Article Text

Abstract
Background Chronic obstructive pulmonary disease (COPD) is a leading cause of morbidity and mortality worldwide. Gender differences in the clinical expression of COPD are increasingly recognised, but outcome differences have not been systematically examined. Gender differences in survival and rate of rehospitalisation were investigated in a large cohort of elderly patients with chronic airflow obstruction hospitalised for COPD.
Methods The databases from the Québec provincial health insurance plan were used. The study population included subjects aged >66 years who received ≥3 prescriptions for respiratory medications in any 1-year period between 1 January 1990 and 31 December 2001. The study cohort consisted of patients with a first hospitalisation for COPD, after selection into the study population. Patients were followed until death or 31 December 2003. The Kaplan–Meier method was used to estimate time to death and time to first hospitalisation for obstructive airways disease (COPD or asthma). The Cox proportional hazards model was used to determine the effect of male gender on all-cause mortality and rehospitalisation.
Results The cohort consisted of 19 260 women and 23 893 men with a mean age of 77 years. 11 245 (58.4%) women and 16 754 (70.1%) men died after cohort entry. Male sex was associated with a significantly increased risk of death (adjusted HR 1.45, 95% CI 1.42 to 1.49) and with a significantly increased risk of rehospitalisation for obstructive airways disease (adjusted HR 1.12, 95% CI 1.09 to 1.15).
Conclusion Mean survival and time to rehospitalisation for obstructive airways disease are significantly better for female patients.
- COPD
- obstructive airways disease
- gender
- sex
- survival
- COPD epidemiology
Statistics from Altmetric.com
Introduction
Chronic obstructive pulmonary disease (COPD) is characterised by progressive and mostly irreversible airflow obstruction. Smoking is by far the most important risk factor.1 COPD is a leading cause of morbidity and mortality worldwide, and is expected to become the third leading cause of death by the year 2020.2 The burden of disease has particularly increased among women. In 2000, for the first time, more women than men died of COPD in the USA.3
Gender differences in the clinical expression of COPD are increasingly recognised. Women tend to be younger and have a lesser smoking history in pack-years then men, yet report more severe dyspnoea.4 There is evidence to suggest that women may be more susceptible to the harmful effects of tobacco.5 6 Gender differences in the manifestations of severe pulmonary emphysema were noted in patients evaluated for the National Emphysema Treatment Trial. Radiographic analysis showed that the severity of emphysema was greater in men, while histological assessment in a subgroup of patients revealed smaller airway lumens with disproportionately thicker airway walls in women.7
Gender differences in outcome have not been systematically examined in patients with COPD. A study of gender differences in the survival of oxygen-dependent patients with COPD showed that women had a significantly higher risk of death than men.8 In contrast, all-cause and respiratory mortality were higher in men than in women with COPD when matched at baseline by the BODE index.9 In a large cohort of elderly patients with chronic airflow obstruction hospitalised for COPD, gender differences in survival and rate of rehospitalisation were investigated. The data contained in this paper were presented in abstract form at the 2010 American Thoracic Society meeting.10
Methods
The databases from the Québec provincial health insurance plan were used. The Régie de l'Assurance Maladie du Québec (RAMQ) administers the universal health insurance program for the 7.5 million residents of the Canadian province. The databases contain information on demographics, all medical services rendered along with ICD-9 or ICD-10 diagnostic codes and, for individuals aged ≥65 years, all outpatient prescription medications dispensed. The accuracy and comprehensiveness of the prescription claims database has been verified previously.11
Subjects with respiratory disease were identified using dispensed prescriptions for the following medications: any form of β agonist, theophylline, ipratropium bromide or inhaled corticosteroids (ICS). Patients who received ≥3 prescriptions for these respiratory medications in any 1-year period, dispensed on at least two separate occasions, constituted the study population. The third prescription for a respiratory medication occurred between 1 January 1990 and 31 December 2001 in subjects aged ≥66 years and was preceded by at least 1 year of prescription information.
The study cohort consisted of all subjects with a first hospitalisation for a primary diagnosis of COPD after selection into the study population. Cohort entry was taken as the date of discharge from this first hospitalisation for COPD (ICD-9 codes 490, 491, 492, 496 and ICD-10 codes J40, J41, J42, J43 and J44). All patients were followed until death or 31 December 2003. Age at the time of discharge from the index hospitalisation and length of follow-up after cohort entry were calculated. All hospitalisations for COPD were identified in the Med-Echo database. Subsequent and/or prior hospitalisations with a primary diagnosis of asthma were identified using the ICD-9 code 493 (asthma) and ICD-10 codes J45 (asthma) and J46 (status asthmaticus).
Prescriptions for the following respiratory medications dispensed in the year before cohort entry were tabulated for each subject: bronchodilators (β agonists, ipratropium bromide and theophylline), inhaled corticosteroids, oral corticosteroids and antibiotics used in the treatment of respiratory tract infections (designated ‘respiratory antibiotics’).
Comorbidities were measured using prescriptions for various classes of medications associated with the treatment of disorders of interest dispensed in the year prior to cohort entry. Diabetes was defined by dispensed insulin or an oral hypoglycaemic agent; cardiovascular disease by a prescription for cardiotropes, antihypertensives, diuretics, vasodilators or antiplatelet agents; CNS drugs included major tranquillisers, anticonvulsants and drugs for Parkinsonism or Alzheimer's dementia; osteoporosis drugs included calcium, vitamin D and bisphosphonates; rheumatic drugs included gold salts, methotrexate, azathioprine, chloroquine, hydroxychloroquine and sulfasalazine. Use of the newer antitumour necrosis factor α agents was minimal in this cohort. Prescriptions for benzodiazepines, antidepressant medications, non-steroidal anti-inflammatory drugs (NSAIDs) and narcotics were considered separately.
The date of death was obtained from the Institut de la Statistique du Québec (ISQ). Cause of death, as reported by the physician who completed the death certificate, is also recorded.
The Kaplan–Meier method was used to estimate time to death and time to first rehospitalisation for COPD alone and for obstructive airways disease (OAD), defined as either COPD or asthma. Cox proportional hazards models were used to determine the effect of male gender on death and repeat hospitalisation for COPD, OAD and all causes. The proportionality of hazards was verified using a graphical method. The analyses were adjusted for age, COPD or asthma hospitalisations in the year prior to cohort entry, comorbidities as defined above and respiratory medications dispensed in the year before cohort entry. All analyses were conducted using SAS Version 9.1. Graphs were designed using GrapPad Prism.
Results
The study population comprised 195 049 individuals receiving treatment for chronic airflow obstruction, of which 45 708 were hospitalised with a primary diagnosis of COPD. A total of 2555 patients were excluded: 2504 patients who died during the index hospitalisation and 51 individuals with an inconsistent end of follow-up date across the various databases.
The study cohort thus consisted of 19 260 women and 23 893 men (total 43 153 individuals) hospitalised with a primary diagnosis of COPD. Details of the baseline characteristics of the women and men in the study cohort are shown in table 1. The mean (SD) age of the women was 77.5 (6.5) years and of the men was 77.3 (6.2) years. All subjects had to have a minimum of 1 year of information in the database prior to cohort entry, and the mean (SD) duration of follow-up after cohort entry was 3.7 (3.0) years. The majority of patients in the study cohort (86.9% of individuals) had no prior COPD hospitalisations. Specifically, only 2.7% of women and 2.6% of men were hospitalised for COPD in the year prior to the index hospitalisation which marked cohort entry. When previous hospitalisations with a primary diagnosis of asthma were examined, 3.4% of women and 1.6% of men had been hospitalised for asthma in the year before cohort entry.
Baseline characteristics
The respiratory medications are presented as mean number of prescriptions dispensed in the year before cohort entry. The mean number of bronchodilator prescriptions dispensed (β2 agonists, ipratropium bromide and theophylline) was higher in men. The mean number of ICS prescriptions as well as the mean number of oral corticosteroid and respiratory antibiotic prescriptions dispensed to men and women were similar.
The prevalence of diabetes, CNS disease and rheumatic disease were similar in men and women. More women were dispensed cardiovascular medications in the year before cohort entry (78.5% vs 71.9%) and more women received osteoporosis medications (13.6% vs 3.8%). A significantly higher proportion of women than men were dispensed benzodiazepines and antidepressant drugs in the year prior to being hospitalised for COPD (62.5% vs 48.7% and 20.3% vs 11.3%, respectively). More women than men were dispensed narcotics and NSAIDs.
A total of 11 245 women (58.4%) and 16 754 (70.1%) men died after cohort entry. The causes of death are shown in table 2. The information was missing in 2.2% of deceased subjects. The most common cause of death was COPD, accounting for 32% of all deaths in women and 36% in men. A very small proportion of deaths were attributed to asthma (79/11 245 deaths in women and 38/16 754 deaths in men). The second most common cause of death was cardiovascular disease, responsible for 26% of all female deaths and 24% of all male deaths. Lung cancer was the documented cause of death in 7% of women and 10% of men.
Causes of death
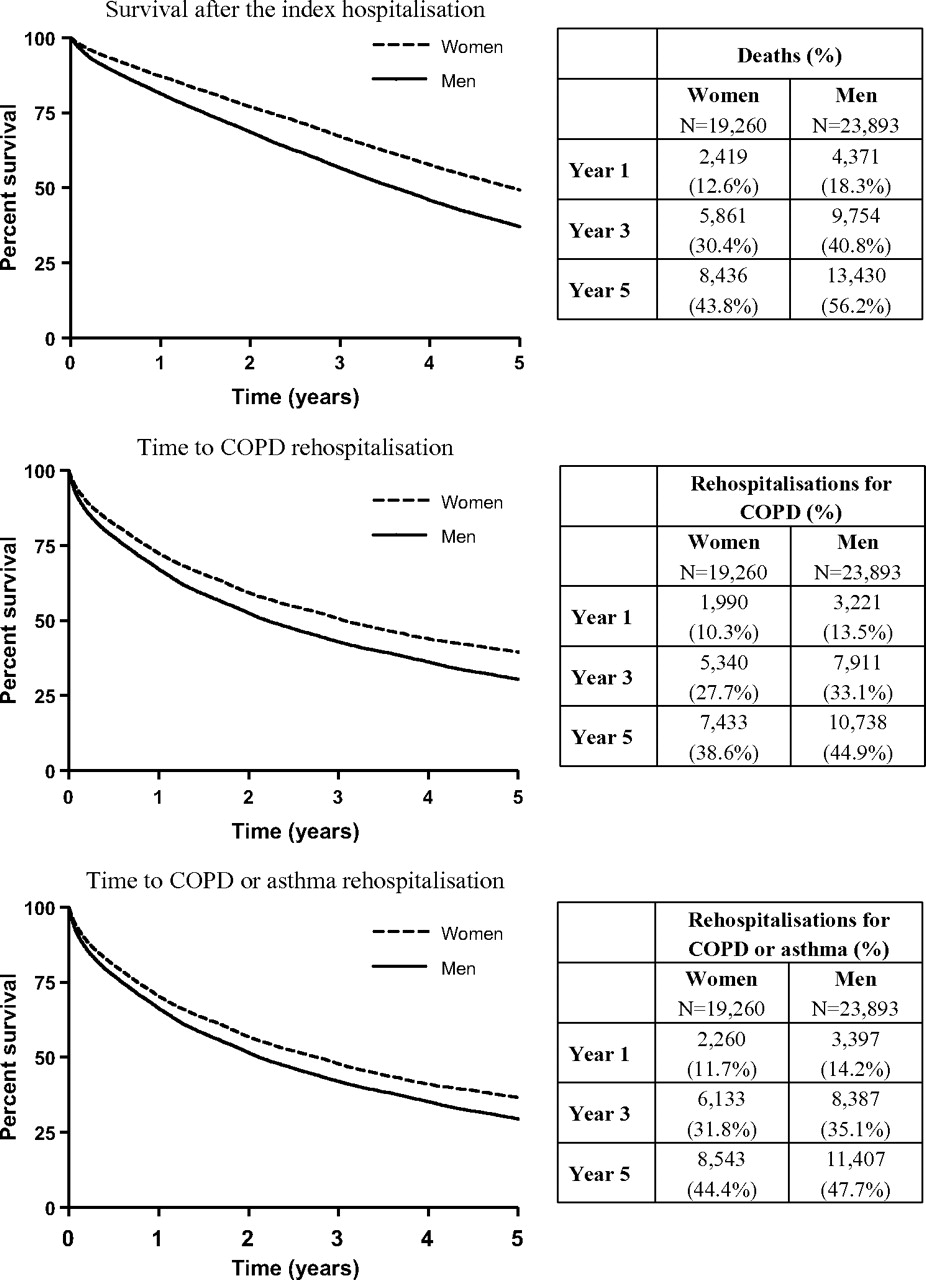
The Kaplan-Meier method was used to estimate survival and time to rehospitalisation for COPD or OAD (figure 1). Cox's regression model was used to examine the effect of gender on mortality and risk of rehospitalisation for OAD (table 3). After adjusting for age, COPD or asthma hospitalisation in the year prior to cohort entry, comorbidities and respiratory medications dispensed, male gender was found to be associated with a significantly increased risk of death (HR 1.45, 95% CI 1.42 to 1.49). Male sex was associated with a lesser though still significantly increased risk of rehospitalisation for OAD (HR 1.12, 95% CI 1.09 to 1.15). The risk of all-cause rehospitalisation was also significantly higher in men (HR 1.14, 95% CI 1.12 to 1.17). The effects of age and prior COPD or asthma hospitalisation on mortality and risk of rehospitalisation (OAD and all-cause) are shown in table 4.
{kind=link}
Survival and time to rehospitalisation for COPD or obstructive airways disease (COPD or asthma).
HRs of mortality and rehospitalisation for COPD, OAD and all causes for men relative to women
Contribution of other covariates to mortality and risk of rehospitalisation (OAD and all-cause)
Discussion
Although COPD was considered a typically male disease in the past, increases in female smoking over the course of the 20th century have translated into a prevalence of COPD that is still rising in women. Investigators only recently began focusing their attention on possible differences in the clinical expression and evolution of disease in men and women with COPD. In a large cohort of elderly patients with chronic airflow obstruction hospitalised for COPD, mean survival and time to rehospitalisation for OAD were found to be significantly better in women.
The study population consisted of subjects who were dispensed respiratory medications used in the treatment of OAD. Patients entered the study cohort upon discharge from the first COPD hospitalisation that followed the initiation of outpatient respiratory medications. The current results therefore apply to patients with COPD of sufficient severity to require being prescribed respiratory medications more than occasionally and to have been hospitalised with COPD as the primary cause. Choosing as our point of departure a hospitalisation for COPD increases the likelihood that the patients studied actually do have COPD. Mortality and rehospitalisation are hard endpoints which are clearly documented within the RAMQ databases. We chose also to examine rehospitalisation for OAD, which encompasses both COPD and asthma hospitalisations after cohort entry, to avoid missing repeat hospitalisations in women who were more likely than men to have been previously hospitalised for asthma. Indeed, rehospitalisation with a primary diagnosis of asthma was more frequent among women in our cohort of patients hospitalised for COPD, yet the risk of rehospitalisation for either COPD or asthma remained higher in men.
The study suffers from the limitations typical of database analyses. Information on risk factors for COPD, particularly smoking and family history, as well as lung function records are not part of the RAMQ databases. This was not an incidence cohort as subjects could be hospitalised for COPD prior to their selection into the study population. However, only a small proportion of cohort subjects were hospitalised for COPD or asthma in the year before the index hospitalisation marking cohort entry. Using COPD hospitalisation as the defining event for cohort entry, we were able to prospectively follow a large group of subjects who were likely to be at similar points in the natural history of their disease.
Gender differences in survival have previously been examined in selected groups of patients with COPD; these studies have yielded conflicting results. A prospective cohort study of 435 patients with COPD (184 women) referred for long-term oxygen therapy was conducted by Machado and colleagues.8 After adjusting for potential confounders including age, pack-years smoked, arterial oxygen tension, forced expiratory volume in 1 s (FEV1) and body mass index, women were found to be at significantly higher risk of death. In contrast, other studies have found survival to be better among women prescribed long-term oxygen therapy. Miyamoto et al analysed survival in a large group of patients receiving home oxygen for chronic respiratory failure due to various causes (COPD, sequelae of tuberculosis, chronic interstitial pneumonia and others) and found that women had a better prognosis than men.12 Women on long-term oxygen therapy for COPD experienced better survival than men in a study by Crocket et al.13 In Swedish patients prescribed oxygen therapy for COPD from 1987 to 2000, women were also found to have a better survival.14 These studies pertain to patients further along in the natural history of COPD.
Differences in survival in men and women with COPD were recently examined by De Torres and colleagues.9 After patients were matched on severity at baseline by their BODE index,15 all-cause and respiratory mortality was found to be significantly higher in man than in women at similar COPD severity. In patients from the Copenhagen City Heart Study hospitalised for COPD, Vestbo et al also found a significantly higher mortality risk in men after adjusting for age and FEV1.16 In our cohort of patients discharged from a COPD hospitalisation, survival was significantly higher for women. After adjustment for age, prior COPD and asthma hospitalisations, comorbidities and respiratory medications dispensed, male sex was associated with a 45% excess in the risk of death.
The survival advantage of women in our cohort is unlikely to result from asthma being mislabelled as COPD. Mislabelling of female respiratory symptoms by physicians has been described, but tends to occur in the opposite direction. Gender bias in physician diagnosis was first suspected by Dodge and Burrows in the Tucson study.17 Similar symptoms in subjects aged >40 years were much more likely to lead to a diagnosis of asthma in women than men. Chapman and colleagues reported similar findings following a survey of 192 primary care physicians.18 When physicians were presented with the hypothetical case of a smoker with cough and dyspnoea, COPD was given as the most probable diagnosis significantly more often for men than women, with more women receiving the alternative diagnosis of asthma.
Asthma hospitalisation in the year before cohort entry conferred a significantly lower risk of death. This is consistent with the findings of Burrows and colleagues who reported a much better survival in subjects with asthma and asthmatic bronchitis than in patients with emphysematous COPD.19 This finding suggests that asthma diagnoses preceding the index hospitalisation were mostly valid, or constitute markers of favourable disease features such as a higher reversibility of airflow obstruction with treatment. Patients with asthma and chronic asthmatic bronchitis in the study by Burrows et al were mostly female, while patients with emphysema were predominantly male. The improved survival among women in this cohort, however, does not appear to be due to the inclusion of a large number of patients with asthma. Only 3.4% of women and 1.6% of men were hospitalised for asthma in the year before cohort entry. The HR of mortality for male versus female gender was recalculated after the exclusion of patients with a prior asthma hospitalisation any time before cohort entry and was essentially unchanged (HR 1.43, 95% CI 1.39 to 1.47).
The survival advantage of women could be attributed to a lesser severity of respiratory disease. Because COPD hospitalisation was the defining event for cohort entry, moderate to severe impairment might be anticipated among all cohort subjects. The numbers of prescriptions for respiratory antibiotics and oral corticosteroids dispensed in the year prior to the index hospitalisation were examined as markers of disease severity and were comparable in men and women. This suggests that selecting our cohort on the basis of hospitalisation for COPD did result in homogeneity as to disease severity. The high death rate in both men and women following the index hospitalisation further attests to the severity of disease in this cohort.
In the present study, 13% of women and 18% of men died in the first year following cohort entry. The 5-year survival was approximately 55% in women and 45% in men. This is similar to results seen in previous smaller studies.16 20 In the general population, differences in lifespan between men and women are large and incompletely understood.21 22 We thought these differences might be eliminated by comparing men and women after hospitalisation for a COPD exacerbation. The persistent survival advantage for women despite significant COPD suggests the presence of factors associated with longevity other than the comorbidities we adjusted for in the analysis.
We assessed comorbidities using prescriptions for medications used in the treatment of the various disorders of interest dispensed in the year before cohort entry.23 More women than men were dispensed cardiovascular medications in the year before hospitalisation for COPD, while the proportion of men and women dispensed medications for diabetes was similar. More women were treated for osteoporosis. Interestingly, more women than men were dispensed benzodiazepines and antidepressants drugs in the year preceding the index hospitalisation. Previous studies have reported a higher prevalence of anxiety and depression among women with COPD,24 and anxiety has been shown to contribute to the risk of repeat hospitalisation in patients with COPD.25 These comorbidities were adjusted for in the multivariate analyses and do not explain the differences in survival observed.
The most commonly documented cause of death was COPD, accounting for approximately one-third of deaths in both men and women. This may be an underestimate as prior data suggest that death in patients with COPD may be attributed to other causes such as congestive heart failure or pneumonia.26 The second most common cause of death in both men and women was cardiovascular disease. A smaller proportion of women died of COPD (32% vs 36% of men), while the proportions of women and men dying of cardiovascular diseases was more similar. The survival advantage of women in this cohort is probably mediated by reduced and/or delayed COPD mortality; a contribution of delayed cardiovascular mortality is also likely. The proportions of men and women dying of lung cancer in this cohort (7% and 10%, respectively) are too small to account for the large differences in mortality observed.
The mechanisms that mediate the survival advantage of women following discharge from a COPD hospitalisation cannot be fully elucidated from the current dataset. Gender differences in the COPD disease phenotype may explain some of the outcome differences observed between women and men in our cohort. Gender differences in the manifestations of severe pulmonary emphysema were recently examined in 1053 patients evaluated for lung volume reduction surgery as part of the National Emphysema Treatment Trial.7 Radiographic assessment showed that the proportion of whole lung emphysema was lower in women, with less peripheral involvement. Histological assessment in a subgroup of 101 patients (41.6% female) revealed anatomically smaller airway lumens with disproportionately thicker airway walls in women. The presence of more severe emphysema in men with COPD has been confirmed by CT scanning.27 28 A predominant ‘airway phenotype’ in women with COPD may translate into significantly different treatment responses, and this warrants further investigation. In addition, the existence of an overlap syndrome of asthma and COPD is increasingly recognised29; gender differences in the epidemiology of this syndrome are plausible and could play a role in the important outcome differences observed in the present study.
In conclusion, mean survival and time to rehospitalisation for OAD were found to be significantly better for women than for men in a large cohort of elderly subjects hospitalised for COPD. Further work is required to elucidate the factors that confer a survival advantage to women following a COPD hospitalisation.
References
Footnotes
Funding AVG was the recipient of a CLA/CIHR/GSK fellowship.
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.