Article Text

Abstract
Introduction Central airway nitric oxide flux (J'awNO) and peripheral airway/alveolar nitric oxide concentration (CANO) during asthma exacerbation has not been investigated after correction for axial NO back-diffusion.
Methods After measuring exhaled NO (fraction of exhaled nitric oxide (FENO); ppb) at 50, 100, 150 and 200 ml/s, J'awNO (nl/s) and CANO (ppb) were calculated using the two-compartment model and corrected for axial NO back-diffusion. Fifteen (8 males), non-smoking, patients with moderate-to-severe treated (inhaled corticosteroid (ICS) and inhaled long-acting β2-agonist (LABA)) asthma, age 57±13 years (mean±SD), were studied at baseline, during exacerbation prior to oral corticosteroid, and during recovery after an 8 day tapering prednisone course. Based on earlier asthma studies without correction, it was hypothesised that with correction for NO axial back-diffusion, the incidence of abnormal J'awNO and CANO at baseline and after exacerbation would be ≥30% in 15 patients with asthma with 80% power.
Results At baseline when clinically stable, after 180 μg of albuterol, forced expiratory volume in 1 s (FEV1; litres) was 78±26% predicted (p=0.009) with increased FENO at 50 ml/s (p=0.01) and J'awNO (p=0.02), but CANO was normal compared with the controls. During exacerbation FEV1 (litres) was 57±20% predicted (p=0.02), with increased FENO at 50 ml/s (p=0.01) and J'awNO (p=0.004), but CANO was normal. Recovery results were similar to baseline. Two of 15 patients with asthma always had normal exhaled NO gas exchange.
Conclusions The central airways were the major site of abnormal NO flux in 13 of 15 patients with moderate–severe asthma when stable and during exacerbation and could be easily detected with abnormal FENO at 50 ml/s. CANO was normal.
Clinical trial number NCT00576069.
- Asthma
- exhaled nitric oxide
- lung function
- exhaled airway markers
- lung physiology
Statistics from Altmetric.com
Measurement of the fraction of exhaled nitric oxide (FENO; ppb) is a relatively simple, reproducible and non-invasive test for monitoring airway inflammation.1 Increased FENO in asthma is accepted as a surrogate for predominantly eosinophilic-mediated inflammation in central airways and increased response to inhaled corticosteroid (ICS).1–5 The currently accepted method of measuring FENO at a single constant expiratory flow rate, usually 50 ml/s, is incapable of separating out whether the source of increased NO production is the large central airways or the peripheral small airway/alveolar site, or both.6 However, increased FENO predominantly reflects large central airways. Therefore, several investigators have developed newer techniques to discriminate NO gas exchange between large central airways and peripheral smaller airways/alveolar compartments.7–12
Using a two-compartment model developed by Tsoukias and George,11 central airway NO flux and peripheral airway/alveolar concentration can be estimated by measuring FENO at multiple expiratory flows and plotting NO output versus expiratory flow. The slope of the linear regression line between NO output versus flow reflects the peripheral airway/alveolar NO concentration (CANO; ppb), whereas the y-intercept reflects central airway NO flux J'awNO (nl/s).11 We13 14 and others8 12 15–21 using this model11 have previously reported NO gas exchange in central as well as peripheral airway/alveolar sites in those with mild8 12 15 18–21 and moderate–severe8 13 14 16 17 20 clinically stable asthma. However, two groups independently12 22 have also demonstrated, both experimentally and theoretically, axial back-diffusion of NO from proximal to peripheral airway/alveoli, against the direction of exhalation. Furthermore, this may contaminate peripheral airway/alveolar levels, leading to an underestimation of central airway NO flux and an overestimation of peripheral airway/alveolar NO levels. Axial NO back-diffusion has not been previously accounted for in those with asthma with abnormal expiratory airflow limitation.
The current prospective outpatient study evaluated FENO using the two-compartment model before and after correcting for NO axial back-diffusion12 22 in clinically stable, non-smoking, treated patients with asthma with moderate–severe expiratory airflow limitation who were not previously studied. Our goal was to evaluate and partition central airway versus peripheral airway/alveolar sites of NO concentration at baseline, during an ensuing spontaneous asthma exacerbation prior to initiation of oral corticosteroid, and following recovery with oral corticosteroid. This has not been investigated previously. Based on our earlier asthma studies13 14 without correction for axial NO back-diffusion, we hypothesised the incidence of abnormal J'awNO and CANO at baseline and after exacerbation to be >30% in 15 patients with asthma with 80% power after correction for axial NO back-diffusion.
Methods
Patient selection
We recruited adult patients with moderate–severe persistent asthma who were on maintenance combination inhaled corticosteroid (ICS)/inhaled long-acting β2-agonist (LABA), fluticasone propionate 250 μg/salmeterol 50 μg twice a day (F250/S50) (Advair250/50, GlaxoSmithKline, Research Triangle Park, North Carolina, USA) for at least 1 year. Smoking history was <5 pack-years and currently all were non-smokers for at least 5 years. All asthma patients were clinically stable for at least 8 weeks and were monitored in our tertiary referral outpatient clinic for ≥3 years. Their asthma symptoms and spirometry were optimal when compared with clinical and spirometric results obtained over the previous ≥3 years. When needed for acute relief, medical treatment included a short-acting inhaled β2-agonist (albuterol sulphate metered dose inhaler (MDI) or solution) and inhaled antimuscarinic agent ipratropium bromide (Atrovent MDI or solution, Boehringer-Ingelheim Pharmaceuticals, Ridgefield, Connecticut, USA). All those with asthma were off oral corticosteroids, antibiotics and leukotriene-modifying agents for at least 8 weeks before entry into the study. Serum eosinophils and immunoglobulin E (IgE) were measured only at baseline. All subjects with asthma had demonstrated bronchodilator reversibility within the past 2 years defined as an increase in forced expiratory volume in 1 s (FEV1) 200 ml and ≥12%, 15 min after 180 μg of albuterol via MDI. Our goal was to study prospectively exhaled NO gas exchange in the initial 15 patients with moderate–severe asthma who developed an acute exacerbation requiring oral corticosteroids.
Normal controls
Normal values for FENO were obtained from 40 normal subjects (20 males), age 57±9 years (mean±SD), who were asymptomatic, healthy lifelong non-smokers with no history of lung disease and not on any medications. No provocative bronchoconstrictor challenge tests were done on normal subjects. All subjects with asthma and normal subjects studied had given informed consent for participation. This study was approved by both Lakewood Regional Medical Center IRB and Western IRB, Olympia, WA, and registered as NCT00576069.
Measurement of exhaled NO gas exchange
All subjects abstained from food and coffee for 2 h and alcohol for 12 h prior to studies. Exhaled NO was measured in triplicate prior to spirometry at four separate constant expiratory flow rates: 50, 100, 150 and 200 ml/s, and the mean of three values obtained within 10% of each other was reported using a Sievers NOA 280 chemiluminescence analyser with varying expiratory airflow resistors (GE Analytical Instruments, Boulder, Colorado, USA) as previously described.13 14 Furthermore, to avoid nasal NO contamination, a mouth pressure of >5 cm H2O was used, as previously recommended.23 The NO analyser was calibrated daily with a known concentration (45 ppm) and before each patient and control subject with NO-free air. The technique of Tsoukias and George11 was used to calculate central airway NO maximal flux (J'awNO, nl/s) (y-intercept) and steady state peripheral airway/alveolar NO concentration (CANO, ppb) (slope) using a linear regression line for each subject with a minimum of three expiratory flow rate data points and r2 of ≥0.9. Correction was made for potential underestimation of large airway NO flux due to axial back-diffusion of NO using the method of Condorelli et al22 by multiplying large airway NO flux J'awNO by a factor of 1.7. Furthermore, to adjust for possible spurious overestimation of values for peripheral lung CANO, initial uncorrected large airway NO flux J'awNO (nl/s) was divided by a correction factor of 0.53 and subtracted from initial uncorrected small airway/alveolar CANO.22 This could yield negative or near zero values for peripheral lung CANO.22 This correction factor was determined in normal subjects and those with mild asthma using flow rates of 50–250 ml/s.22 Investigators responsible for measuring FENO gas exchange and lung function (CFT, CF and AK) were blinded to the therapeutic intervention. Spirometry and NO gas exchange were measured at the initiation of the study when subjects with asthma were clinically stable at baseline, and subsequently prior to initiation of oral corticosteroid during exacerbation, and then during recovery immediately after treatment with an 8 day course of tapering oral corticosteroid.
Lung CT studies
Our goal was to include only patients with asthma without clinically occult significant lung CT-scored emphysema or bronchiectasis. Therefore, all subjects with asthma had high-resolution, thin-section scans of the lung obtained using a helical 64 slice multidetector-row CT (Model Sensation 64, Siemens, Malvern, Pennsylvania, USA). Images were obtained at 5 mm collimation at intervals of 6 mm using 120 kVp and varying mA dependent upon patient size. Reconstructured 1 mm slices were obtained every 9 mm using a window width of 850 HU and level of −600 HU with an edge-enhancing algorithm. Images were scored by a radiologist (Mark J Schein) as 0 to 100, none to worst emphysema, using picture templates which we previously validated using inflated whole lung specimens.24
Lung function studies
When clinically stable at baseline, and during recovery following treatment with oral corticosteroid, subjects with asthma were instructed to continue all their medications, except to withhold MDI albuterol sulphate and/or ipratropium bromide for 6 h, and the LABA DPI (dry powder inhaler) for 24 h prior to testing. Obviously, during asthma exacerbation, medications were not withheld. Our techniques for measuring spirometry, thoracic gas volumes and airway resistance using plethysmography, and diffusing capacity have been previously published.13 14
Protocol: therapeutic intervention with oral corticosteroid
Once selected for this prospective, single-blind, open label to patient study, patients with asthma were continued on maintenance combination ICS plus inhaled LABA. Concurrent acute relief medications when needed included aerosolised and/or nebulised albuterol sulphate and ipratropium bromide. Definition of asthma exacerbation requiring oral corticosteroids included increasing complaints of cough±sputum, chest tightness, wheezing and shortness of breath for ≥1 day. These symptoms were not relieved despite at least three treatments with aerosolised and/or nebulised 2.5 mg albuterol sulphate and 0.5 mg ipratropium bromide within 8 h and there was a concomitant decrease in FEV1 ≥0.3 litres from baseline. In addition, absence of fever and no acute change on a chest x-ray were required. The decision to initiate oral corticosteroids was determined by the emergency ward or other physician who was initially unaware of the study until the patient with asthma informed the physician, and the Principal Investigator was immediately notified. Asthma exacerbation was treated with an 8 day tapering course of oral prednisone starting with 40 mg. Concurrent use of antibiotics was optional and was used in eight of the subjects with asthma. No laboratory study was initiated to definitively determine the aetiology of superimposed acute bronchitis. Measurement of FENO was not used to guide clinical treatment.
Statistical methods
In our previous studies13 14 we noted that >60% of patients with clinically stable moderate–severe asthma had significantly increased peripheral lung CANO without correction for NO axial back-diffusion22 and, after re-examination, >30% after correction.13 In the current study, we needed to evaluate a minimum of 15 patients with moderate–severe asthma at baseline and during exacerbation to achieve 80% power to detect a ≥30% incidence of increased peripheral CANO after correction for NO axial back-diffusion.22 Forty normal age-matched subjects were compared with patients with asthma at baseline using two-group unpaired t tests. Data for those with asthma were initially analysed to determine normality distribution using Shapiro–Wilks test. Because of non-parametric data, analysis of variance (ANOVA) using ranks with repeated measurement was used, with clinical status including stable baseline, exacerbation and recovery as the within factor. Paired t test was used to compare change in clinical status within the same group. S+version for Windows was used for analysis (Tibco Software. Palo Alto, California, USA). Values for p <0.05 were considered significant.
Results
Baseline studies
We prospectively studied 15 (8 males) patients with moderate–severe asthma, age 57±13 years (mean±SD) who had been treated with inhaled combination ICS+LABA for 3.6±0.4 years. Results of lung function studies in normal subjects and those with asthma before and 15 min after 180 μg of albuterol by MDI are presented in table 1. Those with asthma had baseline vital capacity of 3.0±1.0 litres (87±29% predicted), total lung capacity 5.8±0.9 litres (108±19% predicted), residual volume 2.8±1.0 litres (143±47% predicted), functional residual capacity 3.5±0.9 litres (133±62% predicted), single breath diffusing capacity 23±6 ml/min/mm Hg (98±27% predicted) and diffusing capacity/alveolar volume 5.0±0.8 ml/min/mm Hg/l (126±20% predicted). Compared with 40 age-matched normals, values for forced vital capacity (FVC), FEV! and FEV1/FVC were significantly decreased at baseline. High-resolution, thin-section lung CT emphysema scores25 were 9±5 (mean±SD), indicating none or trivial emphysema, and no bronchiectasis was noted in the 15 subjects with asthma. At baseline, serum IgE was 215±154 mg/dl and total blood eosinophil count 0.42±0.36×109 cells/l in the 15 subjects with asthma.
Lung function and nitrix oxide (NO) gas exchange in normal subjects and patients with asthma at baseline, during exacerbation and following recovery
Baseline NO production
Compared with age-matched normal subjects, when clinically stable, baseline values for FENO at 50 ml/s, ppb (p=0.01), FENO at 100 ml/s, ppb (p=0.005), J'awNO, nl/s (p=0.02) and CANO, ppb (p=0.04) in the subjects with asthma were significantly increased prior to Condorelli correction.22 The value for central airway NO flux J'awNO after correction for axial back-diffusion of NO remained significantly increased (p=0.02). However, after correcting22 for NO axial back-diffusion, values for CANO were zero or slightly negative (not statistically different from zero) both in normal subjects and all those with asthma (p=0.2), indicating no or trivial peripheral airway/alveolar CANO concentration. Two of the 15 subjects with asthma at baseline had normal values for NO gas exchange despite abnormal spirometry (see table 1 and figures 1–5).

Measurement of total exhaled nitric oxide (FENO) at 50 ml/s in age-matched normal subjects and patients with asthma on fluticasone 250 μg/salmeterol 50 μg when stable at baseline, during exacerbation and following recovery. ppb, parts per billion. Each figure notes the median, 1–3 interquartile with 5–95% bars in normal subjects and those with asthma, and asthma outliers are represented by a line.
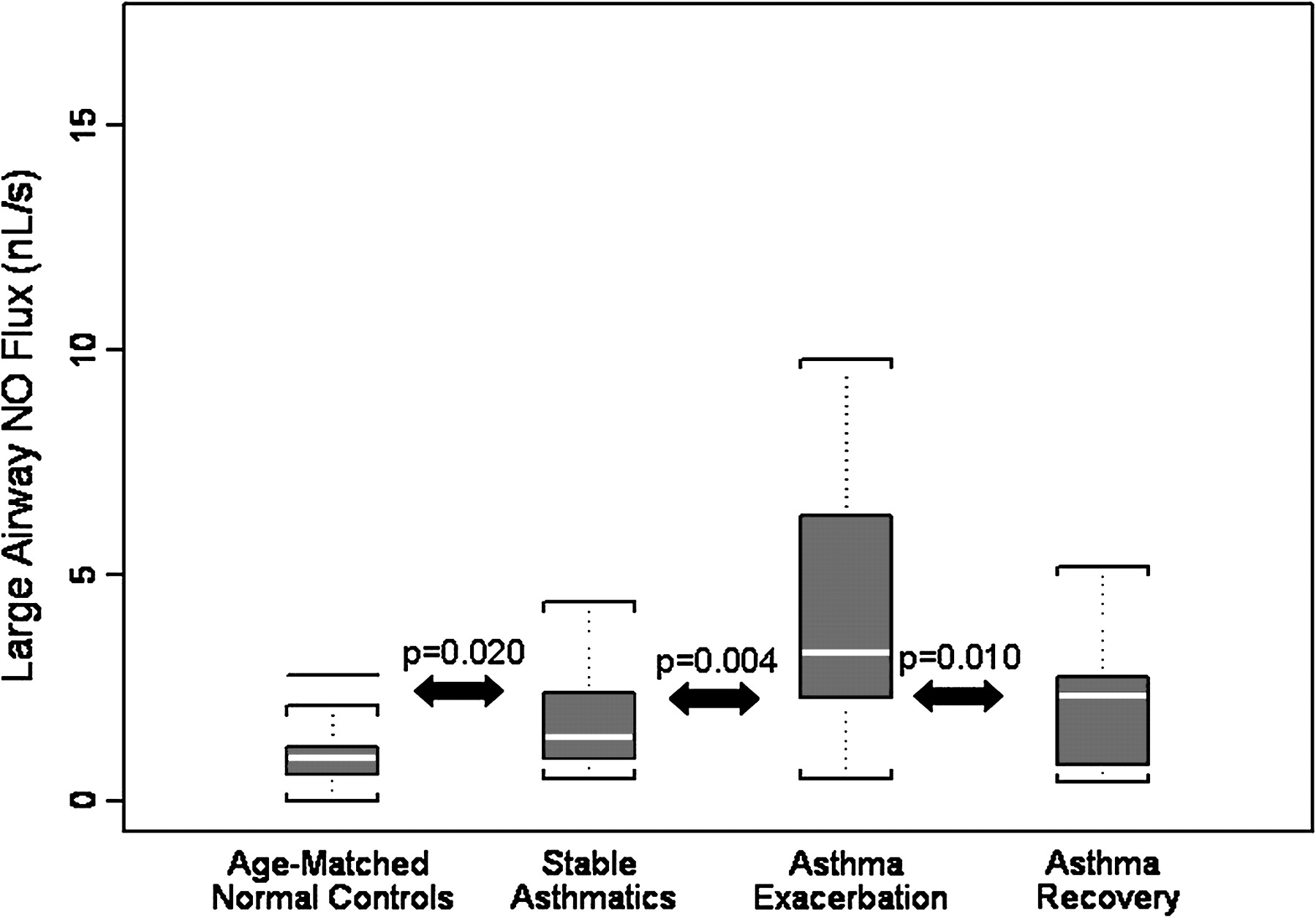
Measurement of large/central airway nitric oxide (NO) flux (nl/s) in age-matched normal subjects and patients with asthma on fluticasone 250 μg/salmeterol 50 μg when stable at baseline, during exacerbation and following recovery. NO values are uncorrected for axial back-diffusion.22
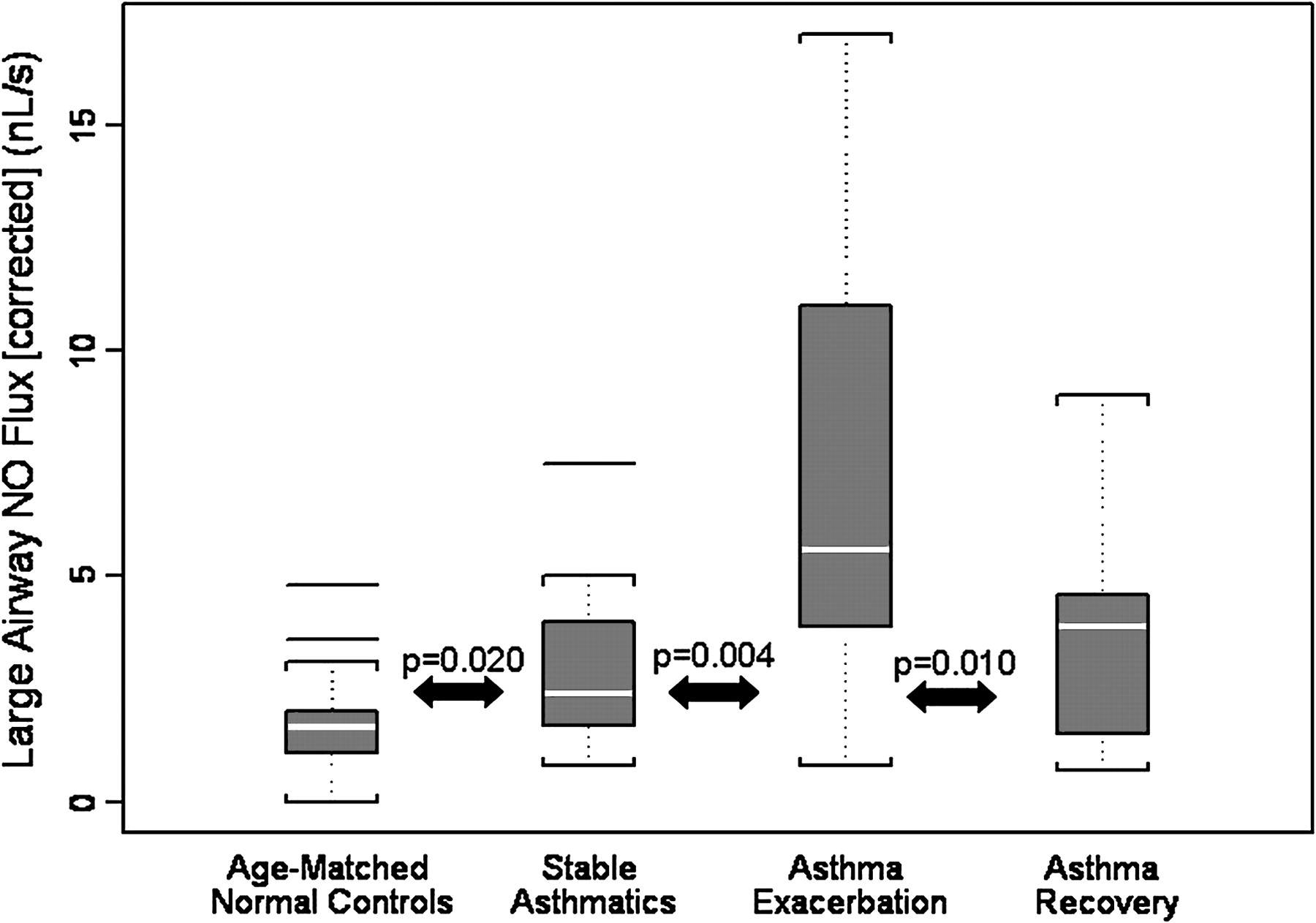
Measurement of large/central airway nitric oxide (NO) flux (nl/s) adjusted for axial NO back-diffusion22 in age-matched normal subjects and patients with asthma on fluticasone 250 μg/salmeterol 50 μg when stable at baseline, during exacerbation and following recovery.

Measurement of small and peripheral airway/alveoli CANO (ppb) in age-matched normals subjects and patients with asthma on fluticasone 250 μg/salmeterol 50 μg when stable at baseline, during exacerbation and following recovery. Nitric oxide (NO) values are uncorrected for axial back-diffusion.22

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Measurement of small and peripheral airway/alveoli CANO (ppb) adjusted for nitric oxide (NO) axial back-diffusion22 in age-matched normal subjects and patients with asthma on fluticasone 250 μg/salmeterol 50 μg when stable at baseline, during exacerbation and following recovery.
Spirometry and NO production during asthma exacerbation prior to initiation of oral corticosteroid
During asthma exacerbation which occurred on average 101±10 days (mean±SD) after baseline, there was a significant decrease in FVC and FEV1 both before and after 180 μg of albuterol. During asthma exacerbation, compared with baseline, there was a significant increase in FENO production at 50 ml/s (p=0.003), at 100 ml/s (p<0.001) and in J'awNO (p=0.004) both before and after correction (p=0.004) for NO axial back-diffusion. There was increased CANO before (p=0.001), but not after (p=0.8) correction for NO axial back-diffusion in all those with asthma. These results allowed us to reject the hypothesis that ≥30% of those with asthma after correction for NO axial back-diffusion would have increased CANO. Two of the subjects with asthma who had normal NO gas exchange at baseline had similar normal values during exacerbation. These two subjects had similar spirometry and serum IgE and total eosinophil count to the other 13 subjects with asthma with abnormal NO gas exchange (see table 1 and figures 1–5).
Spirometry and NO production in recovery after an 8 day oral corticosteroid course
After 10±2 days (mean±SD) following initiation of an 8 day tapering course of oral prednisone, there was a significant increase in spirometry (p≤0.005), compared with values obtained during acute exacerbation. There was also a significant decrease in FENO production at 50 ml/s (p<0.001), at 100 ml/s (p=0.001), J'awNO and CANO compared with values obtained during exacerbation (p=0.01). Results for J'awNO (p=0.01) were unchanged after correction for NO axial back-diffusion. However, CANO was significantly decreased before (p=0.01) but not after (p=0.4) correction for NO axial back-diffusion. The two subjects with asthma who had normal values for NO gas exchange at baseline and despite exacerbation also had normal values during recovery after oral corticosteroid. Their response to oral corticosteroid was similar to that of those with asthma with elevated NO gas exchange (see table 1 and figures 1–5).
Discussion
Spirometry and exhaled NO at multiple expiratory flow rates were measured to determine the contribution of central and peripheral airway/alveolar NO production sites using the two-compartment model.11 Data were obtained initially at baseline, during asthma exacerbation prior to initiating oral corticosteroid, and subsequently during recovery immediately following an 8 day course of tapering oral corticosteroid. At baseline, despite optimal clinical stability, there was significantly abnormal spirometry and both increased central airway NO flux and peripheral airway/alveolar CANO before correction for NO axial back-diffusion.22 However, after correction, peripheral airway/alveolar CANO was normal compared with 40 age-matched healthy, non-smoking controls with normal lung function. During asthma exacerbation, with greater expiratory airflow limitation, central airway NO flux, (J'awNO) was increased before and after correction for NO axial back-diffusion.12 22 However, peripheral airway/alveolar CANO was significantly increased before but not after correction for NO axial back-diffusion.12 22 The results suggest that central airways are the predominant site of increased NO gas exchange in 13 of 15 patients with asthma with moderate–severe expiratory airflow limitation studied at baseline and following exacerbation. Two of the 15 studied patients with asthma had normal values for NO gas exchange at baseline, during exacerbation and following recovery after oral corticosteroid. These two patients may have a non-eosinophilic-mediated inflammatory pathway. However, their clinical and physiological response to 8 day tapering oral corticosteroid treatment was similar to that of the other 13 subjects with asthma, with increased central airway J'awNO flux. Furthermore, measurement of FENO at 50 ml/s, which reflects predominantly large airway NO flux, may be both more relevant and practical, especially when peripheral airway/alveolar NO is normal.
Peripheral airway/alveolar NO production and inhaled corticosteroid
It has been reported that increased central airway NO flux and peripheral lung CANO in asthma reflects predominantly eosinophilic-mediated inflammatory pathways, presumably stimulated by upregulated or overexpressed inducible nitric oxide synthase (iNOS), or less probably constitutive nitric oxide synthase (cNOS).1–6 The present study contradicts in part our previous observations13 14 of increased peripheral lung CANO in 60% of clinically stable patients with moderate–severe asthma that did not take into account axial NO back-diffusion.22 Upon re-examination of our original data,13 14 and after correcting for axial NO back-diffusion,22 peripheral CANO still remained increased in 30% of those with asthma.13 The discrepancy with the present results may in part be related to different cohorts of patients with asthma and the therapeutic regimen. Previous studies uncorrected for axial NO back-diffusion12 22 noted increased central airway NO flux and increased peripheral airway/alveolar CANO in those with clinically stable asthma with mild15 18–21 and moderate–severe obstruction13 14 16 17 despite ICS. Review of published data from van Veen et al16 suggests normal peripheral CANO production after we corrected for NO axial back-diffusion.22 Alternatively, previously published results, also without correction for axial NO back-diffusion,12 22 by Hogman et al,8 Brindicci et al20 and Shin et al,21 reported increased central NO flux but normal peripheral CANO in clinically stable patients with asthmat with mild21 and moderate–severe8 20 expiratory airflow limitation despite ICS. Kerckx and Van Muylem12 noted normal peripheral airway/alveolar NO concentration in those with mild asthma after correction for NO axial back-diffusion. However, Brindicci et al20 reported increased CANO during exacerbation in those with moderate–severe asthma. However, re-examination of their published data20 suggests normal CANO after correction for NO back-diffusion. The reduction in CANO following oral corticosteroid in the present study is similar to our previous experience13 and that of Berry et al17 in those with clinically stable asthma prior to correction for NO axial back-diffusion. We favour the new hypothesis that <30% of those with moderate–severe asthma at baseline and after exacerbation have increased CANO (p<0.001) with a 95% upper confidence limit for incidence of increased CANO of 22%. We would have to study 15 additional subjects with asthma to achieve a 95% upper confidence limit for an incidence of increased CANO<10% (p<0.001).
Potential mechanism(s) for peripheral NO before and after correction for axial NO diffusion
Previously, Silkoff et al5 reported that methacholine-induced bronchoconstriction in subjects with asthma, with reduction in epithelial surface area, decreased NO production by ∼15%. The partial pressure of NO in the small airway and alveolar area (PLNO) is equal to the production of NO by surrounding tissue (VNO)/diffusing capacity of NO from air space into surrounding blood vessels (DLNO).26 Therefore, either an increase in NO tissue production as an inflammatory response (increased iNOS and/or cNOS) or reduced DLNO, or both could account for increased PLNO.26 Lehtimaki et al25 have previously shown an inverse relationship between CANO and pulmonary capillary diffusing capacity in alveolitis. In asthma, we13 14 have previously noted that the increase in CANO was attributed to an increase in NO tissue production, probably related to increased iNOS, and suspect that this is also operant during asthma exacerbation since reduction in DLNO in asthma is unlikely. Furthermore, it would have a relevant effect on NO axial back-diffusion. The increase if any in peripheral lung CANO in clinically stable patients with asthma is modestly downregulated by inhaled compared with systemic corticosteroids.13 14 17
The original two-compartment model developed by Tsoukias and George et al11 to describe central and peripheral airway/alveolar site of NO concentration failed to account for axial back-diffusion of NO from the central airways towards the alveoli. This error may have led to underestimation of central airway NO flux and overestimation of peripheral/alveolar CANO. Subsequent contributions from Condorelli et al22 for NO axial back-diffusion estimated that large airway NO flux is 1.7-fold greater if the flow range is between 50 and 250 ml/s, with trivial NO levels in peripheral lung units in normal subjects (approaching zero). The negligible level of CANO in normal subjects is probably due to the great affinity between periacinar NO and the haemoglobin molecule in the surrounding blood pool.7 11 12 22
Important experimental observations by Kerckx and Van Muylem27 have also demonstrated the inhomogeneous distribution of NO production in healthy adults, with the majority of exhaled NO coming from very proximal airways and ‘larger’ peripheral airways of <17 generation, with little contribution from the lung periphery after correcting for axial NO back-diffusion. The response following histamine-induced bronchoconstriction in normal subjects has been studied by Verbanck et al28 who noted its potential effect to increase convective flow of NO and FeNO at 50 ml/s by a paradoxical decrease in axial back-diffusion of NO. Additionally, Kerckx et al12 reported the inhomogeneous airway contribution of NO production in those with stable asthma without expiratory airflow obstruction and noted a minimal peripheral contribution of NO production, similar to normal subjects, after correcting for axial NO back-diffusion. These observations are similar to those noted by Condorelli et al22 and reinforce the present observations in those with asthma with abnormal expiratory airflow limitation. It is possible that during an acute asthma exacerbation, the correction factor for axial NO back-diffusion would be smaller, due to a smaller cross-sectional area available for back-diffusion of NO through constricted airways. This would result in a potential underestimation of CANO and overestimation of J'awNO using the current technique and interpretation. There are currently no experimental data available on back-diffusion of NO during acute asthma.
Large airway NO flux and ICS, and potential mechanism(s)
Central airway NO flux is the product of NO production in bronchial wall mucosa (Cw) and bronchial NO diffusing capacity (DawNO) which reflects transfer of NO from the airway wall to the lumen of expired air and is proportional to the lumen surface area and transfer coefficient.10 26 While we did not measure Cw and DawNO, this could be estimated as noted by Silkoff et al10 using low exhaled flow rates (5–10 ml/s) and application of a non-linear method. We suspect that in those with both clinically stable and unstable asthma moderate dose ICS (F250/S50) is probably unable significantly to suppress increased bronchoreactive iNOS and/or resident cNOS in the larger airways to reduce bronchial wall (Cw) NO production effectively. Review of the individual data in the present study indicates that 2 of the 15 studied subjects with asthma had normal baseline values for large and small airway/alveolar CANO and without subsequent increase during exacerbation. Despite lack of induced sputum and or airway cellular analyses, this implies a non-eosinophilic inflammatory-mediated pathway29 30 In summary, in the present asthma cohort, and after correction for NO axial back-diffusion, the central airways remain the predominant site of increased NO gas exchange in the subjects with asthma studied at baseline, following exacerbation and subsequent recovery.
Clinical implications
Several investigators2 5 31–36 have addressed the clinical role of add-on monitoring of exhaled NO at a single expiratory airflow rate, usually at 50 ml/s, to help guide inhaled and or systemic corticosteroid dosing in those with clinically stable and unstable asthma, in addition to guideline recommendations which include spirometry.31 Results of five double-blind randomised control trials32–36 comparing add-on FENO versus usual guidelines including spirometry31 were only equivocal. This suggests that routine serial measurements of FENO for clinical asthma management does not appear necessary. However, multiple issues related to study design question the validity of the conclusions.37 The present study is an extension of our original investigation13 14 to define and partition central and peripheral airway/alveolar sites of NO concentration in those with stable asthma at baseline and during exacerbation, initially without13 14 and now with correction for NO axial back-diffusion.12 22 This requires measuring NO gas exchange at four separate expiratory flow rates. However, the current results suggest predominantly central airway sites of abnormal NO gas exchange, presumably reflective of eosinophilic-mediated inflammation, in 13 of the 15 studied subjects with asthma. While measuring FENO at a single expiratory flow rate at 50 ml/s does not provide any information about the contribution of CANO in peripheral sites, it appears that NO overproduction in asthma can be localised to the central airways. Furthermore, it should be emphasised that increased FENO at 50 ml/s, a surrogate of central airway increased NO flux, correlates only modestly with induced sputa eosinophilia >3%: r2=0.26, p<0.001 with a sensitivity of 71% and specificity of 72%,37 and r2=0.29, p=0.007 with tissue eosinophilia in treated subjects with severe refractory asthma.5 The current asthma results are in contrast to our observations in chronic obstructive pulmonary disease where both large airway and peripheral NO are normal, yet large airway NO flux was suppressed with moderate but not low dose ICS.38
Summary
We used the two-compartment NO model11 with correction22 for axial back-diffusion of NO to avoid spurious underestimation of large airway NO flux and overestimation of peripheral CANO. In 13 of 15 the studied clinically stable adult subjects, there was increased NO flux in predominantly central airway sites in those with moderate–severe asthma at baseline with abnormal spirometry despite inhaled corticosteroid. NO production in central airway sites was further increased in the same 13 patients during asthma exacerbation prior to oral corticosteroid and decreased following an 8 day course of tapering oral corticosteroid. This suggests ongoing eosinophilic-mediated inflammation in central airways in these 13 subjects with asthma. Following correction for axial back-diffusion of NO, peripheral airway/alveolar NO values were similar to those of normal subjects. These results are in contrast to our previous observations in other patients with asthma13 14 even after correction for axial NO back-diffusion,22 and suggest that peripheral NO concentration in those with asthma may be normal. Increased measurement of FENO at 50 ml/s may be a practical surrogate for large airway increased NO flux, especially when peripheral lung CANO is normal as in the present asthma exacerbation study.
References
Footnotes
AK, CF, CFT and TM are independent research contractors.
Competing interests PS receives royalties from patents licensed to General Electric Instruments and Aperion, both manufacturers of exhaled NO equipment (range US$2000–US$3000/annum). Consultant to GE Instruments, Aperion and Aperion (range US$10 000–$15 000/annum).
Ethics approval This study was conducted with the approval of the Lakewood Regional Medical Center, Lakewood, California, USA; Western IRB, Olympia, Washington, USA and Registered National Clinical Trials: 00576069.
Provenance and peer review Not commissioned; externally peer reviewed.