Article Text

Statistics from Altmetric.com
Introduction
The discovery of malignant cells in pleural fluid and/or parietal pleura signifies disseminated or advanced disease and a reduced life expectancy in patients with cancer.1 Median survival following diagnosis ranges from 3 to 12 months and is dependent on the stage and type of the underlying malignancy. The shortest survival time is observed in malignant effusions secondary to lung cancer and the longest in ovarian cancer, while malignant effusions due to an unknown primary have an intermediate survival time.2–6 Historically, studies showed that median survival times in effusions due to carcinoma of the breast are 5–6 months. However, more recent studies have suggested longer survival times of up to 15 months.7–10 A comparison of survival times in breast cancer effusions in published studies to 1994 calculated a median survival of 11 months.9
Currently, lung cancer is the most common metastatic tumour to the pleura in men and breast cancer in women.4 11 Together, both malignancies account for 50–65% of all malignant effusions (table 1). Lymphomas, tumours of the genitourinary tract and gastrointestinal tract account for a further 25%.2 12–14 Pleural effusions from an unknown primary are responsible for 7–15% of all malignant pleural effusions.3 13 14 Few studies have estimated the proportion of pleural effusions due to mesothelioma: studies from 1975, 1985 and 1987 identified mesothelioma in 1/271, 3/472 and 22/592 patients, respectively, but there are no more recent data to update this in light of the increasing incidence of mesothelioma.4 13 14
Primary tumour site in patients with malignant pleural effusion
Attempts have been made to predict survival based on the clinical characteristics of pleural fluid. None has shown a definite correlation: a recent systematic review of studies including 433 patients assessing the predictive value of pH concluded that low pH does not reliably predict a survival of <3 months.15 16 In malignant mesothelioma, one study has shown an association between increasing pH and increasing survival.17 Burrows et al showed that only performance status was significantly associated with mortality: median survival was 1.1 months with a Karnofsky score <30 and 13.2 months with a score >70.18
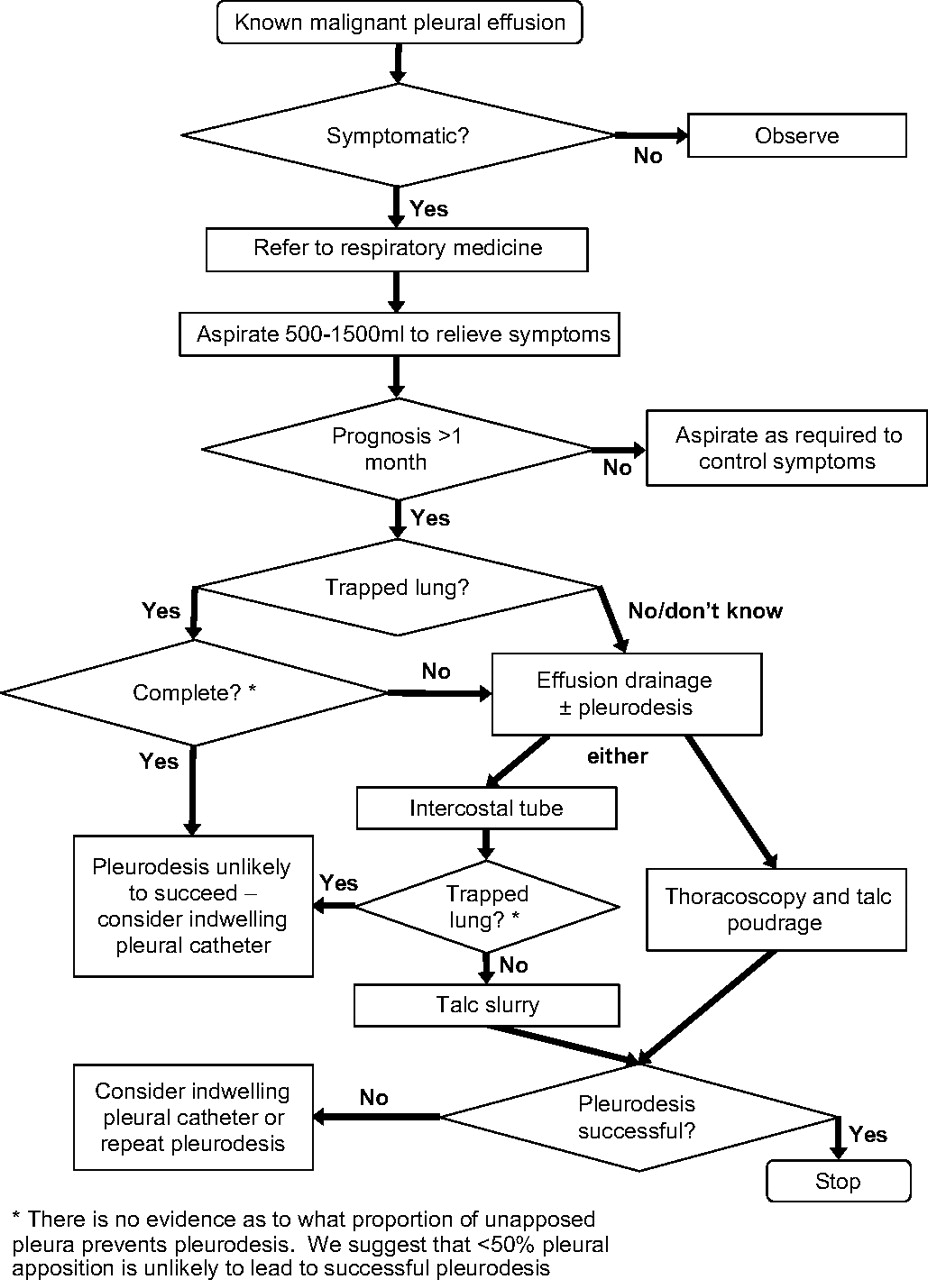
An algorithm for the management of malignant pleural effusions is shown in figure 1.
{kind=link}
Management algorithm for malignant pleural effusion.
Clinical presentation
The majority of malignant effusions are symptomatic. (C)
Massive pleural effusions are most commonly due to malignancy. (C)
The majority of patients who present with a malignant pleural effusion are symptomatic, although up to 25% are asymptomatic with an incidental finding of effusion on physical examination or by chest radiography.1 Dyspnoea is the most common presenting symptom, reflecting reduced compliance of the chest wall, depression of the ipsilateral diaphragm, mediastinal shift and reduction in lung volume.19 Chest pain is less common and is usually related to malignant involvement of the parietal pleura, ribs and other intercostal structures. Constitutional symptoms including weight loss, malaise and anorexia generally accompany respiratory symptoms.
A massive pleural effusion is defined as complete or almost complete opacification of a hemithorax on the chest x-ray. It is usually symptomatic and is commonly associated with a malignant cause.20 The diagnosis of a malignant pleural effusion is discussed in the guideline on the investigation of a unilateral pleural effusion.
Management options
Treatment options for malignant pleural effusions are determined by several factors: symptoms and performance status of the patient, the primary tumour type and its response to systemic therapy, and degree of lung re-expansion following pleural fluid evacuation. Although small cell lung cancer, lymphoma and breast cancer usually respond to chemotherapy, associated secondary pleural effusions may require intervention during the course of treatment (figure 1). Malignant pleural effusions are often most effectively managed by complete drainage of the effusion and instillation of a sclerosant to promote pleurodesis and prevent recurrence of the effusion. Options for management include observation, therapeutic pleural aspiration, intercostal tube drainage and instillation of sclerosant, thoracoscopy and pleurodesis or placement of an indwelling pleural catheter.
Observation
Observation is recommended if the patient is asymptomatic and the tumour type is known. (C)
Advice should be sought from the respiratory team and/or respiratory multidisciplinary team for symptomatic malignant effusions. (✓)
The majority of these patients will become symptomatic in due course and require further intervention. There is no evidence that initial thoracentesis carried out according to standard techniques will reduce the chances of subsequent effective pleurodesis after tube drainage. However, repeated thoracentesis may limit the scope for thoracoscopic intervention as it often leads to the formation of adhesions between the parietal and visceral pleura.
Therapeutic pleural aspiration
Pleural effusions treated by aspiration alone are associated with a high rate of recurrence of effusion at 1 month so aspiration is not recommended if life expectancy is >1 month. (A)
Caution should be taken if removing >1.5 l on a single occasion. (C)
Repeated therapeutic pleural aspiration provides transient relief of symptoms and avoids hospitalisation for patients with limited survival expectancy and poor performance status. It is appropriate for frail or terminally ill patients. However, as small-bore chest tubes are widely available, effective and may be inserted with minimal discomfort,21–26 they may be preferable. The amount of fluid evacuated by pleural aspiration will be guided by patient symptoms (cough, chest discomfort)27 and should be limited to 1.5 l on a single occasion. Pleural aspiration alone and intercostal tube drainage without instillation of a sclerosant are associated with a high recurrence rate and a small risk of iatrogenic pneumothorax and empyema.28–36 Therapeutic pleural aspiration should take place under ultrasound guidance (see guideline on pleural procedures).
Intercostal tube drainage and intrapleural instillation of sclerosant
Other than in patients with a very short life expectancy, small-bore chest tubes followed by pleurodesis are preferable to recurrent aspiration. (✓)
Intercostal drainage should be followed by pleurodesis to prevent recurrence unless lung is significantly trapped. (A)
Pleurodesis is thought to occur through a diffuse inflammatory reaction and local activation of the coagulation system with fibrin deposition.37 38 Increased pleural fibrinolytic activity is associated with failure of pleurodesis, as is extensive tumour involvement of the pleura.39 40 Intercostal drainage without pleurodesis is associated with a high rate of effusion recurrence and should be avoided (see evidence table available on the BTS website at www.brit-thoracic.org.uk). A suggested method for undertaking pleurodesis is shown in box 1.
Box 1 How to perform talc slurry chemical pleurodesis
Insert small-bore intercostal tube (10–14 F).
Controlled evacuation of pleural fluid.
Confirm full lung re-expansion and position of intercostal tube with chest x-ray. In cases where incomplete expansion occurs, see text regarding trapped lung.
Administer premedication prior to pleurodesis (see text).
Instill lidocaine solution (3 mg/kg; maximum 250 mg) into pleural space followed by 4-5 g sterile graded talc in 50 ml 0.9% saline.
Clamp tube for 1-2 h.
Remove intercostal tube within 24-48 h.
In animals the effectiveness of pleurodesis may be reduced by concomitant use of corticosteroids. Recent evidence in rabbits has shown reduced pleural inflammatory reaction and, in some cases, prevention of pleurodesis with administration of corticosteroids at the time of talc pleurodesis.41 A subgroup analysis comparing the efficacy of pleurodesis in the presence and absence of non-randomised oral corticosteroid use also suggested a negative effect of corticosteroids on efficacy.42 The administration of non-steroidal anti-inflammatory drugs (NSAIDs) at the time of pleurodesis is more contentious. Animal studies have suggested that the use of NSAIDs may impair the action of pleurodesis agents, but there is no evidence from human studies.43
Size of intercostal tube
Small-bore (10–14 F) intercostal catheters should be the initial choice for effusion drainage and pleurodesis. (A)
Conventional large-bore intercostal tubes (24–32 F) have been employed in most studies involving sclerosing agents.44 They have traditionally been used because they are thought to be less prone to obstruction by fibrin plugs, but there is little published evidence to confirm this. The placement of large-bore tubes is perceived to be associated with significant discomfort45 and this has led to the assessment of smaller bore tubes (10–14 F) for drainage and administration of sclerosing agents.22 46 47 Three randomised trials investigating the difference in efficacy between small- and large-bore chest tubes all concluded that they were equivalent (see evidence table available on the BTS website at www.brit-thoracic.org.uk).21–23 Studies using small-bore intercostal tubes with commonly used sclerosants have reported similar success rates to large-bore tubes and appear to cause less discomfort.24–26 48 The small-bore tubes in these studies were inserted either at the patient's bedside by a physician or under radiological guidance.
Small-bore tubes have been used for ambulatory or outpatient pleurodesis. Patz and colleagues used a fluoroscopically-placed tube (10 F) connected to a closed gravity drainage bag system for this purpose.49 Bleomycin was the preferred sclerosing agent and the pleurodesis success rate approached 80%. Ambulatory drainage is discussed further in the section on indwelling pleural catheters.
Fluid drainage, pleurodesis and trapped lung
Large pleural effusions should be drained in a controlled fashion to reduce the risk of re-expansion pulmonary oedema. (C)
In patients where only partial pleural apposition can be achieved, chemical pleurodesis may still be attempted and may provide symptomatic relief. (B)
In symptomatic cases where pleural apposition cannot be achieved (‘trapped lung’), indwelling pleural catheters offer a more attractive therapeutic approach than recurrent aspiration. (✓)
Once effusion drainage and lung re-expansion have been radiographically confirmed, pleurodesis should not be delayed. (B)
Suction to aid pleural drainage before and after pleurodesis is usually unnecessary but, if applied, a high-volume low-pressure system is recommended. (C)
Large pleural effusions should be drained incrementally, draining a maximum of 1.5 l on the first occasion. Any remaining fluid should be drained 1.5 l at a time at 2 h intervals, stopping if the patient develops chest discomfort, persistent cough or vasovagal symptoms. Re-expansion pulmonary oedema is a well-described serious but rare complication following rapid expansion of a collapsed lung through evacuation of large amounts of pleural fluid on a single occasion and the use of early and excessive pleural suction.50 51 Putative pathophysiological mechanisms include reperfusion injury of the underlying hypoxic lung, increased capillary permeability and local production of neutrophil chemotactic factors such as interleukin-8.52 53
The most important requirement for successful pleurodesis is satisfactory apposition of the parietal and visceral pleura, confirmed radiologically.44 54 55 Incomplete lung re-expansion may be due to a thick visceral peel (‘trapped lung’), pleural loculations, proximal large airway obstruction or a persistent air leak. Most studies indicate that the lack of a response following instillation of a sclerosant is associated with incomplete lung expansion.56 Where complete lung re-expansion or pleural apposition is not achieved, pleurodesis may still be attempted or an indwelling pleural catheter may be inserted. Robinson and colleagues reported a favourable response in 9 out of 10 patients with partial re-expansion of the lung in a study using doxycycline as a sclerosing agent.57 The amount of trapped lung compatible with successful pleurodesis is unknown. Complete lack of pleural apposition will prevent pleurodesis: consideration of an indwelling pleural catheter is recommended in this situation. Where more than half the visceral pleura and parietal pleura are apposed, pleurodesis may be attempted although there are no studies to support this recommendation.
The amount of pleural fluid drained per day before the instillation of a sclerosant (<150 ml/day) is less relevant for successful pleurodesis than radiographic confirmation of fluid evacuation and lung re-expansion. In a randomised study, a shorter period of intercostal tube drainage and hospital stay was seen in the group in whom sclerotherapy was undertaken as soon as complete lung re-expansion was documented (majority <24 h) than in the group in whom pleurodesis was attempted only when the fluid drainage was <150 ml/day. The success rate in both groups approached 80%.55 After sclerosant instillation, the duration of intercostal drainage appears not to affect the chances of successful pleurodesis, although the only randomised study to address this question was underpowered.58
Suction may rarely be required for incomplete lung expansion and a persistent air leak. When suction is applied, the use of high-volume low-pressure systems is recommended with a gradual increment in pressure to about –20 cm H2O.
Analgesia and premedication
Lidocaine (3 mg/kg; maximum 250 mg) should be administered intrapleurally just prior to sclerosant administration. (B)
Premedication should be considered to alleviate anxiety and pain associated with pleurodesis. (C)
Intrapleural administration of sclerosing agents may be painful; significant pain is reported in 7% patients receiving talc to 60% with historical agents such as doxycycline.57 59 Discomfort can be reduced by administering local anaesthetic via the drain prior to pleurodesis. Lidocaine is the most frequently studied local anaesthetic for intrapleural administration. The onset of action of lidocaine is almost immediate and it should therefore be administered just before the sclerosant. The maximum dose of lidocaine is 3 mg/kg (21 ml of a 1% lidocaine solution for a 70 kg male), with a ceiling of 250 mg. The issue of safety has been highlighted in two studies. Wooten et al60 showed that the mean peak serum concentration of lidocaine following 150 mg of intrapleural lidocaine was 1.3 μg/ml, well below the serum concentration associated with central nervous system side effects (ie, >3 μg/ml). In an earlier study of 20 patients, larger doses of lidocaine were necessary to achieve acceptable levels of local anaesthesia. The patients receiving 250 mg lidocaine had more frequent pain-free episodes than those given 200 mg, while serum levels remained within the therapeutic range. Side effects were limited to transient paraesthesiae in a single patient.61 The reason for the significant difference in analgesia between the two groups with only a small increment in the lidocaine dose was unclear.
There are no studies to inform a recommendation on the use of premedication and sedation in non-thoracoscopic pleurodesis. Pleurodesis is an uncomfortable procedure and is associated with anxiety for the patient. The use of sedation may be helpful to allay such fears and induce amnesia. The level of sedation should be appropriate to relieve anxiety but sufficient to maintain patient interaction. Sedation employed before pleurodesis should be conducted with continuous monitoring with pulse oximetry and in a setting where resuscitation equipment is available.62 Further research is underway to address this issue.
Sclerosant and complications
Talc is the most effective sclerosant available for pleurodesis. (A)
Graded talc should always be used in preference to ungraded talc as it reduces the risk of arterial hypoxaemia complicating talc pleurodesis. (B)
Talc pleurodesis is equally effective when administered as a slurry or by insufflation. (B)
Bleomycin is an alternative sclerosant with a modest efficacy rate. (B)
Pleuritic chest pain and fever are the most common side effects of sclerosant administration. (B)
An ideal sclerosing agent must possess several essential qualities: a high molecular weight and chemical polarity, low regional clearance, rapid systemic clearance, a steep dose-response curve and be well tolerated with minimal or no side effects. The choice of a sclerosing agent will be determined by the efficacy or success rate of the agent, accessibility, safety, ease of administration, number of administrations to achieve a complete response and cost. Despite the evaluation of a wide variety of agents, to date no ideal sclerosing agent exists.
Comparison of sclerosing agents is hampered by the lack of comparative randomised trials, different eligibility criteria and disparate criteria for measuring response and end points. A complete response is usually defined as no reaccumulation of pleural fluid after pleurodesis until death, and a partial response as partial reaccumulation of fluid radiographically but not requiring further pleural intervention such as aspiration. However, some studies use a 30-day cut-off. A recent Cochrane review concluded that thoracoscopic talc pleurodesis is probably the optimal method for pleurodesis.63 This view is supported by a systematic review.64 Studies are presently underway investigating other agents including the profibrotic cytokine transforming growth factor β.
Tetracycline
Until recently, tetracycline had been the most popular and widely used sclerosing agent in the UK. Unfortunately, parenteral tetracycline is no longer available for this indication in many countries as its production has ceased.65
Sterile talc
Talc (Mg3Si4O10(OH)2) is a trilayered magnesium silicate sheet that is inert and was first used as a sclerosing agent in 1935.66 Talc used for intrapleural administration is asbestos-free and sterilised effectively by dry heat exposure, ethylene oxide and gamma radiation. It may be administered in two ways: at thoracoscopy using an atomiser termed ‘talc poudrage’ or via an intercostal tube in the form of a suspension termed ‘talc slurry’.
Success rates (complete and partial response) for talc slurry range from 81% to 100%.30 54 56 67–70 The majority of studies have used talc slurry alone and only a limited number of comparative studies have been published (see evidence table available on the BTS website at www.brit-thoracic.org.uk). A truncated randomised study by Lynch and colleagues71 compared talc slurry (5 g) with bleomycin (60 000 units) and tetracycline (750 mg). Although the study was terminated early because of the removal of tetracycline from the US market, analysis of the data to that point revealed no differences between the three treatment groups 1 month after pleurodesis. In a randomised trial between talc slurry (5 g) and bleomycin (60 000 units), 90% of the talc group achieved a complete response at 2 weeks compared with 79% of the bleomycin group, which was statistically insignificant.72 Three studies have directly compared talc slurry with talc poudrage (see evidence table available on the BTS website at www.brit-thoracic.org.uk).73–75 For one randomised study the data are available only in abstract form.73 It suggests superiority of poudrage over slurry, but limited data are available to validate this conclusion. Of the other two studies, Stefani et al compared medical thoracoscopy and talc poudrage with talc slurry in a non-randomised way.75 Their results suggest superiority of poudrage over slurry, but the two groups were not equal with respect to performance status. In the largest study, Dresler et al compared a surgical approach to talc poudrage with talc slurry.74 They concluded equivalence, but 44% of patients dropped out of the study before the 30-day end point due to deaths and a requirement of 90% lung re-expansion radiologically after intervention to be included in the analysis.
Three studies have compared talc poudrage with other agents administered via an intercostal tube. One compared bleomycin (see below) and the other two tetracyclines (see evidence table available on the BTS website at www.brit-thoracic.org.uk).76–78 Diacon et al concluded that talc insufflation at medical thoracoscopy was superior to bleomycin instillation on efficacy and cost grounds.76 Kuzdzal et al and Fentiman et al both showed an advantage of talc insufflation over tetracyclines.77 78 Each of the three studies analysed fewer than 40 patients.
Talc slurry is usually well tolerated and pleuritic chest pain and mild fever are the most common side effects observed. A serious complication associated with the use of talc is adult respiratory distress syndrome or acute pneumonitis leading to acute respiratory failure. There have been many reports of pneumonitis associated with talc pleurodesis, although predominantly from the UK and the USA where historically non-graded talc has been used.56 79–87 The mechanism of acute talc pneumonitis is unclear and has been reported with both talc poudrage and slurry. 56 80 This complication is related to the grade of talc used. Maskell and colleagues undertook two studies to determine this association. In the first study they randomised 20 patients to pleurodesis using either mixed talc or tetracycline and compared DTPA clearance in the contralateral lung with that undergoing pleurodesis at 48 h after pleurodesis.88 DTPA clearance half time decreased by more in the talc group, which is a marker of increased lung inflammation. There was also a greater arterial desaturation in those patients exposed to talc. In the second part of the study, graded (particle size >15 μm) and non-graded (50% particle size <15 μm) talc were compared. There was a greater alveolar–arterial oxygen gradient in the group exposed to non-graded talc at 48 h after pleurodesis. In a subsequent cohort study of 558 patients who underwent thoracoscopic pleurodesis using graded talc, there were no episodes of pneumonitis.89
Two studies have investigated the systemic distribution of talc particles in rats after talc pleurodesis. The earlier study using uncalibrated talc found widespread organ deposition of talc particles in the lungs, heart, brain, spleen and kidneys at 48 h. The later study used calibrated talc and found liver and spleen deposition (but no lung deposition) at 72 h, but no evidence of pleurodesis in the treated lungs.90 91 A further study in rabbits found greater systemic distribution of talc with ‘normal’ (small particle talc).92 This supports the evidence from clinical studies that large particle talc is preferable to small particle talc.
Bleomycin
Bleomycin is the most widely used antineoplastic agent for the management of malignant pleural effusions. Its mechanism of action is predominantly as a chemical sclerosant similar to talc and tetracycline. Although 45% of the administered bleomycin is absorbed systemically, it has been shown to cause minimal or no myelosuppression.93 Bleomycin is an effective sclerosant with success rates after a single administration ranging from 58% to 85% with a mean of 61%. No studies have demonstrated superiority over talc.42 71 72 94–102 It has an acceptable side effect profile with fever, chest pain and cough the most common adverse effects.99 102 The recommended dose is 60 000 units mixed in normal saline. Bleomycin has also been used in studies evaluating small-bore intercostal tubes placed under radiological guidance with similar efficacy rates.46 48 49 103 In the USA, bleomycin is a more expensive sclerosant than talc, but this is not the case in Europe where non-proprietary formulations are available.42 72 104
Rotation following pleurodesis
Patient rotation is not necessary after intrapleural instillation of sclerosant. (A)
Rotation of the patient to achieve adequate distribution of the agent over the pleura has been described in many studies. However, rotating the patient is time consuming, inconvenient and uncomfortable. A study using radiolabelled tetracycline showed that tetracycline is dispersed throughout the pleural space within seconds and rotation of the patient did not influence distribution.105 A subsequent randomised trial using tetracycline, minocycline and doxycycline revealed no significant difference in the success rate of the procedure or duration of fluid drainage between the rotation and non-rotation groups.106 A similar study using talc showed no difference in distribution of talc after 1 min or 1 h and no difference in the success rate of pleurodesis at 1 month.107
Clamping and removal of intercostal tube
The intercostal tube should be clamped for 1 h after sclerosant administration. (C)
In the absence of excessive fluid drainage (>250 ml/ day) the intercostal tube should be removed within 24–48 h of sclerosant administration. (C)
Clamping of the intercostal tube following intrapleural administration of the sclerosant should be brief (1 h) to prevent the sclerosant from immediately draining back out of the pleural space, although there are no studies to prove that this is necessary.105 Intercostal tube removal has been recommended when fluid drainage is <150 ml/day, but there is little evidence to support this action.58 68 108 109 In the only randomised study that has addressed the issue, Goodman and Davies randomised patients to 24 h versus 72 h drainage following talc slurry pleurodesis regardless of volume of fluid drainage. They found no difference in pleurodesis success, although they did not reach the recruitment target based upon the power calculation. In the absence of any evidence that protracted drainage is beneficial, and given the discomfort associated with prolonged drainage, we recommend removal of the intercostal tube within 24–48 h after the instillation of the sclerosant, provided the lung remains fully re-expanded and there is satisfactory evacuation of pleural fluid on the chest x-ray.
Pleurodesis failure
The most likely cause of pleurodesis failure is the presence of trapped lung. There is no reliable way to predict pleurodesis failure: a recent systematic review found that an arbitrary cut-off of pH <7.20 did not predict pleurodesis failure.15 Where pleurodesis fails, there is no evidence available as to the most effective secondary procedure. We recommend that further evacuation of pleural fluid should be attempted with either a repeat pleurodesis or insertion of indwelling pleural catheter, depending upon the presence of trapped lung. Surgical pleurectomy has been described as an alternative option for patients with mesothelioma (see later).
Malignant seeding at intercostal tube or port site
Patients with proven or suspected mesothelioma should receive prophylactic radiotherapy to the site of thoracoscopy, surgery or large-bore chest drain insertion, but there is little evidence to support this for pleural aspirations or pleural biopsy. (B)
Local tumour recurrence or seeding following diagnostic and therapeutic pleural aspiration, pleural biopsy, intercostal tube insertion and thoracoscopy is uncommon in non-mesothelioma malignant effusions.110–113 However, in mesothelioma up to 40% of patients may develop malignant seeding at the site of pleural procedures. Three randomised studies have addressed the efficacy of procedure site radiotherapy to prevent tract metastasis (see evidence table available on the BTS website at www.brit-thoracic.org.uk).114–116 Boutin and colleagues114 found that local metastases were prevented in patients who received radiotherapy (21 Gy in three fractions) to the site of thoracoscopy. All the patients received radiotherapy within 2 weeks of thoracoscopy. The incidence of tract metastases in the control group in this study was 40%. This study was followed by a longitudinal study that supported its conclusions.117 In two later studies including sites from a wider range of procedures such as needle biopsy and chest drain, the incidence of tract metastases was not significantly different. Bydder and colleagues showed no benefit of a single 10 Gy radiotherapy fraction to the intervention site in preventing recurrence.116 All the patients received radiotherapy within 15 days of the procedure, but 46% of procedures were fine needle aspirations. O'Rourke and colleagues used the same radiotherapy dose as Boutin but to smaller fields. They found no benefit of radiotherapy, but again included a range of procedures including needle biopsy. The study included 60 patients but only 16 thoracoscopies, 7 in the radiotherapy group and 9 in the best supportive care group. Tract metastases occurred in 4 patients in the best supportive care group (a rate of 44%) and none in the radiotherapy group.115 This is very similar to the incidence of tract metastasis in the study by Boutin et al (40%). The other procedures were pleural biopsies (45%) and chest tubes (25%). A longitudinal study by Agarwal et al found the highest rate of pleural tract metastases in association with thoracoscopy (16%), thoracotomy (24%) and chest tube (9%), but a much lower rate in association with pleural aspiration (3.6%) and image-guided biopsy (4.5%).118 Careful analysis of the available data therefore supports the use of radiotherapy to reduce tract metastasis after significant pleural instrumentation (thoracoscopy, surgery or large-bore chest drain), but not for less invasive procedures such as pleural biopsy or pleural aspiration. A larger study to specifically address this question would be of use.
A cohort of 38 patients described by West et al reported an incidence of pleural tract metastasis after radiotherapy of 5%, but in these cases the metastasis occurred at the edge of the radiotherapy field. Of six patients who received radiotherapy after an indwelling pleural catheter, one subsequently developed pleural tract metastasis.119 There are, at present, insufficient data on which to make a recommendation about the use of radiotherapy in the presence of indwelling pleural catheters.
The role of prophylactic radiotherapy following pleural procedures in non-mesothelioma malignant effusions has not been established and therefore cannot be recommended.
Intrapleural fibrinolytics
Intrapleural instillation of fibrinolytic drugs is recommended for the relief of distressing dyspnoea due to multiloculated malignant effusion resistant to simple drainage. (C)
The use of fibrinolytic agents to ameliorate symptoms related to complex pleural effusions has been described in several studies although there are no randomised controlled trials.
Davies et al found that intrapleural streptokinase increased pleural fluid drainage and led to radiographic improvement and amelioration of symptoms in 10 patients with multiloculated or septated malignant effusions. Intrapleural streptokinase was well tolerated and no allergic or haemorrhagic complications were reported.120 Gilkeson et al121 preferred urokinase in their prospective but non-randomised study. Twenty-two malignant pleural effusions were treated with urokinase resulting in a substantial increase in pleural fluid output in patients both with and without radiographic evidence of loculations. The majority then underwent pleurodesis with doxycycline resulting in a complete response rate of 56%. Similarly, no allergic or haemorrhagic complications were encountered. In the largest series, 48 patients unfit for surgical release of trapped lung after incomplete lung re-expansion following tube drainage were given intrapleural urokinase.122 Breathlessness was improved in 29 patients, 27 of whom eventually successfully achieved pleurodesis. This study compared cases with historical controls treated solely with saline flushes and in whom breathlessness was not assessed.
None of these studies is large enough to accurately describe the safety profile of fibrinolytic drugs in this setting. Immune-mediated or haemorrhagic complications have rarely been described with the administration of intrapleural fibrinolytics in contrast to systemic administration of these agents.123 124 A chest physician should be involved in the care of all patients receiving this treatment.
Thoracoscopy
In patients with good performance status, thoracoscopy is recommended for diagnosis of suspected malignant pleural effusion and for drainage and pleurodesis of a known malignant pleural effusion. (B)
Thoracoscopic talc poudrage should be considered for the control of recurrent malignant pleural effusion. (B)
Thoracoscopy is a safe procedure with low complication rates. (B)
Thoracoscopy (under sedation or general anaesthesia) has grown in popularity as a diagnostic and therapeutic tool for malignant effusions. Under sedation, it is now widely used by respiratory physicians in the diagnosis and management of pleural effusions in patients with good performance status.125–128 Patient selection for thoracoscopy and talc poudrage is important in view of the invasive nature of the procedure and cost.129 A significant benefit of thoracoscopy is the ability to obtain a diagnosis, drain the effusion and perform a pleurodesis during the same procedure.
The diagnostic yield and accuracy of thoracoscopy for malignant effusions is >90%.99 125 127 130 131 Talc poudrage performed during thoracoscopy is an effective method for controlling malignant effusions with a pleurodesis success rate of 77–100%.6 68 97 132–138 Randomised studies have established the superiority of talc poudrage over both bleomycin and tetracyclines (see evidence table available on the BTS website at www.brit-thoracic.org.uk).73 76–78 One large randomised study comparing talc poudrage with talc slurry failed to establish a difference in efficacy between the two techniques.74 A further small non-randomised study comparing these two techniques also established equivalence.133 A large study has established the safety of talc poudrage using large particle talc; no cases of respiratory failure were seen in this cohort of 558 patients.89 Talc poudrage is known particularly to be effective in the presence of effusions due to carcinoma of the breast.139
Thoracoscopy has less to offer in patients with a known malignant pleural effusion and a clearly trapped lung on the chest x-ray. However, under general anaesthesia, reinflation of the lung under thoracoscopic vision will inform whether the lung is indeed trapped and therefore guide the decision to perform talc poudrage or insert a pleural catheter. The procedure can facilitate breaking up of loculations or blood clot in haemorrhagic malignant pleural effusion and can allow the release of adhesions and thereby aid lung re-expansion and apposition of the pleura for talc poudrage.140 141
Thoracoscopy is a safe and well-tolerated procedure with a low perioperative mortality rate (<0.5%).6 126 129 142 The most common major complications are empyema and acute respiratory failure secondary to infection or re-expansion pulmonary oedema, although the latter may be avoided by staged evacuation of pleural fluid and allowing air to replace the fluid.127 129 143
Long-term ambulatory indwelling pleural catheter drainage
Ambulatory indwelling pleural catheters are effective in controlling recurrent and symptomatic malignant effusions in selected patents. (B)
Insertion of a tunnelled pleural catheter is an alternative method for controlling recurrent and symptomatic malignant effusions including patients with trapped lung. Several catheters have been developed for this purpose and the published studies employing them have reported encouraging results.140 144–147 The presence of foreign material (silastic catheter) within the pleural space stimulates an inflammatory reaction, and vacuum drainage bottles connected to the catheter every few days encourage re-expansion and obliteration of the pleural space. Most catheters can be removed after a relatively short period.
In the only randomised and controlled study to date, Putnam and colleagues145 compared a long-term indwelling pleural catheter with doxycycline pleurodesis via a standard intercostal tube. The length of hospitalisation for the indwelling catheter group was significantly shorter (1 day) than that of the doxycycline pleurodesis group (6 days). Spontaneous pleurodesis was achieved in 42 of the 91 patients in the indwelling catheter group. A late failure rate (defined as reaccumulation of pleural fluid after initial successful control) of 13% was reported compared with 21% for the doxycycline pleurodesis group. There was a modest improvement in the quality of life and dyspnoea scores in both groups. The complication rate was higher (14%) in the indwelling catheter group and included local cellulitis (most common) and, rarely, tumour seeding of the catheter tract.
The largest series to date reported on 250 patients, with at least partial symptom control achieved in 88.8%. Spontaneous pleurodesis occurred in 42.9% while catheters remained until death in 45.8%.148 A more recent series of 231 patients treated with an indwelling catheter to drain pleural effusion reported a removal rate of 58% after spontaneous cessation of drainage, with only 3.8% reaccumulation and 2.2% infection.147 This group included those with trapped lung (12.5% of all patients) or who had failed other therapy. A further series of 48 patients reported a spontaneous pleurodesis rate of 48%.149 Pien et al studied a group of 11 patients in whom an indwelling catheter was placed specifically for a malignant effusion in the presence of trapped lung; 10 patients reported symptomatic improvement.144
A recent series of 45 patients reported by Janes et al described three cases of catheter tract metastasis associated with indwelling pleural catheters occurring between 3 weeks and 9 months after insertion. Metastases occurred in 2 of 15 patients with mesothelioma but in only 1 of 30 patients with other metastatic malignancy.150
An indwelling pleural catheter is therefore an effective option for controlling recurrent malignant effusions when length of hospitalisation is to be kept to a minimum (reduced life expectancy) or where patients are known or are suspected to have trapped lung and where expertise and facilities exist for outpatient management of these catheters. Although there is a significant cost associated with the disposable vacuum drainage bottles that connect to indwelling pleural catheters, there may be a cost reduction associated with reduced length of hospital stay or avoidance of hospital admission.
Pleurectomy
Pleurectomy has been described as a treatment for malignant pleural effusions. Open pleurectomy is an invasive procedure with significant morbidity. Complications may include empyema, haemorrhage and cardiorespiratory failure (operative mortality rates of 10–19% have been described).151–153 Pleurectomy performed by video-assisted thoracic surgery has been described in a small series of patients with mesothelioma. There is not sufficient evidence to recommend this as an alternative to pleurodesis or indwelling pleural catheter in recurrent effusions or trapped lung.154
References
Footnotes
Competing interests No member of the Guideline Group is aware of any competing interests.
Provenance and peer review The draft guideline was available for online public consultation (July/August 2009) and presented to the BTS Winter Meeting (December 2009). Feedback was invited from a range of stakeholder institutions (see Introduction). The draft guideline was reviewed by the BTS Standards of Care Committee (September 2009).