Article Text

Abstract
Background Measures of ventilatory efficiency during cardiopulmonary exercise testing (CPX), such as the VE/VCO2 slope and ventilatory equivalent for CO2 at anaerobic threshold (EqCO2_AT), are increasingly being used as prognostic markers in heart failure and pulmonary arterial hypertension (PAH). Little is known about whether these measures can be applied to all forms of PH, in particular chronic thromboembolic pulmonary hypertension (CTEPH), where thrombotic vascular occlusion may an impact on gas exchange through increased dead space fraction.
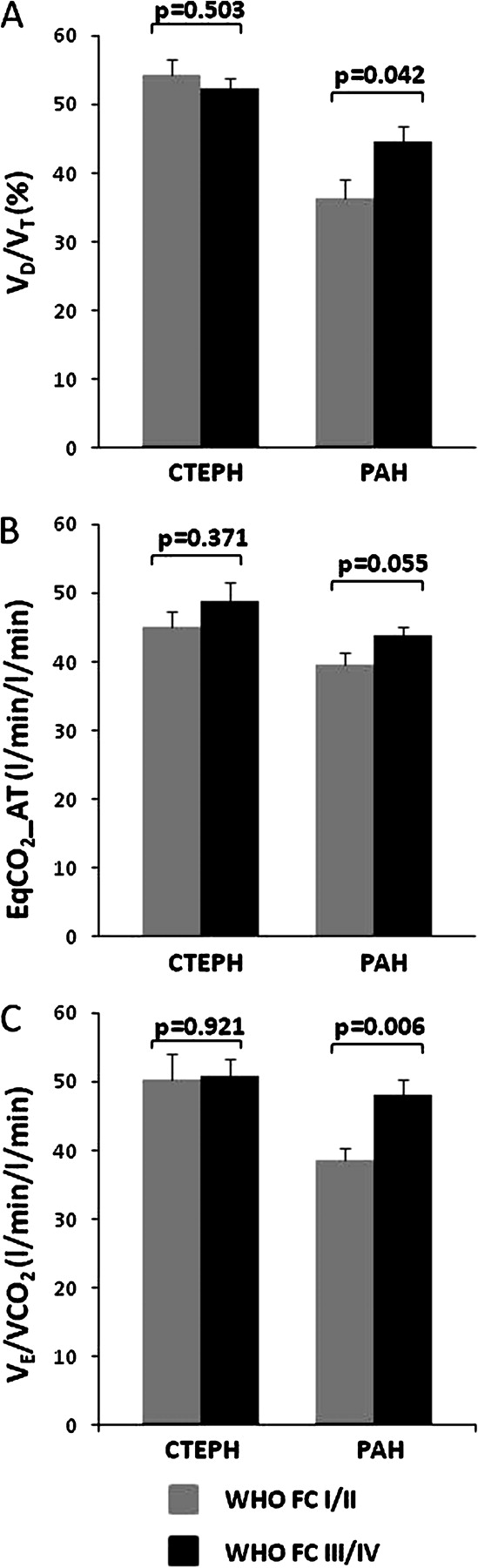
Methods and results 127 patients, 77 with CTEPH and 50 with PAH, underwent incremental CPX. Ventilatory dead space fraction (VD/VT) measured at peak exercise with arterial blood gas analysis was higher in CTEPH than PAH (52.9 vs 41.8, p<0.001).The VE/VCO2 slope was higher in CTEPH patients than in PAH patients (50.7 vs 44.4, p=0.024) and was mirrored by similar changes in EqCO2_AT (47.7 vs 42.0 p=0.008). Multivariate analysis demonstrated disease subtype to be a powerful independent predictor of VD/VT (p<0.001), VE/VCO2 slope (p=0.003) and EqCO2_AT (p<0.001). These three measures could distinguish between WHO functional classes I/II and III/IV in PAH, but not CTEPH (Abstract S98 Figure 1). As a result of increased ventilatory inefficiency in CTEPH, breathing reserve was lower at peak exercise compared with PAH (29.0 vs 38.8, p=0.003) despite similar peak VO2 and heart rate reserves.

{kind=link}
Conclusion Significant differences in gas exchange exist between CTEPH and PAH, possibly due to differences in VD/VT as a result of vascular occlusion due to thromboembolic disease. These findings increase our understanding of the mechanisms of exercise limitation in subtypes of pulmonary hypertension, with increased dependence on gas exchange and ventilatory capacity in CTEPH. Furthermore these differences in gas exchange dissociate measures of ventilatory efficiency from disease severity in CTEPH. Caution should be applied in using common prognostic end-points from CPX in all forms of pulmonary hypertension.