Article Text

Statistics from Altmetric.com
Case presentation
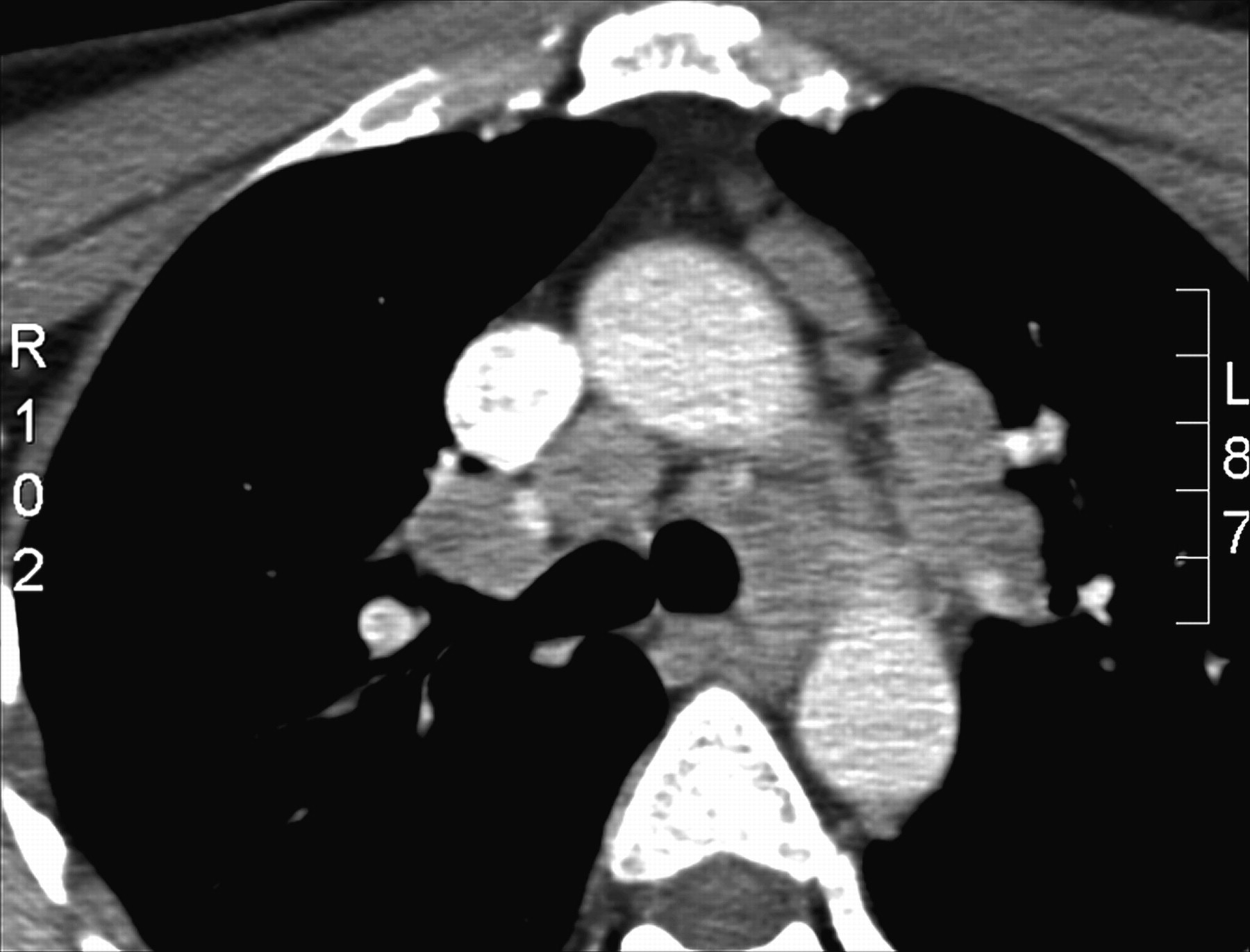
A non-smoking 45-year-old white man presented with a globus sensation worsened by lying down, with no complaints of hoarseness or dysphonia. He denied fever, fatigue, cough, chest pain, sweats, weight loss, reflux, arthralgias, myalgias and rash. He also denied exposure to asbestosis, beryllium, silica, HIV or tuberculosis, but he reported a recent cat bite. Physical examination revealed normal vital signs, no cervical or supraclavicular lympadenopathy and a normal cardiorespiratory system. He was referred to the otolaryngology department. Laryngoscopy revealed right vocal cord paralysis. A CT scan of the neck/chest identified diffuse mediastinal lymphadenopathy without parenchymal changes (figures 1 and 2).

CT scan of high right paratracheal lymph node.

CT scan showing low paratracheal involvement.
A purified protein derivative test was negative. Endobronchial ultrasound (EBUS)-directed transbronchial needle aspirations (TBNA) were performed of the paratracheal and subcarinal lymph nodes (figure 3). Diagnostic bronchoscopy revealed no endobronchial lesions or mucosal abnormalities. Acid-fast bacilli studies were negative and flow cytometry detected no monoclonal lymphocytes. Bacterial and fungal cultures, cryptococcal/histoplasma antigen, HIV and Bartonella serology were negative. ACE was 31 U/l (reference range 9–67 U/l). Pulmonary function testing revealed mild decreased diffusion capacity but was otherwise normal. Empirical steroid therapy failed to provide benefit and mediastinoscopic right paratracheal lymphadenectomy was subsequently conducted (figure 4).

Endobronchial ultrasound-directed transbronchial needle aspiration cytology.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Mediastinoscopic lymphadenectomy histology.
Question
What is the diagnosis?
See page 231 for answer
Answer
From question on page 211
Non-caseating granulomas were identified on cytological and histological examination consistent with a diagnosis of sarcoidosis (figures 3 and 4). Sarcoidosis-associated vocal cord paralysis is uncommon. In general, vocal cord paralysis is usually bilateral or left-sided, probably due to decreased lymphatic drainage. In sarcoidosis, isolated right vocal cord paralysis has never been reported. Granulomatous invasion of the laryngeal nerves (perineuritis) and sarcoidosis-related cranial polyneuritis resulting in bilateral vocal cord paralysis have been reported rarely.1 Reports of unilateral left vocal cord paralysis are more common and are probably caused by compression by the bulky mediastinal disease on the left recurrent nerve at the level of the aorta. With a presumptive diagnosis of sarcoidosis based on the initial EBUS-TBNA cytology, oral steroids were administered for 2 months. The patient experienced no symptomatic improvement.
Studies suggest that the diagnostic accuracy of EBUS-TBNA in sarcoidosis is 85–91%.2 Although the patient's diagnosis was felt to be accurate, there remained concerns of a missed carcinoma. Sarcoid-like reactions can occur in the regional lymph nodes of carcinomas with a frequency of 4.4%.3 We also considered the possible benefit of lymphadenectomy in alleviating the compressive effects of the right paratracheal node, despite the prolonged course of nerve compression. Similarly, left recurrent laryngeal nerve palsy associated with silicosis improved after 15 weeks following mediastinoscopic lymphadenectomy.4 The patient's concern about malignancy and the potential therapeutic benefit of lymphadenectomy prompted mediastinoscopy. Mediastinoscopy (with a reported diagnostic accuracy in stage I or II sarcoidosis of 82–97%) confirmed the patient's diagnosis.5 Six months after complete right paratracheal lymphadenectomy, both the globus sensation and right vocal cord function had improved. Given the patient's improvement with nodal resection, we suspect in this case the vocal cord paralysis was caused by nerve compression, reinforcing the need for decompression even in late stages (figure 1).
Footnotes
Conflict interests None.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Airwaves