Article Text

Abstract
Background The aim of this study was to estimate the long-term (cost-) effectiveness of smoking cessation interventions for patients with chronic obstructive pulmonary disease (COPD).
Methods A systematic review was performed of randomised controlled trials on smoking cessation interventions in patients with COPD reporting 12-month biochemical validated abstinence rates. The different interventions were grouped into four categories: usual care, minimal counselling, intensive counselling and intensive counselling + pharmacotherapy (‘pharmacotherapy’). For each category the average 12-month continuous abstinence rate and intervention costs were estimated. A dynamic population model for COPD was used to project the long-term (cost-) effectiveness (25 years) of 1-year implementation of the interventions for 50% of the patients with COPD who smoked compared with usual care. Uncertainty and one-way sensitivity analyses were performed for variations in the calculation of the abstinence rates, the type of projection, intervention costs and discount rates.
Results Nine studies were selected. The average 12-month continuous abstinence rates were estimated to be 1.4% for usual care, 2.6% for minimal counselling, 6.0% for intensive counselling and 12.3% for pharmacotherapy. Compared with usual care, the costs per quality-adjusted life year (QALY) gained for minimal counselling, intensive counselling and pharmacotherapy were €16 900, €8200 and €2400, respectively. The results were most sensitive to variations in the estimation of the abstinence rates and discount rates.
Conclusion Compared with usual care, intensive counselling and pharmacotherapy resulted in low costs per QALY gained with ratios comparable to results for smoking cessation in the general population. Compared with intensive counselling, pharmacotherapy was cost saving and dominated the other interventions.
- COPD smoking cessation cost-effectiveness model
- COPD epidemiology
- health economist
Statistics from Altmetric.com
Introduction
Smoking cessation is still the most important intervention to slow down the disease progression of chronic obstructive pulmonary disease (COPD).1–3 It decreases the annual decline in lung function,4 reduces symptoms of cough and sputum, improves health status and reduces exacerbations of COPD.5 Because of the strong association between use of healthcare services and disease severity,6 slowing down disease progression is likely to reduce annual COPD-related healthcare costs.
Current treatment guidelines recommend that all patients with COPD who smoke should be offered the most intensive smoking cessation intervention feasible.7 8 A review of five smoking cessation interventions offered to patients with COPD by Wagena et al showed that only pharmacotherapy combined with intensive counselling seemed to be effective in this patient group. The effects of less intensive strategies did not reach statistical significance.9 A more recent review concluded that counselling plus nicotine replacement therapy (NRT) had the greatest effect on prolonged abstinence rates in patients with COPD who smoke.10 Although almost all smoking cessation interventions targeted at smokers in the general population are cost-effective,11 12 little is known about the cost-effectiveness of smoking cessation interventions offered to patients who already have a smoking-related disease like COPD. Since information on the short-term cost-effectiveness of these interventions in COPD is already scarce, information on the long-term cost-effectiveness is virtually absent. It is, however, highly relevant to know the long-term cost-effectiveness because the health benefits are small in the first year after the intervention but will continue to increase over time.
The aim of this study was to estimate the impact of smoking cessation interventions offered to patients with COPD on the future burden of COPD using a previously published dynamic population-based model of COPD disease progression.13
Methods
Study selection
All randomised controlled trials published in English investigating the effectiveness of a smoking cessation intervention in patients with COPD confirmed by spirometry or physician diagnosis were included if the follow-up was at least 12 months. The smoking cessation intervention or therapy had to be the primary intervention and not part of a disease management or education programme and abstinence of smoking had to be biochemically validated.
Search strategy
We performed a literature search in MEDLINE using the following MeSH headings or words in the title or abstract: COPD or ‘chronic obstructive pulmonary disease’ or ‘chronic bronchitis’ in combination with smoking, tobacco, nicotine or smok* or nicotin* and one of the following terms: smoking cessation or tobacco use or quit* or stop* or cessat* or abstin* or abstain*. The search was performed in February 2009 and was limited to randomised controlled trials published in English. We also searched the reference lists of retrieved articles and checked the systematic reviews for further references. If the search in MEDLINE resulted in studies reporting 6-month results, but the authors were aware of other publications in which the 12-month results were presented, the study was included.
Methodological quality
The methodological quality of the selected studies was evaluated using the Jadad scale and the Delphi list.14 15 The Jadad scale consists of five questions with respect to randomisation and blinding. Each positive answer to a question was valued with 1 and a negative answer with 0, resulting in a sum score ranging from 0 to 5.14 The Delphi list consists of nine aspects regarding randomisation, study population, blinding and presentation of results. Possible answers were scored as 1 point (‘yes’) or 0 points (‘no’ or ‘don't know’), resulting in a sum score ranging from 0 to 9.15 Both scores were assigned independently by two reviewers (MH and TF/MRvM). Points of disagreement were discussed until consensus was reached. Both scores were used in combination to assess the methodological quality of the studies.
Combination of abstinence rates and intervention costs
The interventions performed in the different arms of the selected trials were grouped into four categories: (1) care as usual—defined as no counselling or pharmacotherapy or any other type of smoking intervention offered as part of the trial (‘usual care’); (2) minimal or brief counselling <90 min in total (‘minimal counselling’); (3) intensive counselling ≥90 min without pharmacotherapy (‘intensive counselling’); and (4) intensive counselling in combination with any type of pharmacotherapy (‘pharmacotherapy’). Interventions offering pharmacotherapy on a non-compulsory basis were included in the category with pharmacotherapy if this was used by >50% of the patients. Patients in the placebo arms of drug trials often received some form of counselling and were therefore grouped into the categories ‘minimal counselling’ or ‘intensive counselling’ depending on the duration of counselling. For our model calculations we needed absolute quit rates for at least one of the four intervention categories. We therefore used random effect meta-analysis16 to account for study heterogeneity and estimated mean abstinence rates for all four categories. The rates were calculated separately for 12 months continuous abstinence and 12 months point prevalence abstinence; 12 months continuous abstinence was defined as biochemical validated abstinence at all measurements up to 12 months including the 12-month measurement and 12 months point prevalence abstinence was defined as biochemical validated abstinence at 12 months. We recalculated the abstinence rates of the intention-to-treat population assuming subjects with missing data to be smokers when this was not done in the main analysis of the article.
For studies providing sufficient details about the intervention, the costs of the intervention were estimated using Dutch unit costs for the year 2007. Based on these estimates the average intervention costs for all four intervention categories were calculated as the weighted means over the studies using the numbers of patients as weights.
Model
A dynamic population model for COPD was used to estimate the impact of increased implementation of smoking cessation interventions compared with usual care.13 The model is representative for the total Dutch COPD population (306 000 patients in 2000) and is dynamic because changes in the population such as birth, mortality, ageing and changing smoking patterns in the population are taken into account. The model distinguishes six states: no COPD, four COPD severity stages (mild, moderate, severe and very severe COPD based on the GOLD classification8) and dead. The prevalence of COPD for the first year of simulation was distributed over the four COPD severity stages according to the observed severity distribution of physician-diagnosed patients in the Netherlands.17 For each following year the model simulates the changes in the number of patients with COPD, the severity distribution and annual COPD-related healthcare costs due to incidence, mortality and disease progression (ie, annual decline in forced expiratory volume in 1 s (FEV1) percentage predicted). Incidence, mortality and disease progression are specified by gender, age, smoking status and COPD disease severity. COPD-related healthcare costs are specified by gender, age and COPD severity. The most important input parameters of the model are shown in table 1. An extensive description of the model can be found elsewhere13 and is summarised in the online supplement. The model can be used for projections of the Dutch COPD population over time but, more importantly, to evaluate the long-term costs and health benefits of interventions as was done for this study. The effects of smoking cessation were modelled as a one-time increase in FEV1 percentage predicted in the year of smoking cessation followed by a lower annual decline in FEV1 percentage predicted based on the Lung Health Study4 and reduced mortality due to COPD and other smoking-related diseases. The implementation of smoking cessation interventions for patients with COPD was modelled by replacing the smoking cessation rates of usual care by the higher smoking cessation rates of the intervention for a certain period of time for a certain (part of) the COPD population. A higher cessation rate compared with usual care results in more patients with COPD quitting smoking, slower progression to worse COPD severity stages, less mortality and a reduction in COPD-related healthcare costs. The model uses 12-month abstinence rates and accounts for annual probabilities to relapse in former smokers, so former smokers may start smoking again >1 year after quitting.13
Main input parameters of the COPD disease progression model13
Outcome parameters
The long-term effectiveness of the interventions was expressed in terms of the cumulative number of life years and quality-adjusted life years (QALYs) gained and the cumulative reduction in mortality. QALYs were calculated by weighting life years for the quality of life during these years in each COPD severity stage using EQ-5D utility weights (table 1). The cumulative number of life years, QALYs and deaths over the entire time horizon was calculated as the sum of the annual number of patients alive, the annual number of QALYs and the annual number of deaths, respectively, discounting future outcomes. The cumulative COPD-related healthcare costs were calculated as the properly discounted sum of the annual COPD-related healthcare costs over the time horizon. Finally, the cost per (quality-adjusted) life year gained was calculated as the ratio of total intervention costs minus savings in COPD-related healthcare costs compared with usual care divided by the cumulative (quality-adjusted) life years gained compared with usual care.
Base case analysis
In the base case analysis we modelled the impact of offering minimal counselling, intensive counselling or pharmacotherapy to 50% of the Dutch patients with COPD who smoke (76 000 patients) for 1 year compared with usual care; 50% was chosen because this percentage of patients with COPD who smoke reported a willingness to stop smoking within 6 months.19 20 The base case analysis was performed using the mean 12-month continuous abstinence rates as calculated in the meta-analysis. Analyses were performed from a healthcare perspective. Effects and costs were evaluated over a time horizon of 25 years and were discounted at 1.5% and 4%, respectively, as recommended by the Dutch guidelines for pharmacoeconomic evaluations.21
Uncertainty and sensitivity analyses
The uncertainty around the outcomes due to the uncertainty around the calculated abstinence rates and intervention costs was assessed using the 95% lower and upper limits of the difference in the abstinence rate compared with usual care and the minimum and maximum estimates of the intervention costs. Furthermore, a series of one-way sensitivity analyses was performed to estimate the impact of the choice of input parameters on the outcomes. In the first sensitivity analysis the impact of using the 12-month point prevalence rates was assessed. In the second analysis, effects and costs were not discounted. For our base case analyses we used absolute quit rates based on random effect meta-analysis. In the third sensitivity analysis we replaced these by estimating the OR of minimal counselling, intensive counselling and pharmacotherapy versus usual care using a network meta-analysis approach22 and applied these ORs to the average 12-month continuous abstinence rate for usual care. In the fourth sensitivity analysis the model was run for the cohort of Dutch patients with COPD present at the start of the simulations, assuming no new incidence of COPD. In contrast to the Netherlands, in many countries nortriptyline is not considered and/or used for pharmacological smoking cessation support because it is not registered as such. In the fifth sensitivity analysis we therefore estimated the outcomes for pharmacotherapy excluding the studies on nortriptyline.
Results
The literature search identified 39 publications of which 26 were rejected in the first selection based on the title and abstract only. The remaining 13 references were reviewed in full, resulting in the further exclusion of three papers. One reported abstinence rates which were not biochemically validated. The other two studies had a follow-up of 6 months and, to our knowledge, no other publication was available that reported the results at 12 months. Two publications concerned the same study. This resulted in the inclusion of 10 papers reporting nine different studies.2 20 23–30 The characteristics of these studies are shown in table 2.
Characteristics of studies included in the review
The methodological quality of the selected studies is described in the table in the online supplement. The highest scores were observed for studies comparing pharmacological treatments because these studies scored positive on items about ‘double-blinding’. In studies comparing counselling with, for instance, usual care, double-blinding is not feasible so they received a lower quality score. All nine studies were included in the analyses. The table in the online supplement also shows the definitions of abstinence, the method of biochemical validation and the reported abstinence rates for the interventions in the different arms of the nine selected studies. Nineteen different estimates of 12-month continuous abstinence were reported, one estimate for usual care,20 three for minimal counselling,20 23 24 six for intensive counselling24–29 31 and nine for pharmacotherapy (three for NRT, three for bupropion and three for nortriptyline).23–29 31
The weighted average 12-month continuous abstinence rates for intensive counselling (6.0%) and for pharmacotherapy (12.3%) were significantly higher than for usual care (1.4%). This was not the case for minimal counselling with an abstinence rate of 2.6% (table 3). Six studies provided sufficient details to estimate the additional costs of the interventions, minimal counselling (three estimates20 23 24), intensive counselling (five estimates24–27) and pharmacotherapy (eight estimates23–27) compared with usual care. Table 3 shows the weighted average intervention costs as well as the minimum and maximum costs observed within the intervention category.
Combined abstinence rates for the four interventions groups and associated intervention costs
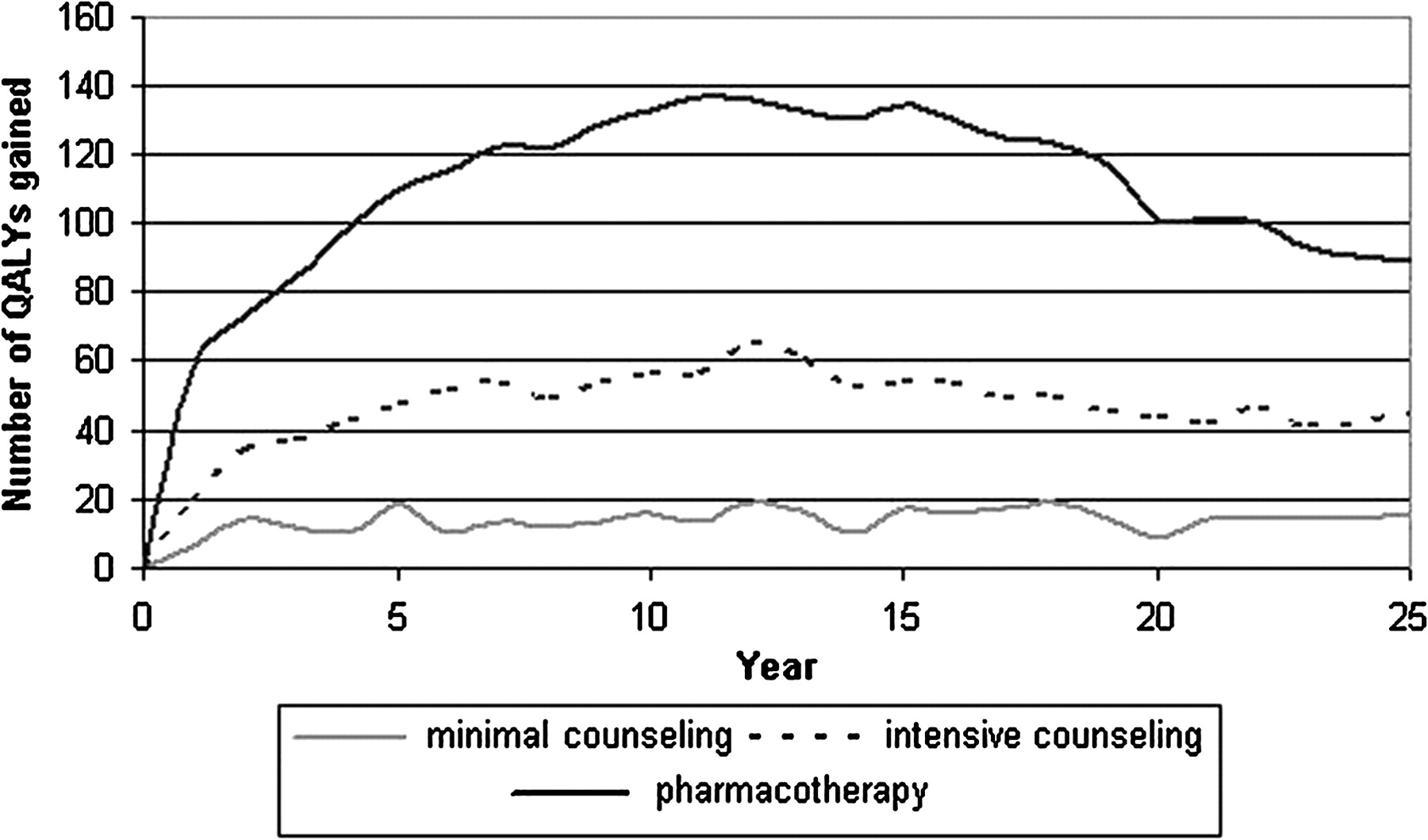
Table 4 shows the results for the base case analysis, 1 year implementation of the intervention for 50% of the patients with COPD who smoked and evaluation of outcomes over a 25-year time horizon. Compared with usual care, the discounted cumulative number of QALYs gained among this group of patients with COPD in the Netherlands was 280 for minimal counselling, 960 for intensive counselling and 2240 for pharmacotherapy. Figure 1 shows the undiscounted number of QALYs gained per year over the 25-year time horizon of the base case analysis. For each of the interventions the maximum gain in QALYs was observed 10–15 years after implementation. Compared with usual care, the net costs (difference in intervention costs minus savings in COPD-related healthcare costs) were €4.8×106 for minimal counselling, €7.9×106 for intensive counselling and €6.3×106 for pharmacotherapy. Estimates of the cost-effectiveness compared with usual care ranged from €2400 for pharmacotherapy to €16 900 per QALY gained for minimal counselling. If each intervention was compared with the next most effective intervention, the cost per QALY of intensive versus minimal counselling was €4600, while pharmacotherapy versus intensive counselling was cost saving.
Results of the base case and sensitivity analyses (€, 2007): 1-year implementation of minimal counselling, intensive counselling or intensive counselling in combination with pharmacotherapy (‘pharmacotherapy’) compared with usual care, time horizon 25 years*

Annual number of quality-adjusted life years (QALYs) gained over time for 1-year implementation of minimal or brief counselling, intensive counselling without pharmacotherapy and intensive counselling with pharmacotherapy (‘pharmacotherapy’) compared with usual care, 0% discounting.
Uncertainty and sensitivity analyses
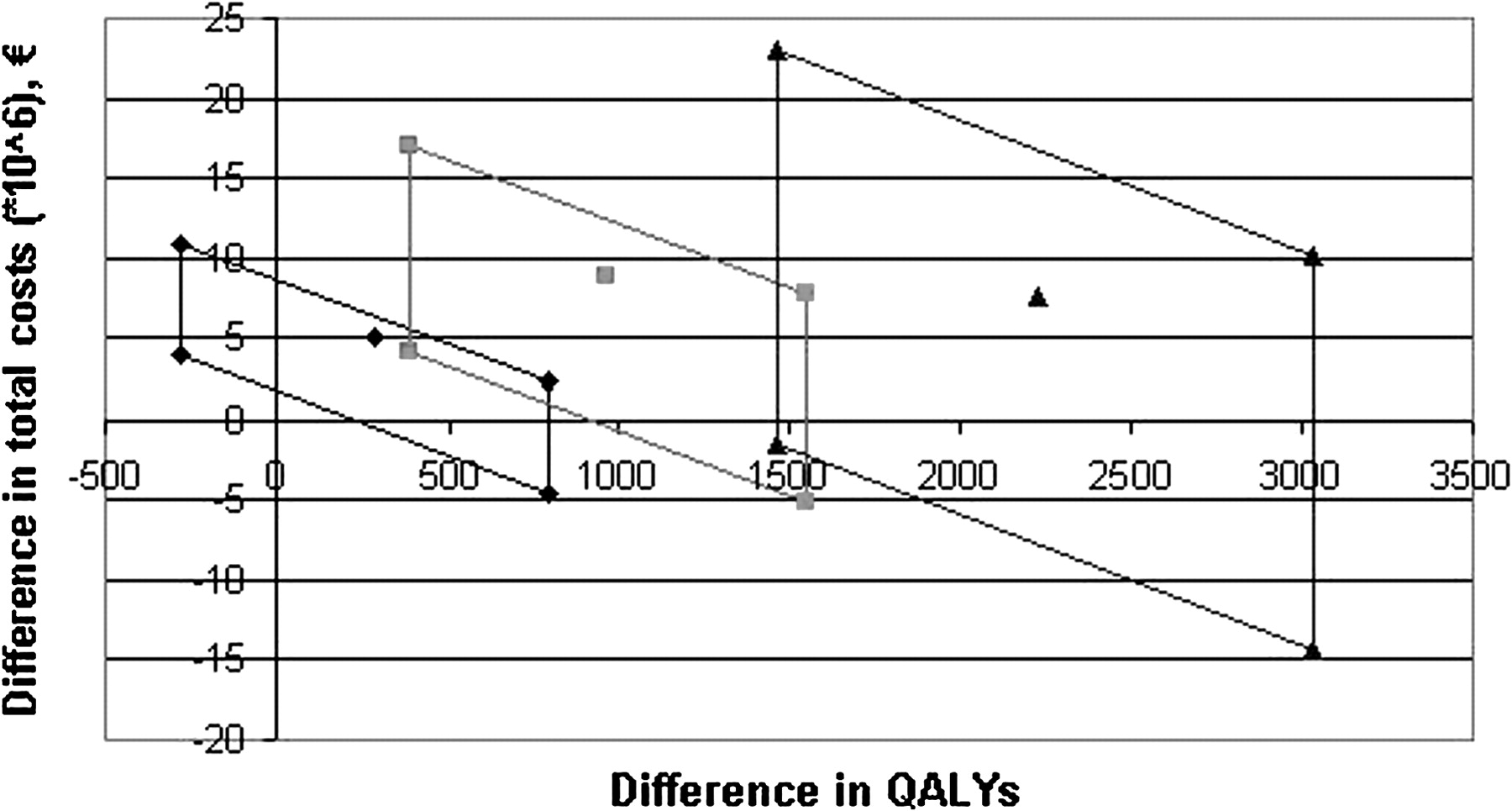
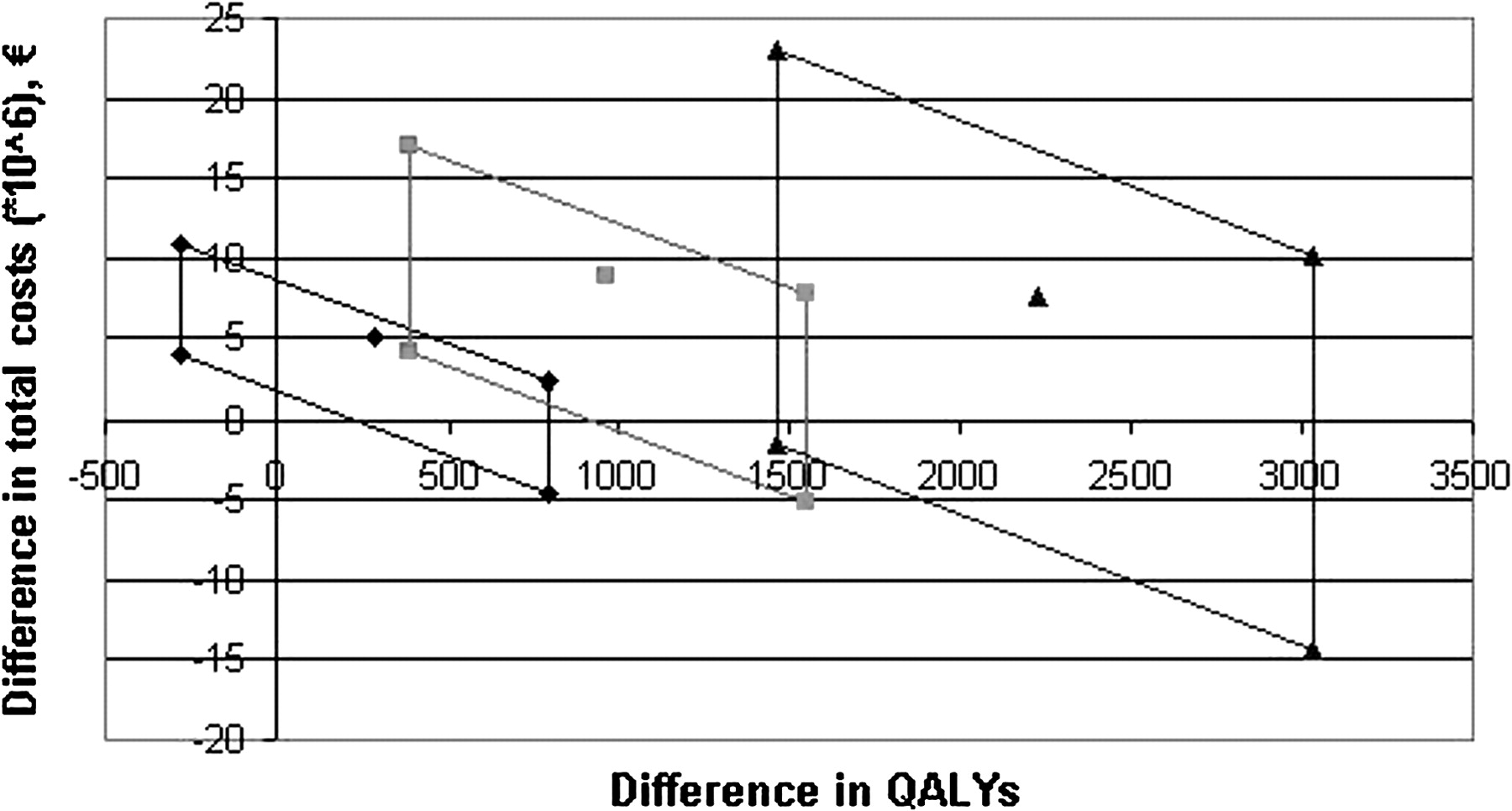
Figure 2 shows the uncertainty around the difference in total costs and the difference in QALYs compared with usual care as a result of the uncertainty around the 12-month continuous abstinence rates and the intervention costs. For minimal counselling the results varied from less effective than usual care with higher costs to more effective with cost savings. The results for intensive counselling ranged from more effective and cost saving to a maximum possible cost per QALY gained of €44 800, while for pharmacotherapy the results ranged from more effective and cost saving to a maximum of €15 700 per QALY gained. The results of the different sensitivity analyses for all interventions compared with usual care are shown in table 4. Using the 12-month point prevalence rates for each of the three types of interventions and usual care resulted in a slightly lower estimate of the cost per QALY gained for minimal counselling and slightly higher estimates for intensive counselling and pharmacotherapy versus usual care compared with the base case analysis. No discounting for both effects and costs also resulted in lower estimates of the cost per QALY gained, with pharmacotherapy even being cost saving. The third sensitivity analysis resulted in ORs of 2.4, 4.7 and 9.8 for minimal counselling, intensive counselling and pharmacotherapy, respectively, compared with usual care. Applying these to the 12-month continuous abstinence rate of usual care (1.4%) resulted in the following abstinence rates of 3.3%, 6.4% and 13.2% for minimal counselling, intensive counselling and pharmcotherapy, respectively. Consequently, the cost-effectiveness of all three interventions was slightly better than the base case analysis. Outcomes based on a cohort of patients with COPD instead of using the dynamic version of the model did not have much influence on the results. The fifth sensitivity analysis based on the 12-month continuous abstinence rate and the weighted average intervention costs excluding the studies on nortriptyline (12.0% and €403, respectively) showed an increase in the cost per QALY for pharmacotherapy compared with usual care from €2400 to €6100.
{kind=link}
{kind=link}
Uncertainty concerning the difference in total costs and the difference in quality-adjusted life years (QALYs) for the base case analysis, 1 year implementation of the intervention compared with usual care over a time horizon of 25 years, discount rate for effects 1.5% and for costs 4%. Diamond, minimal or brief counselling; square, intensive counselling; triangle, intensive counselling plus pharmacotherapy.
Discussion
This study estimated the impact of offering different types of smoking cessation interventions to patients with COPD. Meta-analysis showed that both intensive counselling (defined as >90 min counselling) as well as intensive counselling with any type of pharmacotherapy were significantly more effective than usual care. The cost-effectiveness ratios for both types of intervention were low and below €20 000 per QALY gained, the often used threshold for an intervention to be considered cost-effective in the Netherlands.32 Comparison of pharmacotherapy with intensive counselling resulted in cost savings, making pharmacotherapy the most favourable intervention. The cost per QALY gained for minimal or brief counselling (defined as counselling for <90 min) was also below €20 000, but the effectiveness was not significantly different from usual care.
Our literature search on studies reporting the effectiveness of smoking cessation interventions in patients with COPD resulted in nine studies. It was therefore impossible to group the interventions into more than three or four categories, although we acknowledge that differences in methods and interventions within one category existed. Minimal and intensive counselling are commonly used classifications in smoking cessation studies and reviews. The pharmacotherapy category was too small to subdivide by type, intensity or duration of pharmacotherapy. Longer duration or greater intensity of pharmacotherapy would probably lead to higher abstinence rates, although it is not clear whether this is also true for patients with COPD. With regard to type of pharmacotherapy, the meta-analysis included three estimates on each type of pharmacotherapy (bupropion, nortriptyline and NRT). If, despite the low numbers, the category pharmacotherapy was subdivided into intensive counselling plus NRT and intensive counselling plus antidepressant, the cost per QALY gained would have been €10 400 for NRT and €600 for antidepressants, both low ratios. However, more research on the effectiveness of pharmacotherapies in patients with COPD is needed to give better estimates of the cost-effectiveness specified by type, intensity of supportive counselling and duration of pharmacotherapy. Our estimate of pharmacotherapy included the results of studies offering pharmacotherapy on a non-compulsory basis if this was used by more than 50% of the patients. This might have resulted in a potential underestimation of the effect of pharmacotherapy. Exclusion of the two trials with non-compulsory pharmacotherapy, however, only had a small effect on the incremental cost-effectiveness ratio of pharmacotherapy (€1900 instead of €2400 per QALY gained).
Our estimates of the 12-month continuous abstinence rates of intensive counselling (6.0%) and pharmacotherapy (12.3%) were still relatively low and lower than observed in the general population (10% and 17%, respectively).33 34 These results suggest that abstinence rates in patients with COPD are lower than in ‘healthy’ smokers. This finding was also observed in a study by Wagena et al which showed that patients with COPD had a 30% higher chance of relapsing than smokers at risk of COPD.27 By increasing the intensity and duration of counselling and/or pharmacotherapy, the abstinence rates in COPD may possibly increase, as shown by the Lung Health Study also included in our meta-analysis.2 This study is unique in terms of intensity of the intervention, monitoring of patients and follow-up, which resulted in remarkably high abstinence rates for the smoking intervention group but also for the usual care group. Although the current guidelines advocate the most intensive smoking cessation intervention, it is questionable whether an intervention with such a high intensity as the Lung Health Study is feasible in daily practice.
Results for the cost-effectiveness of pharmacotherapy and intensive counselling in COPD were comparable with the cost per QALY gained for smoking cessation support in the general population. For the general population studies on NRT, bupropion and nortriptyline have shown cost-effectiveness ratios consistently below €10 000 per (quality adjusted) life year.12 35–38 The cost-effectiveness ratio for minimal counselling in COPD is somewhat higher than in studies in the general public.11 12 This is probably a result of the lower abstinence rate and the relatively high intervention costs compared with other studies on minimal counselling. In our study, minimal counselling for patients with COPD consisted of an average of about 25 min counselling while, in most general population studies, minimal counselling is defined as <10 min of cessation advice.
The common approach in reviews evaluating the effectiveness of smoking cessation interventions is to report the RR or OR of one comparator with the other.9 33 34 The best method to retain randomisation would be a network meta-analysis. However, in addition, for a cost-effectiveness analysis the absolute quit rate for at least one of the interventions or usual care needs to be estimated. We decided instead to use the averages of the absolute quit rates as obtained from random effects meta-analysis in our base case analysis. Estimating ORs and applying them to the absolute quit rate of usual care would have resulted in a slightly more favourable cost per QALY estimates for all interventions, but would not have changed the conclusions much (see third sensitivity analysis).
In conclusion, compared with usual care, implementation of intensive counselling with and without pharmacotherapy for patients with COPD resulted in low costs per QALY gained with ratios in the range of results presented for smoking cessation support in the general population. Implementation of minimal counselling was also cost-effective, but the effectiveness was not significantly different from usual care. Pharmacotherapy in combination with intensive counselling was cost saving compared with intensive counselling alone and dominated the other interventions. These results confirm the advice given in the guidelines that patients with COPD should be offered the most intensive smoking cessation intervention feasible, not only from a clinical but also from an economic perspective.
Acknowledgments
The authors acknowledge the help of Maiwenn Al with the statistical analyses.
References
Supplementary materials
Web Only Data thx.2009.131631
Files in this Data Supplement:
Footnotes
Funding This study was financially supported by the Dutch Government (Ministry of Health).
Competing interests MH has participated in smoking cessation research that is financially supported by the pharmaceutical industry. TF is an employee of the Dutch National Institute for Public Health and the Environment and also works on a project granted by the Dutch National Asthma Foundation to develop a simulation model of COPD. MR-vM participates in smoking cessation research that is financially supported by the pharmaceutical industry and also acts as a consultant on smoking cessation issues. RH has no conflicts of interest.
Provenance and peer review Not commissioned; externally peer reviewed.