.
Results Data were available for 261 patients with COPD participating in seven programmes: mean (SD) age 69.0 (9.0) years, forced expiratory volume in 1 s (FEV1) 51.1 (18.7) % predicted, MRC score 3.2 (1.0). Mean change in CAT score after PR was 2.9 (5.6) points, improving by 3.8 (6.1) points in those scoring ‘much better’ (n=162), and by 1.3(4.5) in those who felt ‘a little better’ (n=88) (p=0.002). Only eight individuals reported no difference after PR and three reported feeling ‘a little worse’, so comparison with these smaller groups was not possible.
Conclusion The CAT score is simple to implement as an outcome measure, it improves in response to PR and can distinguish categories of response.
- Quality of life
- minimal clinically important difference
- COPD
- pulmonary rehabilitation
Statistics from Altmetric.com
Key messages
What is the key question?
Does the COPD assessment test (CAT), a new health status measure for the condition, show a response to pulmonary rehabilitation?
What is the bottom line?
A fall (improvement) in the score occurs following pulmonary rehabilitation which was larger in those who felt ‘much better’ rather than in those who felt only ‘a little better’.
Why read on?
The article compares response to the CAT, which is simple to implement and score, with response to other outcome measures currently in use for pulmonary rehabilitation.
Introduction
In patients with chronic obstructive pulmonary disease (COPD), pulmonary rehabilitation (PR) can reduce symptoms, improve activity, restore independent function and reduce healthcare utilisation.1–3 Validated tools including the St George's Respiratory Questionnaire (SGRQ),4 the Chronic Respiratory Questionnaire (CRQ)5 and the Clinical COPD Questionnaire (CCQ)6 have been used to assess the impact of PR on health-related quality of life. However, current health-related quality of life questionnaires are complex, time-consuming to complete and may require specialist software or licences to use, which limits their applicability in routine practice.
The COPD assessment test (CAT)7 was developed as a short, simple instrument for quantifying the symptom burden of COPD in routine practice to aid health status assessment and facilitate communication between patient and healthcare professionals. It consists of eight items, each presented as a semantic 6-point differential scale, providing a score out of 40 indicating the impact of the disease. It is completed by the patient and the result is immediately available without the need for any calculation, apart from summing the scores on individual items. Scores of 0–10, 11–20, 21–30 and 31–40 represent mild, moderate, severe or very severe clinical impact.8
The CAT was derived from 21 candidate items identified through qualitative research with patients with COPD from three prospective international studies (Europe and the USA, n=1503). Psychometric and Rasch analyses identified eight items fitting a unidimensional model to form the CAT, with high internal consistency (Cronbach α was 0.88). Intraclass correlation coefficient was 0.8 for test–re-test in stable patients and CAT score correlated well with the COPD-specific version of the SGRQ (r=0.80). There are data to show that it distinguishes stable from exacerbating patients,7 but as yet no data on how it responds to PR or any other intervention.
PR programmes routinely use various methods to collect data about patients' baseline characteristics including health status and to assess their response to rehabilitation. The adoption of the CAT as an outcome measure by a network of pulmonary rehabilitation centres around London provided the opportunity to evaluate its responsiveness relative to other outcome measures used in rehabilitation studies and explore the use of an anchor questionnaire to address the minimum clinically important difference for the CAT.
Methods
We performed a multicentre, prospective study of response to PR in patients with a clinical diagnosis of COPD. The study was approved by the Riverside Research Ethics Committee and recorded on an international trials register: ISRCTN51185878. Participating sites were located throughout London in both primary and secondary care settings. Patients were referred into programmes by a medical practitioner. All programmes included a mixture of aerobic and strength training and a mixture of supervised sessions and unsupervised home exercise, usually two supervised and one or more home sessions per week, with a duration of 8 weeks. Initial exercise prescription was based on the outcome of a baseline walking test, and workloads were increased through the programme as tolerated. Programmes were multidisciplinary, with an educational component covering issues including exercise, medication use, diet and coping strategies. Data were collected between January and August 2010 and recorded at enrolment and completion of the programmes.
The primary objective of the study was to establish the change in CAT score occurring in response to PR, relating this to an anchor question to explore CAT scores that may be indicative of the minimum clinically important difference (MCID). Response to the anchor question used to assess overall response to rehabilitation, ‘How do you feel your overall condition has changed after rehabilitation?’ was scored; 1, ‘I feel much better’; 2, ‘I feel a little better’; 3, ‘I feel no different’; 4, ‘I feel a little worse’; 5, ‘I feel much worse’. The anchor question was asked at the end of the final assessment session.
Secondary objectives were to compare baseline CAT and change in CAT score with other health status and functional parameters measured in rehabilitation and to measure effect size of the tests being evaluated. The programmes in this study used a range of different baseline measures and outcomes, and the use of some outcomes varied between sites within programmes, so that the sample size for comparing the CAT with other measures was variable.
Description of other comparator outcome measures used
The CCQ6 is a self-administered questionnaire developed to measure clinical control in patients with COPD. It includes 10 items; each response is graded 1–6, with a higher score indicating worse health status. Cronbach α is high (0.91). Significant correlations have been demonstrated between the CCQ total score and domains of the SGRQ (r=0.67–0.72). In patients with COPD, the correlation between the CCQ and forced expiratory volume in 1 s (FEV1) % predicted was r= −0.49. Test–re-test reliability is high (intraclass coefficient=0.94). The minimum clinically important difference of the CCQ is 0.4.9
The SGRQ4 consists of 50 items with 76 weighted responses. It was developed and validated in both asthma and COPD. It is completed by the patient by hand, but requires a computer to score it. Scores are calculated for three domains: symptoms, activity and impacts (psychosocial), as well as a total score. Psychometric testing has demonstrated its repeatability, reliability and validity. Scores range from 0 to 100, with a higher score indicating worse health status. A minimum change in score of four units was established as clinically relevant after patient and clinician testing. The SGRQ correlates significantly with other measures of disease activity such as cough, dyspnoea, 6 min walk test (6MWT) and FEV1, as well as other measures of general health such as the SIP (sickness impact profile) and SF36 (short form 36).
The CRQ5 is a self-reported questionnaire developed to determine the effect of treatment on quality of life in clinical trials. It consists of four dimensions: dyspnoea, fatigue, emotional function and the patient's feeling of control over the disease (mastery). Reproducibility, tested by repeated administration to patients in a stable condition, has been excellent: the coefficient of variation was <12% for all four dimensions. An MCID has been determined as 0.5 for each of the mean domain scores of the CRQ.10
The incremental shuttle walking test ISWT (ISWT) uses a 10 m course and the walking speed is externally paced by signals from an audio cassette or CD. The patient is required to walk between two cones in time to a set of auditory beeps.11 The patient walks for as long as they can until they are either too breathless or can no longer keep up with the beeps, at which time the test ends. The number of shuttles (laps between the cones) is recorded. The results of the ISWT can be used to prescribe the intensity of walking exercise. Following PR in patients with COPD, an improvement of 47.5 m in ISWT corresponded to a patient perception that their exercise performance was ‘slightly better’, and an improvement of 78.7 m corresponded with ‘better’.12
The endurance shuttle walk test (ESWT)13 is a standardised field test for the assessment of endurance capacity in patients with chronic lung disease. The test was developed as an adjunct to the ISWT so that together they form a practical method of assessing both functional and endurance exercise capacity using the same 10 m shuttle course.
The 6MWT is a self paced test that measures the distance that a patient can quickly walk in a period of 6 min (the 6MWD).14 Verbal instructions are standardised. Optimal reference equations from healthy population-based samples using standardised 6MWT methods have recently become available, and a walking distance in excess of 500 m is typical for patients of an age comparable with those entering PR.15
Statistics and data analysis
The data were anonymised at each site and collated centrally for analysis using SPSS v18. Paired t tests were used for comparison of CAT score before and after rehabilitation sessions. Univariate analysis of variance was used for each anchor question response. Correlations between change in CAT and other measures of health status and disease severity were calculated using Pearson correlations and linear regression tools; significantly skewed data were log transformed before analysis. Effect size was calculated as the mean difference in values before and after PR divided by the mean SD (ie, mean SD at baseline and follow-up). It therefore expresses the change in response to treatment against the variability of the parameter in the population being studied. Data are presented as mean±SD unless otherwise specified, and a p value of <0.05 is taken as significant.
Results
Data on CAT score before and after pulmonary rehabilitation were available for 297 individuals, age 69.2±9.3 years, 62.7% male, FEV1 50.9±18.9 % predicted, MRC dyspnoea score 3.4±1.0, median body mass index (BMI) 27.7±6.5. In response to the anchor question, 162 reported that they were much better after PR, 88 a little better, 8 no different and 3 a little worse. In 36 cases the anchor question was not completed. The group in whom the anchor question was not documented did not differ significantly from those in whom it had been recorded. Although not therefore available for the primary outcome, data from these 36 cases were retained for other analyses. Location, recruitment figures and outcome measures used at different sites are given in table 1.
Participating centres and outcome measures employed
Baseline CAT score correlated in univariate analysis with other health status measures, MRC score, ISWT distance, age and airflow obstruction, as expected, with a higher CAT score associated with worse breathlessness, anxiety, depression and functional exercise capacity (table 2). The CAT score was lower in men, 19.7±7.2 versus 21.5±7.5 (p=0.03). In a stepwise regression analysis including age, MRC dyspnoea score, BMI, gender and FEV1 % predicted (n=178 with these data available), only age and MRC dyspnoea score were retained, giving the equation; CAT score=18.8+3.9(MRC score)–0.16(age) (r2=0.29).
Univariate correlates of baseline CAT score
The response of the various outcome measures to rehabilitation are given in table 3 together with estimation of the effect size. The CAT improved significantly following rehabilitation, −2.9±5.6 (p<0.001), as did all other measures of health status and functional capacity. The effect size of rehabilitation on CAT score was moderate (d=0.4); other health status measure effect sizes were variable (CCQ 0.6, CRQ 0.8 and SGRQ 0.2), although the numbers completing each measure were variable—for example, the SGRQ was used in only 39 participants, which means that direct comparisons require caution.
Response to pulmonary rehabilitation (PR)
Change in CAT score in response to rehabilitation was independently associated with baseline CAT score, falling most in those with the highest baseline symptom burden (r=−0.34 p<0.0001). The score also improved more in women: ΔCAT −3.8±6.1 versus −2.2±5.3 (p=0.019), but was not associated with baseline dyspnoea, anxiety and depression, walking distance or airflow obstruction.
Change in CAT score following PR correlated significantly with changes in other measures of response to PR (table 4). Figure 1 shows the correlation between the change in the most frequently recorded measure of health status (the CRQ total score, n=195) and ΔCAT score following PR.
Univariate correlates of change in CAT score
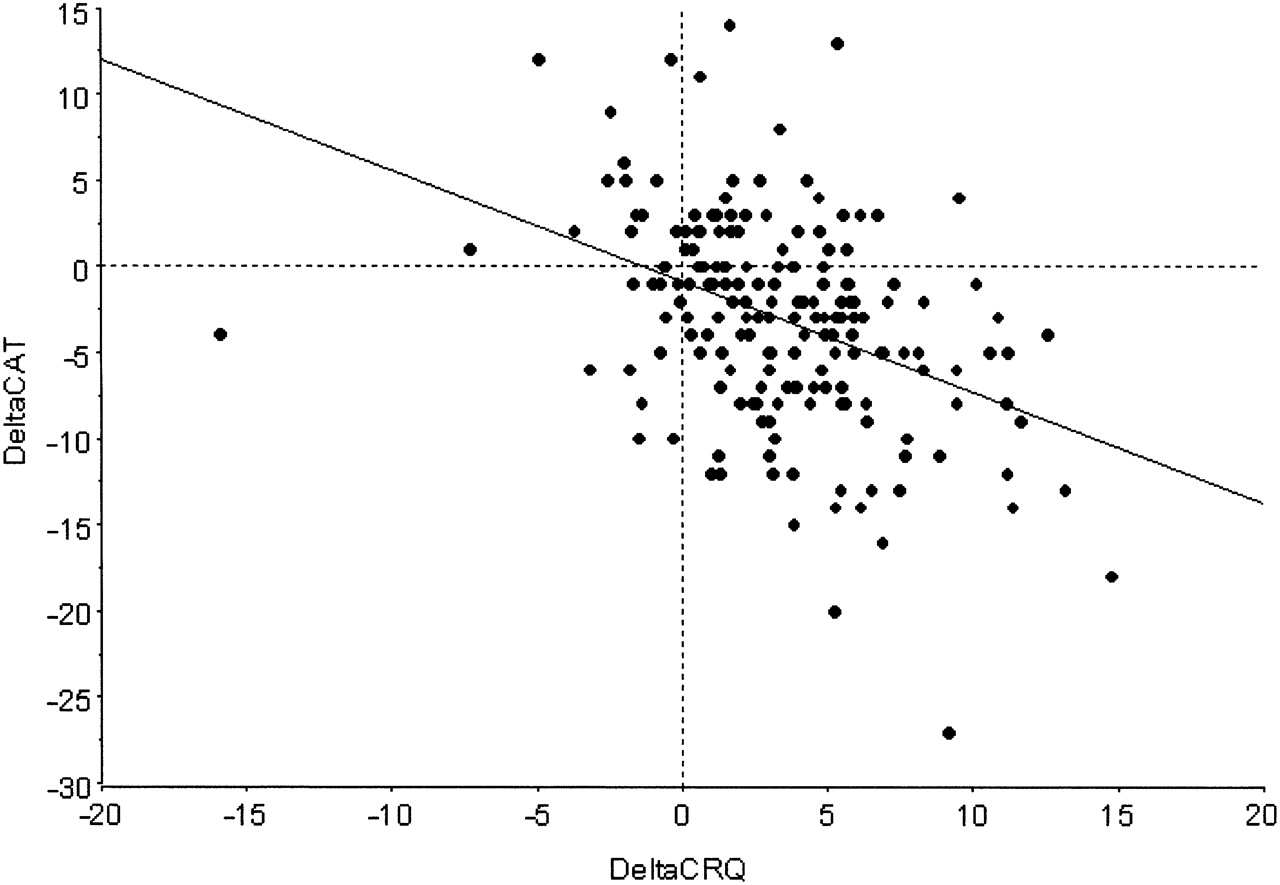
Change in COPD (chronic obstructive pulmonary disease) assessment test (CAT) in response to pulmonary rehabilitation correlated with change in Chronic Respiratory Questionnaire (CRQ) total score (r=−0.41; p<0.001).
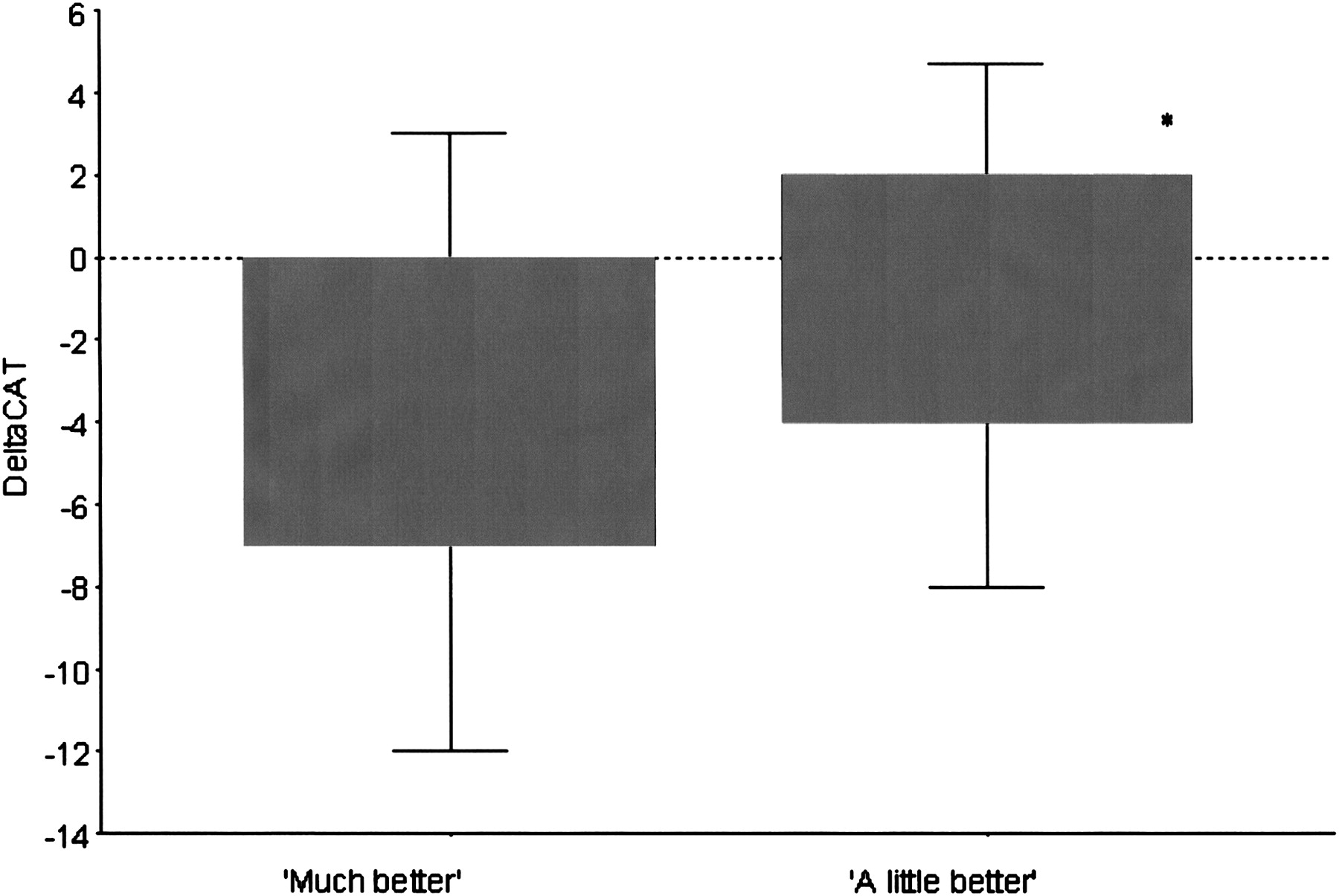
The data in table 5 show the change in CAT and other outcome measures following PR according to the different anchor response categories. Change in CAT score was sensitive to different levels of response to the anchor question (−3.8±6.1 ‘much better’; −1.3±4.5 ‘a little better’, p=0.002) (figure 2). Only small numbers were available for the response categories ‘no different’, n=8 ΔCAT −2.3±3.3; and ‘a little worse’, n=3 ΔCAT +2±0.
Change in outcome measure by anchor question response

{kind=link}
{kind=link}
Change in COPD (chronic obstructive pulmonary disease) assessment test (CAT) score after pulmonary rehabilitation corresponding to different responses to the anchor question ‘How do you feel your overall condition has changed after rehabilitation?’: ‘much better’ n=162, ΔCAT −3.8±6.1; ‘a little better’ n=88, ΔCAT −1.3±4.5 (p<0.002). As only small numbers were available for these categories, data for ‘no different’ n=8 ΔCAT −2.3±3.3; and ‘a little worse’ n=3 ΔCAT +2±0 are not shown.
Table 5 shows that in addition to change in CAT score, change in CRQ and the Hospital Anxiety and Depression (HAD) scores also differed significantly across anchor responses.
Discussion
The main findings of the present study are that the CAT score is responsive to PR and can discriminate between different levels of subjective response when compared with an anchor question, with a fall of 1.3 points corresponding to ‘a little better’ and 3.8 points to ‘much better’. It correlated with improvements in other outcome measures, and the estimated effect size of PR on change in CAT was moderate.
Methodological issues
A strength of this study is that it included a relatively large sample of unselected patients taking part in clinical PR programmes with data collected prospectively across multiple sites. As such, it is likely to be generalisable to routine clinical practice. The centres participating added the CAT score alongside the data they were already collecting routinely, which meant that not all patients had all outcomes measured. Caution is therefore needed in comparing the different measures, as sample sizes available for the comparisons vary. In particular, the sample size for the SGRQ is small.
The MCID for the CAT has not yet been established. Based on a mapping exercise with the published data comparing the CAT and SGRQ,7 the 4-unit MCID for the SGRQ corresponds to a value of 1.6 units for the CAT MCID. An objective of this study was to provide further data that might contribute to the CAT MCID estimation process, but the effectiveness of PR meant that the full range of the anchor question responses 1–5 was not used. This type of one-direction change limits the reliability of MCID estimates; however, the change of 1.3 units observed in the 53 patients who reported that they were ‘a little better’ is of a similar magnitude to the change in CAT score that corresponds to the SGRQ MCID. An alternative approach is to use the MCID of another validated and repeatable clinical measure such as the CRQ as an anchor for those that respond to PR. This technique has been used previously when estimating MCID for exercise tests in COPD.16 However the use of linear regression in this way assumes no measurement error17 and its reliability is dependent upon the strength of correlation between the two measurements, which in the case of the CRQ was only 0.4 (figure 1).
Significance of the findings
The data suggest that the CAT score can be used as an outcome measure in patients with COPD taking part in PR. Since the tool is quick to complete and score and can therefore be integrated into routine clinical practice, it offers the possibility of a closer integration between PR and other aspects of care. The CAT can be completed by patients online, which may be of use in the home management and maintenance of rehabilitation. We acknowledge that certain tools used for baseline assessment may provide specific information that will influence clinical practice, for example the HAD score may guide referral for psychological support, and the lung information needs questionnaire (LINQ) might identify individuals who need particular attention to their understanding of their disease.18 19 A significant amount of time and effort is required by both patients and health professionals in the completion and scoring of various outcome measures around PR, which has an opportunity cost for the delivery of the PR intervention itself. Given the resource limitations that exist, the widespread introduction of a simpler tool such as the CAT may have significant cost benefits.
An important observation is that the overall effectiveness of PR in the programmes in this study was similar to that outlined in a recent meta-analysis of clinical trials of PR, where improvements in CRQ (0.77–1.1) and SGRQ (−6.1) exceeded their respective MCIDs.2 This suggests that outcomes achieved in routine clinical practice are comparable with those observed in clinical trials, at least in patients completing the programme. In our study the participants exceeded the MCID for the CRQ, the 6MWT and the ISWT (table 3).10 12 16 In fact the effectiveness of PR meant that the full range of the anchor question responses 1–5 was not used—only 8 (3%) subjects reported no improvement and 3 (1%) that they were a little worse. This may appear to differ from the results of Singh et al who found a wider range of responses when they assessed the MCID for the ISWT, but it should be noted that the anchor question in that study addressed exercise capacity specifically rather than the more general question in the present paper ‘How do you feel your overall condition has changed after rehabilitation?’.12
Conclusion
The CAT score is responsive to PR and able to distinguish different levels of response. Widespread adoption of the CAT as a substitute for more time-consuming questionnaires has the potential to streamline PR provision and improve benchmarking between programmes.
Acknowledgments
The authors would like to acknowledge the following for their assistance in collecting data: Karen Ingram, Ria Fowler and Amy Clark at Harefield Hospital; and Hellene Bellas at King's College Hospital.
References
Footnotes
Funding The National Institute of Health Research (NIHR) Respiratory Biomedical Research Unit Royal Brompton & Harefield NHS Foundation Trust and Imperial College. WD-CM is funded by an NIHR Clinician Scientist award. The views expressed in this publication are those of the authors and not necessarily those of the NHS, the NIHR or the Department of Health. NSH is an HEFCE Clinical Senior Lecturer.
Competing interests None.
Ethics approval This study was conducted with the approval of the Riverside Research Ethics Committee.
Provenance and peer review Not commissioned; externally peer reviewed.