Article Text

Abstract
Introduction US Guidelines define healthcare associated pneumonia (HCAP) as patients with regular contact with healthcare (eg, nursing home residents, patients with recent hospital admissions or regular outpatient clinics). It is argued that such patients are more likely to develop infection with resistant organisms and require broader spectrum antibiotics. UK guidelines do not distinguish between HCAP and community-acquired pneumonia (CAP). The aim of this study was to investigate whether HCAP is a distinct clinical phenotype.
Methods We studied consecutive patients aged 18+ presenting to an emergency department with CAP according to current UK definitions (NHS Lothian 2006–2009). Exclusion criteria included hospital acquired pneumonia, immunosupressed patients, and patients not actively treated (palliative). Cases were reviewed by two investigators and HCAP patients were defined according to 2005 ATS/IDSA guidelines. Survival was analysed by Kaplain–Meier analysis and logistic regression.
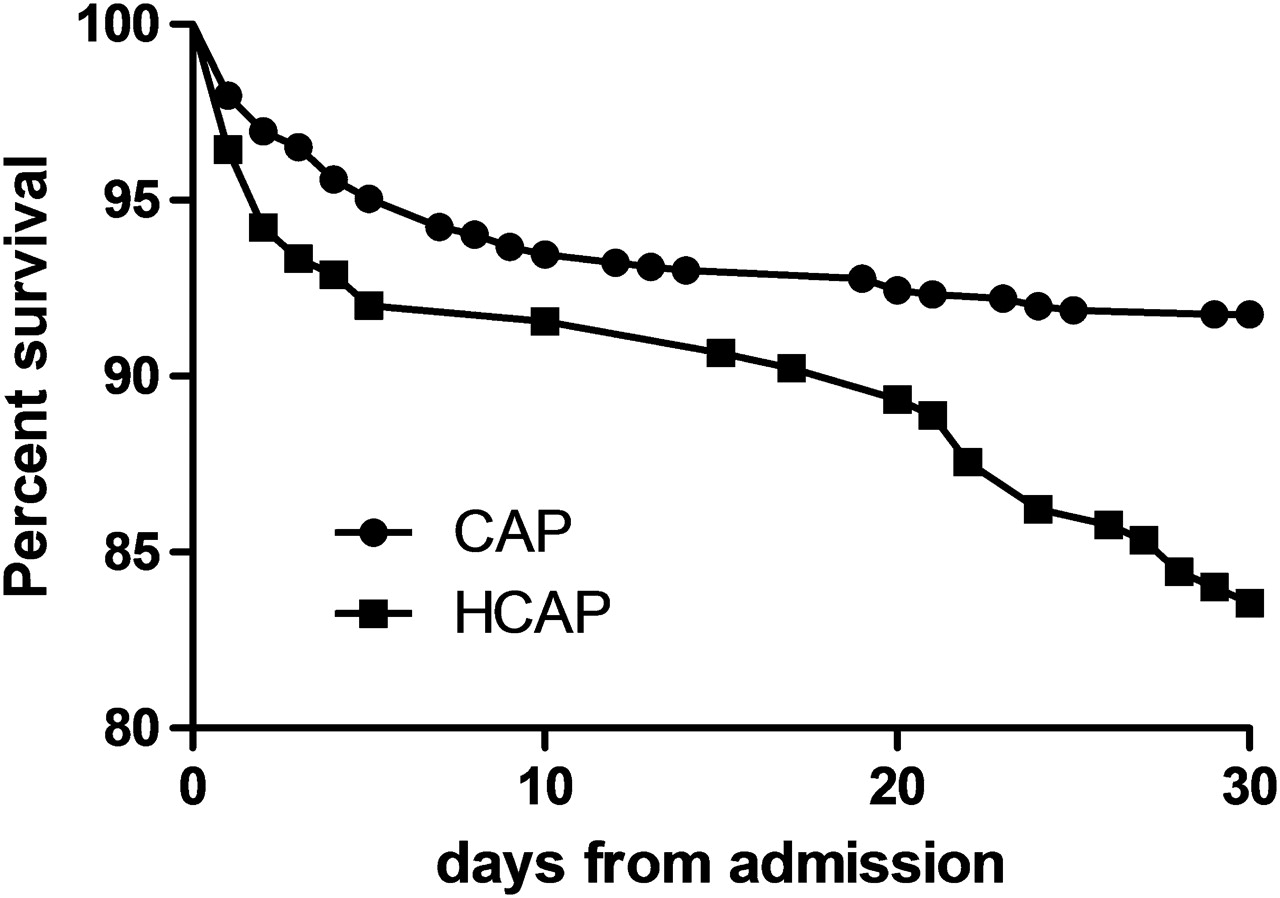
Results This study analysed 1111 consecutive patients. Of these, 224 (20.2%) met the criteria for HCAP (39.3% hospitalised within 3 months, 37.5% nursing home residents, 10.7% recent outpatient appointments, 12.5% ‘other’). 96.4% of HCAP patients received standard ‘CAP’ antibiotic therapy without coverage of Pseudomonas aeruginosa or MRSA. Demographic comparison of HCAP and CAP patients showed HCAP patients were significantly older (median age 76 vs 64, p<0.0001) and more likely to have co-morbidities, for example, congestive cardiac failure (30% vs 17%, p<0.0001), COPD (33.5% vs 20.8%, p<0.0001). HCAP patients had higher markers of severity and worse outcomes on univariate analysis. Mean admission CURB65 score was greater (2.32 vs 1.78, p<0.0001), median length of stay was longer (7 vs 5 days, p=0.01) and 30-day mortality was double that of CAP patients (16.5% vs 8.2%, p=0.0004). Kaplain–Meier analysis showed higher mortality for HCAP patients (Log rank test χ2 13.24 df=1, p=0.0003) as shown in Abstract S127 Figure 1. On multivariate analysis, however, after adjustment for age, co-morbidities and initial pneumonia severity, HCAP was not independently associated with increased 30-day mortality AOR 1.13 (0.69–1.84, p=0.6).

{kind=link}
Conclusions Healthcare associated pneumonia is common, with around 20% of CAP patients meeting the definition. Although HCAP patients are older and have more co-morbidities, HCAP is not independently associated with 30-day mortality.