Article Text

Abstract
Background Asthma is a growing public health problem in developing countries. However, few studies have studied the role of urbanisation in this phenomenon. It was hypothesised that children living in a peri-urban setting in Peru have higher rates of asthma and allergy than rural counterparts.
Methods 1441 adolescents aged 13–15 years were enrolled from two settings: a peri-urban shanty town in Lima (n=725) and 23 rural villages in Tumbes (n=716). Participants filled in questionnaires on asthma and allergy symptoms, environmental exposures and sociodemographics, and underwent spirometry, and exhaled nitric oxide (eNO) and allergy skin testing. Indoor particulate matter (PM) concentrations were measured in 170 households.
Results Lima adolescents had higher rates of lifetime wheezing (22% vs 10%), current asthma symptoms (12% vs 3%) and physician-diagnosed asthma (13% vs 2%; all p <0.001). Current rhinitis (23% vs 12%), eczema (12% vs 0.4%), atopy (56% vs 38%), personal history of cigarette smoking (7.4% vs 1.3%) and mean indoor PM (31 vs 13 μg/m3) were also higher in Lima (all p <0.001). The peri-urban environment of Lima was associated with a 2.6-fold greater odds (95% CI 1.3 to 5.3) of asthma in multivariable regression. Forced expiratory volumes were higher and FEV1/FVC (forced expiratory volume in 1 s/forced vital capacity) ratios were lower in Lima (all p <0.001). Higher eNO values in Lima (p <0.001) were attributable to higher rates of asthma and atopy.
Conclusions Peri-urban adolescents had more asthma, atopy and airways inflammation and were exposed to more indoor pollution. The findings provide evidence of the risks posed to lung health by peri-urban environments in developing countries.
- Asthma risk
- atopy
- exhaled nitric oxide
- urban–rural
- developing country
- asthma epidemiology
- clinical epidemiology
- exhaled airway markers
Statistics from Altmetric.com
- Asthma risk
- atopy
- exhaled nitric oxide
- urban–rural
- developing country
- asthma epidemiology
- clinical epidemiology
- exhaled airway markers
Key messages
What is the key question?
We wanted to know whether the trend for increased urbanisation in developing countries could account in part for the increasing prevalence and morbidity of asthma.
What is the bottom line?
Our study showed that adolescents living in a peri-urban environment had increased levels of atopy, asthma and airway inflammation compared with their counterparts living in a rural environment.
Why read on?
The peri-urban environment of Lima conveyed a nearly threefold increased risk of current asthma. The higher levels of indoor air pollution may contribute to these findings.
Introduction
Asthma is widely recognised for its high prevalence and public health importance in developed countries.1 It is estimated to affect 300 million individuals worldwide,2 and its burden in disability-adjusted life years lost is comparable with that of diabetes mellitus or cirrhosis.2 Risk factors for asthma include allergic symptoms,3–5 atopy3 and elevated total serum immunoglobulin E (IgE).6 Urbanisation has become recognised as an important contributor to childhood asthma.7–9 Some purport that urbanisation leads to increased asthma due to higher levels of air pollution including particulate matter (PM),10 while others have pointed to changes in diet.11 12 Others hypothesise that exposure to fewer parasitic infections or a greater number of viral infections early in life while the immune system is developing may play a role in asthma risk.9 As many major urban centres in the developing world are undergoing rapid growth accompanied by increases in outdoor air pollution, the incidence and burden of asthma are also likely to increase.
The effect of urbanisation on asthma risk is well known; however, few studies have been conducted in low- and middle-income countries. Moreover, unique exposures in developing countries such as to biomass fuels, peri-urban sprawl and inadequate water and sanitation warrant further consideration. Three African studies point to an urban environment as an important risk factor in developing countries.13–15 Urban asthma prevalence ranged from 4% to 23% in these studies, and the increase in odds from rural to urban environments ranged between 1.5 and 4. These rates of asthma are in agreement with the region's results in the International Study of Asthma and Allergies in Childhood (ISAAC).1 Peru is reported to have one of the highest prevalences of asthma worldwide.1 ISAAC reported that 48% of adolescent children had ever wheezed and 26% had experienced wheezing within the previous year. A study in a Lima shanty town reported that 21% of children ever had asthma-related symptoms, and 23% showed a decrease in forced expiratory volume in 1 s (FEV1) postexercise.16 However, these studies were conducted in urban areas of Lima, where one-third of the population lives. There remains limited information on asthma in other regions of Peru or on risk factors driving this high burden of disease in Lima. We hypothesised that children living in a peri-urban setting would have a higher risk of asthma symptoms, allergy and airways inflammation than their rural counterparts.
Methods
We provide an abbreviated description of our data collection methods. Additional detail is provided in an online supplement.
Study setting
We conducted our study in two coastal regions of Peru. Pampas de San Juan de Miraflores is a peri-urban shanty town in Lima with high population density centred on a heavily trafficked avenue. Tumbes is located in northern Peru near the Ecuador border and has little traffic and migration. We conducted our study in a cluster of 23 rural villages outside Tumbes city.
Study subjects
In Lima, we invited an age- and sex-stratified sample of adolescents 13–15 years of age to participate. In Tumbes, we invited all 13- to 15-year-old adolescents in the above 23 villages. Inclusion and exclusion criteria are detailed in the online supplement.
Study design
We carried out home visits to enrol participants, administer the survey and perform physical testing. During the first visit, we asked about asthma and allergy symptoms using a validated questionnaire,17 asthma medications use, biomass fuel exposures and sociodemographics.
We conducted physical testing during a second visit. After measuring height and weight, we conducted spirometry presalbutamol and postsalbutamol according to standard guidelines.18 We measured exhaled nitric oxide (eNO) levels in parts per billion (ppb) and applied allergy skin tests for cockroach, dust mite mix, cat hair, dog epithelium, mouse epithelium and mixed moulds. We measured approximate PM2.5 concentrations (μg/m3) for 48 h using a portable nephelometer in a random subset of 100 households in Lima and 70 in Tumbes. We obtained outdoor PM data in Lima from DIGESA (http://www.digesa.sld.pe).
This study was approved by the Institutional Review Boards of the Johns Hopkins Bloomberg School of Public Health in Baltimore, USA, and AB PRISMA in Lima, Peru.
Definitions
We defined current asthma symptoms as wheezing or asthma medication use in the past year; atopy as a positive test to one or more skin test allergens; and reversibility as a ≥12% increase in FEV1 from preslabutamol to postsalbutamol.18 We graded asthma severity as per National Asthma Education Prevention Program guidelines.19
Biostatistical methods
We used standard statistical methods for the calculation of ORs and χ2 tests. We used logistic regression analysis to model the effect of multiple variables on the risk of asthma. We conducted analyses in R (http://www.r-project.org) and STATA 10. These methods are discussed in detail in the online supplement.
Results
Baseline characteristics
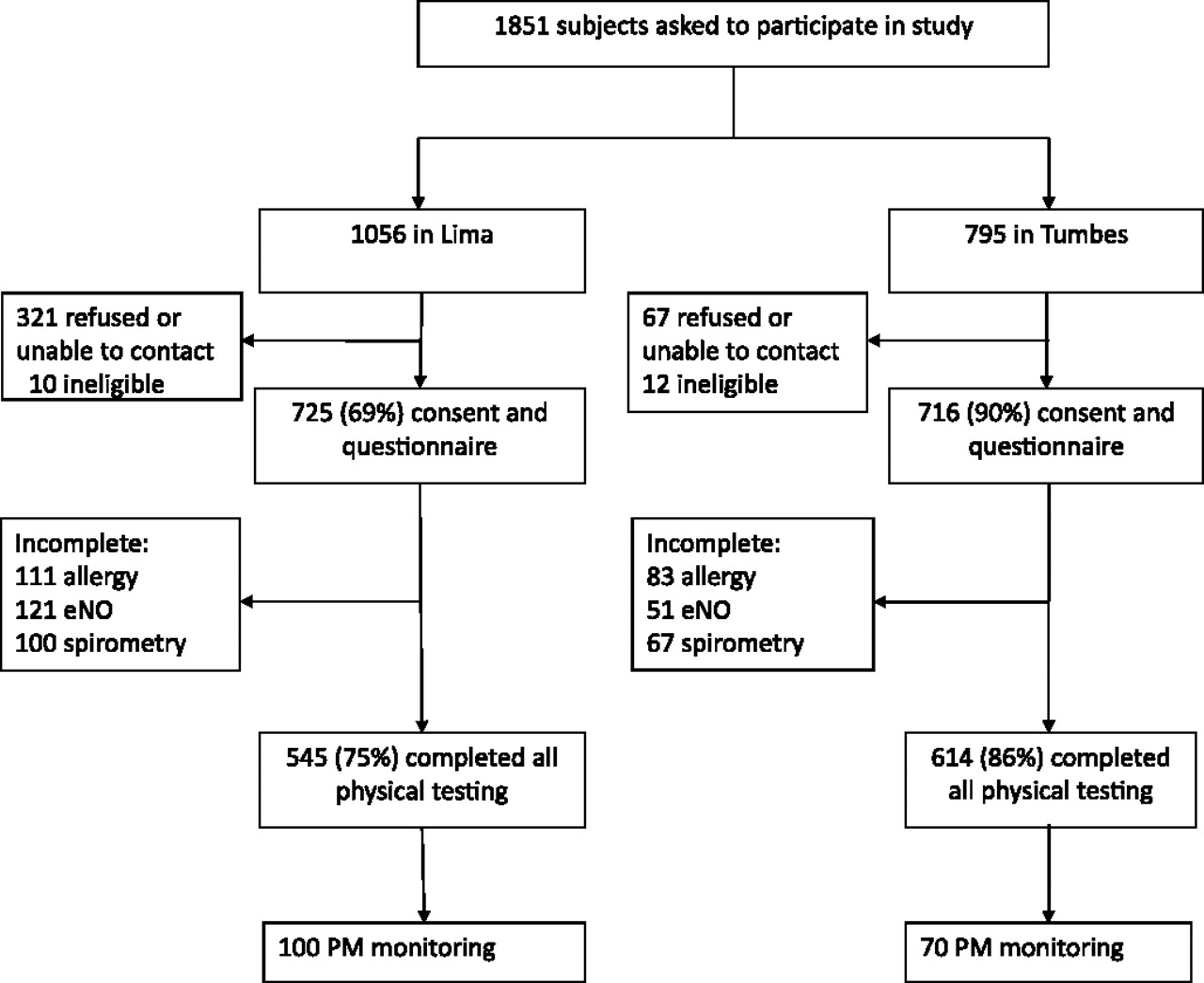
Of 1851 adolescents identified from census data, we enrolled 1441 (78%) during the first visit (figure 1). Seven hundred and twenty-five adolescents in Lima and 716 in Tumbes responded to our survey. Of those enrolled, 545 (75%) in Lima and 614 (86%) in Tumbes completed all aspects of physical testing. A total of 625 (86%) participants in Lima and 649 (91%) in Tumbes completed spirometry. There were no important differences in the distributions of sex or age by site (table 1). Body mass index (BMI) was greater in Lima than in Tumbes. Girls were taller in Tumbes than in Lima. Household incomes were lower in Tumbes than in Lima, as almost threefold more households reported total earnings of <US$175 per month. Fewer households in Tumbes had private sanitation facilities (27% vs 92%, p<0.001).

Flow diagram of recruitment, questionnaires and procedures in Lima and Tumbes, Peru; 2009–2010. eNO, exhaled nitric oxide; PM, particulate matter.
Comparison of personal characteristics, sociodemographics and exposures of adolescents aged 13–15 in urban Lima and rural Tumbes; Peru 2009–2010
Six hundred and ninety-eight (96%) of the Lima adolescent participants had lived in Lima since birth, and >99% had lived in the study community for ≥5 years. A total of 661 (92%) of the Tumbes adolescent participants had lived in Tumbes since birth, and >99% have lived in the study community for ≥5 years. Immigration, however, was common among parents of Lima adolescents. Of the Lima participants, 556 (77%) had at least one parent that had emigrated from the highlands. In contrast, 564 (79%) of the Tumbes participants had both parents who were born in Tumbes. A greater proportion of peri-urban participants reported spending at least 11 h a day at home than did their rural counterparts (70% vs 60%; p<0.001).
Asthma symptoms
All indicators of asthma symptoms were 2–3 times greater in Lima (table 2). The onset of asthma symptoms occurred at an earlier age in Lima. There were no differences in lifetime or current asthma symptoms or age of onset between boys and girls at either site (all p ≥0.12). The most common precipitants of asthma symptoms were upper respiratory infections and exercise. There were no differences in asthma severity between sites (table 3). Approximately 50% of those with asthma were mild intermittent (table 3). A greater proportion of participants in Tumbes with asthma symptoms required emergency visits to hospitals or health centres, and fewer used inhaled corticosteroids or long-acting β-agonists for asthma control compared with those in Lima.
Differences in asthma, allergic symptoms and atopy between Lima and Tumbes; Peru 2009–2010
Asthma severity, burden and relationship with atopy among those with current asthma in Lima and Tumbes; Peru 2009–2010
Adolescents with current asthma symptoms were equally likely to have a lifetime history of rhinitis across sites (table 3). Among those with asthma, the rate of atopy was greater in Lima than in Tumbes (77% vs 56%, respectively); however, this increase only trended towards significance (p=0.09). Adolescents in Lima without current asthma symptoms had a greater prevalence of lifetime rhinitis or atopy than adolescents in Tumbes. Overall, there was a higher prevalence of eczema and a greater number of positive allergen skin tests in Lima than in Tumbes, regardless of asthma symptoms. Rhinitis in the past 12 months, eczema in the past 12 months, atopy and being overweight (BMI >25) were all predictors of current asthma symptoms in Lima in both the unadjusted and multivariable analyses (table 4). In Tumbes, where we had fewer participants with current asthma symptoms (n=22), we identified rhinitis in the past 12 months as the only significant predictor of current asthma symptoms. When we pooled data from both sites, rhinitis in the past 12 months, atopy and being overweight remained important predictors of current asthma symptoms (table 4). The peri-urban environment of Lima was associated with a 2.6-fold greater odds (OR 2.6, 95% CI 1.3 to 5.3) of current asthma after controlling for atopy, allergy symptoms, environmental exposures, household size, sanitation and sociodemographics. We did not find interactions between urbanisation status and: atopy (p=0.38), rhinitis (p=0.14) or being overweight (p=0.67).
Multivariable analysis on the odds of current asthma symptoms stratified by study site; Peru, 2009–2010
Allergic symptoms
Self-reported symptoms of allergic rhinitis were almost twice as prevalent among participants in Lima as among those in Tumbes (table 2). A physician diagnosis of rhinitis was exceptionally rare at either site despite a high proportion of symptom reporting among study participants. Parental rhinitis was fivefold higher in Lima, and in both sites it was a risk factor for rhinitis among offspring (OR 3.0, 95% CI 2.2 to 4.2). Eczema was more prevalent in Lima than in Tumbes (table 2). As with rhinitis, a physician diagnosis of eczema was low despite high symptom rates. Atopy was significantly higher in Lima than in Tumbes (56% vs 38%, p <0.001). The odds of atopy were not increased by having at least six residents in the household, a measure we used as a surrogate for sibling number in either Tumbes (OR 1.3, 95% CI 0.9 to 1.9) or Lima (OR 1.0, 95% CI 0.8 to 1.4).
Spirometry and postbronchodilator reversibility
Six hundred and twenty-five (86%) participants in Lima and 649 (91%) in Tumbes completed spirometry according to standard quality criteria. FEVs were significantly greater in Lima than in Tumbes (table 5). These differences remained even after controlling for age and height within each sex group (all p <0.001). FEV1/forced vital capacity (FVC) values were also lower in Lima than in Tumbes (eFigure 1 (see online)). Reversibility was higher in Lima, but it did not achieve statistical significance (table 5).
Comparison of forced expiratory volumes before and after bronchodilators in Lima and Tumbes; Peru, 2009–2010
Airways inflammation
Mean eNO levels were significantly higher in Lima than in Tumbes (21.9 vs 17.6 ppb; p <0.001). Current asthma symptoms, rhinitis in the past 12 months and atopy increased mean eNO levels at both sites (all p <0.001). eNO measurements conducted in the spring were also higher than measurements conducted in the autumn at both sites (p ≤0.05). Otherwise, there was considerable heterogeneity in the effect of multiple predictors on eNO across sites (eTable 1 (see online)). After adjusting for asthma and atopy in multivariable regression, we found that there was no difference in eNO by site (p=0.47). In multivariable regression, there was a multiplicative interaction between the current asthma symptoms and atopy on eNO levels (table 6; p=0.04 for Lima and p<0.001 for Tumbes).
Exhaled nitric oxide levels stratified by current asthma symptoms and atopy in Lima and Tumbes; Peru, 2009–2010
Household exposures
The primary source of cooking fuel was propane gas at both sites (table 1). A greater proportion of households used wood-burning stoves for cooking on a daily or semi-daily basis in Tumbes than in Lima (42% vs 8.6%; p<0.001). While propane gas stoves were used exclusively indoors, wood-burning stoves were generally used outside of the house (data not shown). Tumbes adolescents had higher rates of secondhand smoking exposure versus Lima adolescents (20.3% vs 12.8%, respectively; p<0.001). A greater proportion of adolescents reported ever smoking in Lima than in Tumbes (7.4% vs 2.2%, respectively; p<0.001).
Median concentrations of indoor PM in Lima were ∼2.4-fold higher than those in Tumbes (31 μg/m3 vs 13 μg/m3; p <0.001; figure 2). We speculate that indoor pollution levels probably reflect outdoor pollution levels at both sites for two reasons. First, most houses regularly left open doors (73% in Lima and 97% in Tumbes) or windows (75% in Lima and 94% in Tumbes) during the daytime year-round, and on average there were two windows and 1.4 doors left open at all times. Secondly, average 24 h outdoor PM2.5 concentrations in Lima were similar to indoor levels at 38 μg/m3 for 2009. Outdoor PM2.5 concentrations were not available in Tumbes.

{kind=link}
{kind=link}
Boxplots of median particulate matter concentrations (approximate PM2.5) in Lima and Tumbes; Peru 2009–2010.
Discussion
Adolescents living in peri-urban Lima were at a much higher risk of having asthma and allergy symptoms than their rural counterparts in Tumbes. Specifically, asthma symptoms were 2–3 times greater in Lima alongside a twofold increase in allergic symptoms, a 50% increase in atopy and a 15-fold increase in eczema. Adolescents in Lima also had a lower FEV1/FVC than did those in Tumbes. While postbronchodilator reversibility was also more common in Lima, this increase did not achieve statistical significance. Higher rates of asthma symptoms and atopy in Lima were associated with greater airways inflammation. Adolescents in Lima were exposed to higher levels of indoor air pollution, were more likely to smoke, had a greater mean BMI and were more likely to live in households with adequate sanitation facilities than adolescents in Tumbes. Thus, urbanisation is linked to several factors that may help explain why we would expect to see more asthma and atopy in Lima than in Tumbes.
It is well recognised that urbanisation is an important risk factor for asthma in both developed and developing countries.9 13–15 Most of the in-depth studies on urbanisation and asthma in developing countries have been conducted in Africa.21 A recent study conducted in Ghana found that urban poor adolescents had similar rates of exercise-induced bronchoconstriction to their rural counterparts, whereas wealthy urban adolescents had much higher rates.22 In our study, unlike the study in Ghana, urban poor adolescents had a two- to three-fold greater risk of asthma symptoms. Meanwhile, there is limited published information on how urbanisation affects asthma symptoms or quantitative asthma phenotypes in Latin America and what unique exposures may drive differences in the prevalence of asthma across varying degrees of urbanisation. One study performed in Costa Rica found that sensitisation to Ascaris lumbricoides was associated with reductions in FEV1 and FEV1/FVC, increased airway responsiveness and a greater number of asthma hospitalisations.23 Other studies have shown that the prevalence of asthma symptoms increases among Peruvian children living in areas of high traffic density,24 and that higher levels of air pollutants were associated with higher rates of emergency room asthma visits in Mexico City.25 In addition, the contributions of biomass fuels and indoor air pollution to asthma risk have not been carefully characterised in urban versus rural studies. In our study, we collected detailed information on biomass fuels and quantitative measurements of indoor PM. In Tumbes, nearly half of the households cooked with firewood on a daily or semi-daily basis. However, we did not observe a greater risk of asthma in adolescents who lived in households that used wood-burning stoves frequently. This may be because most wood-burning stoves in Tumbes were exclusively located outdoors. Since indoor PM concentrations were on average twice as great in Lima, outdoor biomass cooking did not appear to have a significant effect on indoor PM concentrations in Tumbes. As households in both sites had open connections to the environment year-round, we believe that these increased levels in Lima probably reflect high outdoor air pollution.
There are several risk factors that may help explain differences in asthma between our sites, such as obesity, diet and exposure to infections early in childhood. An increased BMI may be a consequence of a more sedentary lifestyle or changes in diet. In our study, overweight was a risk factor for asthma, which supports the conclusions of a recent systematic review.26 Diet has also been implicated in the development of asthma.27 Increased urbanisation can have a direct effect on changes in diet; however, we did not collect diet information. It is also possible that differences in rates of infections between Lima and Tumbes may help explain differences in asthma. Participants in Tumbes were more likely to have less access to adequate sanitation facilities that may increase their risk of infection; however, we did not have information on past history or current history of infections, nor did we test for parasitic infections. A greater sibship size is thought to be protective against asthma. We did not collect data on sibship size; however, there was no relationship between household size and either asthma or atopy. We also did not assess for airways hyper-responsiveness. Airways hyper-responsiveness is a marker of asthma, and previous studies in developing countries have shown >20% rates of exercise-induced bronchoconstriction in urban areas.13 16
We were surprised to find that adolescents in Lima had 10–15% larger FEVs than did those from Tumbes, accompanied by significantly larger percentage predicted values for FEV1 and FVC. We initially speculated that this difference may have been related to parental origins as they could not be explained by differences in the distributions of age, height or sex. While >95% of adolescents from our Lima site were born in Lima, over three-quarters had at least one parent that had emigrated from high-altitude rural areas. It has been previously reported that lung volumes are elevated in both native highlanders and non-native individuals living in the highlands.28–30 One possible explanation is that these children had a genetic predisposition to having greater lung volumes; however, this hypothesis needs further investigation. Despite these lung function differences, we did not see additional risk of asthma conveyed by having one or both parents from the highlands among Lima adolescents.
The peri-urban environment of Lima was associated with a 2.6-fold greater odds of current asthma after controlling for atopy, allergy symptoms, environmental exposures, household size, sanitation and sociodemographics. On the other hand, the risk of atopy only increased by 50%. This suggests that the higher prevalence of asthma in the peri-urban setting cannot be explained by the increase in atopy alone; there may be several contributing factors. For example, traffic in peri-urban Lima is poorly regulated and may be associated with an increased risk of both childhood asthma24 31 and atopy.31 Heavy traffic volumes also contribute to poor air quality. Our study found that indoor air pollution was also higher in Lima; however, we only collected indoor air pollution levels in a subset of households at both study sites and the relationship between environment and asthma and how it interacts with other risk factors such as genetic predisposition needs to be further explored. A higher rate of smoking alongside a higher prevalence of allergic rhinitis in peri-urban Lima may further predispose children to asthma symptoms.32 A higher rate of smoking may also contribute to decreased effectiveness of inhaled corticosteroid therapy in asthmatics.33
While it has become clear that eNO may be less useful in the diagnosis of asthma,34 it may be helpful in identifying participants with co-morbid asthma and atopy. In our study, eNO levels in Lima were higher because there was more asthma and atopy in this population. This corroborates recent findings,35 meanwhile suggesting that atopic asthma may be more severe than non-atopic asthma or that it may even be a related but distinct process altogether.
In summary, we found that the peri-urban environment is a risk factor for asthma and atopy. As urban centres in developing countries continue to grow, governments can implement policies to curb the effects of rapid urbanisation and urban health exposures. In doing so, they will not only improve quality of life for their urban inhabitants, but may also help curb the emerging asthma epidemic in many developing countries.
Acknowledgments
We are grateful to administrative and operations support staff at AB PRISMA in Lima, to Dr Hugo Garcia (Universidad Peruana Cayetano Heredia, Lima, Peru) and the Cysticercosis Elimination Project in Tumbes. Lincoln Diagnostics (Decatur, Illinois) and ALK-Abello (Round Rock, Texas) generously donated all skin prick atopy kits and antigens, respectively, used in this study. Aerocrine (New Providence, New Jersey) provided us, at discount, materials for eNO testing.
References
Supplementary materials
Web Only Data thx.2011.158956
Files in this Data Supplement:
Footnotes
See Editorial, p 1025
Funding The study was supported by the Johns Hopkins Center for Global Health (Principal Investigator NNH) and the Fogarty International Center, National Institutes of Health (NIH; grant R24 TW007988). WC was supported by a Clinician Scientist Award from the Johns Hopkins University, a K99/R00 Pathway to Independence Award (K99HL096955) from the National Heart, Lung and Blood Institute, NIH and by a contract (HHSN268200900033C) with the National Heart, Lung and Blood Institute, NIH. KCB was supported in part by the Mary Beryl Patch Turnbull Scholar Program. CLR was a Fogarty International Clinical Research Scholar during the time of the study and was further supported by Tufts University School of Medicine and by a pre-doctoral T35 Training Grant (T35AI065385) of the NIH. LMB was supported by a predoctoral T35 Training Grant (T35AI065385) of the NIH. Support for exposure measurements was provided by National Institute for Environmental Health Sciences grant numbers (ES015803). RAW was supported in part by the Dorney–Koppel Family Foundation. NNH, WC and PNB were also supported by an R01 grant from the National Institutes of Environmental Health Sciences (R01ES018845). Study sponsors played no role in the study design, data collection, data analysis, data interpretation or the decision to submit the article for publication. The opinions, results and conclusions reported in this paper are those of the authors and are independent from the funding sources. All authors had full access to all of the data (including statistical reports and tables) in the study and can take responsibility for the integrity of the data and the accuracy of the data analysis.
Competing interests None.
Ethics approval This study was conducted with the approval of the Institutional Review Boards of the Johns Hopkins Bloomberg School of Public Health in Baltimore, USA, and AB PRISMA in Lima, Peru.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Editorial