Article Text

Abstract
Background and aims Asthma comorbidity, such as depression and obesity, has been associated with greater healthcare use, decreased quality of life and poor asthma control. Treating this comorbidity has been shown to improve asthma outcomes as well as overall health. Despite this, asthma comorbidity remains relatively under-recognised and understudied—perhaps because most asthma occurs in young people who are believed to be healthy and relatively free of comorbidity. The aim of this study was to quantify empirically the amount of comorbidity associated with asthma.
Methods A population-based cohort study was conducted using the health administrative data of the 12 million residents of Ontario, Canada in 2005. A validated health administrative algorithm was used to identify individuals with asthma.
Results The amount of comorbidity among individuals with asthma, as reflected in rates of hospitalisations, emergency department visits and ambulatory care claims, was found to be substantial and much greater than that observed among individuals without asthma. Together, asthma and asthma comorbidity (the extra comorbidity found in individuals with asthma compared with those without asthma) were associated with 6% of all hospitalisations, 9% of all emergency room visits and 6% of all ambulatory care visits that occurred in Ontario.
Conclusions Asthma comorbidity places a significant burden on individuals and the healthcare system and should be considered in the management of asthma. Further research should focus on which types of asthma comorbidity are responsible for the greatest burden and how such comorbidity should be prevented and managed.
- Asthma
- asthma epidemiology
- comorbidity
- epidemiology
- population health
Statistics from Altmetric.com
Introduction
Asthma comorbidity has been associated with increased healthcare use, decreased quality of life and poor asthma control, and evidence suggests that treating it improves asthma outcomes.1–4 Thus, asthma comorbidity prevention and management offers a potentially important approach to improving the overall health of people with asthma and decreasing its burden on the healthcare system.
Despite its potential importance, comorbidity in asthma has been a relatively under-recognised and understudied area, as evident by its comparative lack of attention in the literature and asthma guidelines.5 This is in contrast to other prevalent chronic diseases, such as diabetes and coronary artery disease, where treatment of comorbidities such as renal disease and hypercholesterolaemia is considered very important. This may be because asthma is most prevalent in populations that are assumed to be relatively free of comorbidity such as children and young adults. It may also be because clear pathological links between asthma and potentially associated comorbidity have not been established—like they have been, for example, between diabetes and renal disease. Finally, asthma comorbidity may be under-recognised because its burden on individuals and society has never been well quantified and appreciated.6 Therefore, in order to estimate the amount of asthma comorbidity and its impact on the healthcare system, we conducted a population-based study using health administrative data to measure empirically the amount of comorbidity that occurred in individuals with asthma compared with those without asthma. Thus we were able to estimate the extra comorbidity that accompanied asthma or the amount of ‘asthma comorbidity’ in individuals with asthma. We then used this individual estimate to determine the overall burden of asthma comorbidity on the healthcare system.7
Methods
Study design
A population-based study was conducted using health administrative data.
Setting
Ontario is a province in Canada with a diverse, multicultural population of ∼12 million people. Since universal healthcare insurance is provided to all residents regardless of ability to pay, Ontario health administrative databases contain virtually complete individual-level information on all the health services (including physician visits, emergency department visits and hospitalisations) used by the population. The only exception is the provision of prescription medications, which are only provided to those aged ≥65 years and those who are on welfare.
Data sources
Four Ontario population-based health administrative databases were used to identify individuals with asthma and estimate the amount of comorbidity. The Ontario Health Insurance Plan (OHIP) database contains information on all claims made by Ontario physicians (except for claims from some salaried physicians and for some aboriginal populations, patients in the Armed Forces and patients in penal institutions). The Canadian Institute for Health Information (CIHI) Discharge Abstract Database is a national database that contains discharge information from every acute hospitalisation in Canada since 1991. The CIHI National Ambulatory Care Reporting System (NACRS) contains information on patient visits to emergency departments. Finally, the Ontario Registered Persons Database (RPDB) captures and maintains demographic information, including date of birth and gender, on all individuals living in the province of Ontario regardless of whether or not they had received any medical care. Linkage of the above three databases (which are exclusive of each other) on an individual level with the RPDB (and therefore with each other) was performed through an encrypted version of the unique Ontario health card number given to all Ontario residents. Such linkage allows for access to a complete health service use profile of every resident of Ontario while protecting their confidentiality.
Participants
All Ontario residents in 2005 were included. Those who died or moved out of the province were excluded. Individuals with asthma were identified using the Ontario Asthma Surveillance Information System (OASIS) database which is a validated registry of all Ontario residents identified as having asthma between 1991 and 2005 (the most recent year for which data were available). To generate the database, a previously validated asthma case-definition algorithm based on claims data was used. Details of the validated algorithm have been published elsewhere.8 9 Once entered into the database, patients remained part of the asthma population until they moved out of the province or died. Individuals with asthma were further subdivided into ‘active’ (those who had used health services for asthma in 2005) and ‘less active’ (those who did not use health services for asthma in 2005) groups. Asthma health services claims were identified using the OHIP and International Classification of Disease (ICD) 9th revision code 493 or ICD 10th revision codes J45 and 46. All health services use (ambulatory care, emergency department and hospital) for these individuals in 2005 were used for analysis.
Outcomes
The primary outcome was the amount of comorbidity in individuals with asthma which was compared with the amount of comorbidity in those without asthma. As a direct correlation between amount of comorbidity and health service claims has been previously well validated, the amount of comorbidity was estimated to be the rate of non-asthma health services use per individual per year.10 11 All non-asthma health services use, instead of just claims for comorbidities proven to be associated with asthma, were considered because empiric studies have shown that excess comorbidity associated with asthma can be found in most disease areas.1 12 The rate of extra comorbidity in those with asthma, or ‘asthma comorbidity’, was estimated by subtracting the rate of non-asthma claims in the asthma group from the rate of (‘non-asthma’) claims in the non-asthma group. Thus any comorbid condition could be considered asthma comorbidity as long as it was more commonly found in the asthma group.
The overall burden of asthma comorbidy in Ontario was estimated by determining the proportion of overall healthcare claims associated with it.
Analyses
Normal approximation (z) tests for equivalence were conducted to determine if the study populations were statistically equivalent in terms of demographic characteristics. Socioeconomic status was inferred from neighbourhood income derived from postal codes and census data.13 Rural status (rural vs urban) was determined using postal code and was based on Statistics Canada's definition of rurality.14
Non-asthma ambulatory care, emergency department visit and hospitalisation claim rates were calculated for the active and less active asthma groups, and overall (‘non-asthma’) claim rates were calculated for the non-asthma group for 2005. For ambulatory care claims only one diagnostic code is provided per claim but, since it was possible for multiple claims to occur during one ambulatory care encounter (eg, one claim for a physician visit and another for an immunisation), only one ambulatory care claim per physician per patient per service day was used to avoid overcounting healthcare use. Since the CIHI databases permitted multiple diagnostic codes per hospitalisation, to avoid double counting, if any of the diagnoses were asthma the hospitalisation or emergency department visit was considered to be due to asthma, otherwise it was considered to be due to a non-asthma condition. All rates were calculated per 100 individuals per year, and age and sex standardised to the 2001 Ontario population.15 The 95% CIs were calculated using the γ distribution.16 All analyses were done using SAS 9.1 software.
To estimate the proportion of all healthcare claims in Ontario in 2005 associated with asthma comorbidity, the number of asthma comorbidity claims in 2005 was first calculated by multiplying the asthma comorbidity claim rate (as calculated above) by the number of individuals with asthma and then dividing by 100. This figure was then divided by the total number of healthcare claims made for any cause for any person in the province of Ontario (derived directly from the health administrative data). The total number of claims associated specifically with asthma was determined directly from the health administrative data.
Secondary analysis
In order to determine if asthma comorbidity rates varied in different segments of the population, results were stratified for children (≤15 years) and adults (>15 years), gender, socioeconomic status and rural or urban residence location. All rates were standardised to the 2001 Ontario population.
To explore further what diagnoses asthma comorbidity was comprised of, the approximate proportion of asthma comorbidity claims for respiratory conditions (eg. upper respiratory tract infection, pneumonia, allergic rhinitis) that might precipitate an asthma exacerbation was estimated.
In another secondary analysis, in order to begin to explore what conditions and diseases made up asthma comorbidity, standardised rates of ambulatory care claims in 16 disease areas based on ICD 9th revision chapters were compared between the asthma and non-asthma groups.
Results
Participants
In 2005, there were 1 662 577 individuals (12.8% of the population) who had been diagnosed with asthma and 11 286 149 individuals who had never been diagnosed with asthma in Ontario. Less than 0.3% of the study population died or moved out of the province during the year. Of the individuals with asthma, 436 403 (26.2%) had active asthma and the rest less active asthma. Demographic characteristics of the active asthma, less active asthma and non-asthma populations can been seen in table 1.
Demographic characteristics of the active asthma, less active and non-asthma populations
Amount of comorbidity in individuals with asthma
Individuals with asthma had a higher amount of comorbidity than those without asthma (table 2). Individuals with active asthma had, on average, 1616 (95% CI 1615 to 1618) non-asthma ambulatory claims per 100 individuals per year. This amount was much greater than the 200 (95% CI 199 to 200) asthma claims per 100 individuals per year that they also had. In addition they also had 68.2 (95% CI 68.0 to 68.5) emergency department visits and 25.8 (95% CI 25.6 to 26.0) hospitalisations per 100 individuals for non-asthma conditions. The amount of comorbidity in individuals with less active asthma was less than in those with active asthma but still notably more than in those without asthma (table 2).
Amount of asthma-specific, non-asthma and asthma comorbidity* health services use in individuals with active asthma, less active asthma and without asthma
Additional comorbidity in individuals with asthma
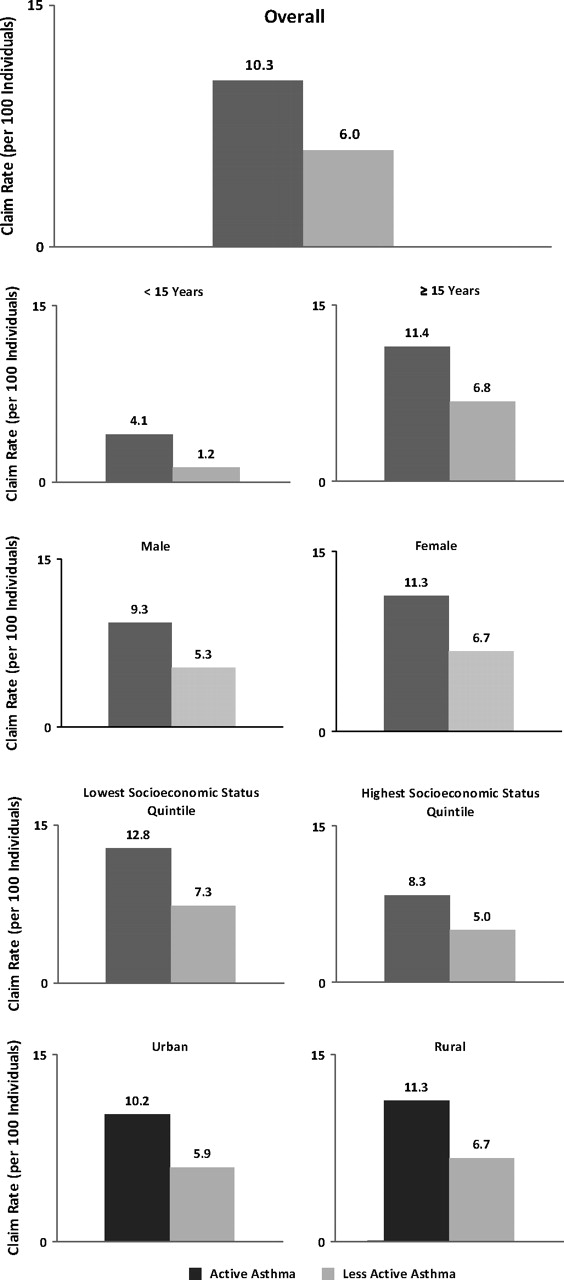
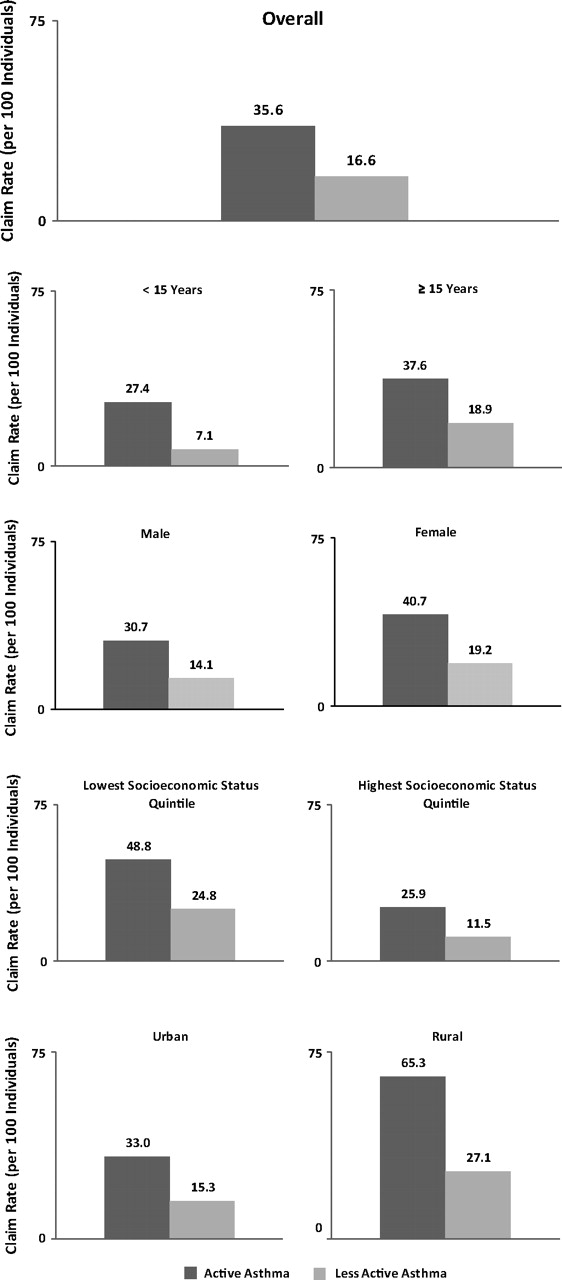
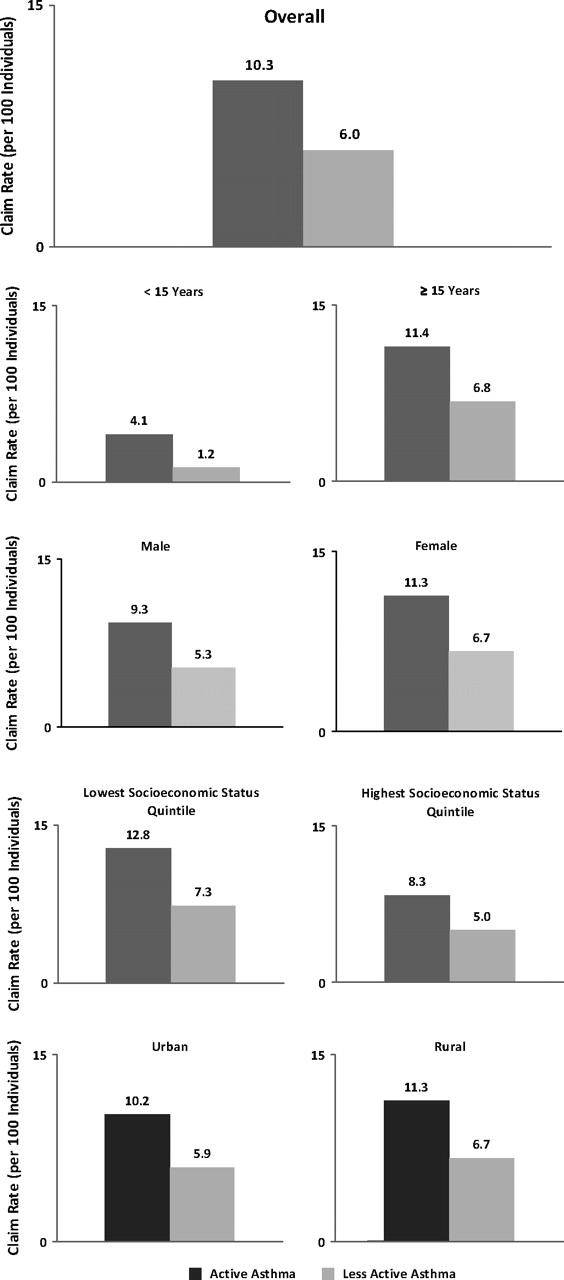
Individuals with asthma had significantly more comorbidity than those without asthma, as seen in table 1. The additional amount of comorbidity, or ‘asthma comorbidity’, in individuals with active asthma accounted for 674, 35.6 and 10.3 ambulatory care claims, emergency department visits and hospitalisations per 100 individuals, respectively (see table 2 and figures 1–3). The asthma comorbidity in individuals with less active asthma was less, accounting for 359, 21.5 and 6.0 ambulatory care claims, emergency department visits and hospitalisations per 100 individuals, respectively (see table 2 and figures 1–3).

Asthma comorbidity ambulatory care claim rates in individuals with active asthma and less active asthma, overall and stratified by age, socioeconomic status and rural or urban residence location.

Asthma comorbidity emergency department visit rates in individuals with active asthma and less active asthma, overall and stratified by age, socioeconomic status and rural or urban residence location.
{kind=link}
{kind=link}
{kind=link}
Asthma comorbidity hospitalisation rates in individuals with active asthma and less active asthma, overall and stratified by age, socioeconomic status and rural or urban residence location.
Proportion of healthcare claims associated with asthma comorbidity
When all the healthcare claims in Ontario in 2005 for any cause and for any person were considered (a total of 131.3 million ambulatory care claims, 4.7 million emergency department visits and 2.2 million hospitalisations), an estimated 5.6% of all ambulatory claims, 7.7% of all emergency department visits and 5.5% of all hospitalisations were found to be associated with asthma comorbidity. When asthma comorbidity claims were added to asthma-specific claims, it accounted for 6.3% of all ambulatory claims, 9.2% of all emergency department visits and 6.3% of all hospitalisations in Ontario.
Secondary analysis
The rate of asthma comorbidity appeared to be substantial regardless of age, gender, socioeconomic status or living in a rural or urban area (figures 1–3).
When claims for asthma comorbidity were examined more closely, it was found that about half were for respiratory conditions (eg, upper respiratory tract infection, pneumonia, allergic rhinitis) that might precipitate an asthma exacerbation.
When standardised ambulatory care claim rates in 16 disease areas based on ICD 10th revision chapters were compared between the asthma and non-asthma groups, much greater comorbidity was found in the asthma group (table 3). The greatest absolute differences in rates were observed for respiratory disease other than asthma, psychiatric disease and musculoskeletal disease.
Age- and sex-standardised ambulatory care claim rates in 16 major disease areas in asthma and non-asthma groups
Discussion
We conducted a population-based study using health administrative data that demonstrated that the amount of comorbidity among individuals with asthma, as reflected in rates of hospitalisations, emergency department visits and ambulatory care claims, was substantial and much greater than (in some cases more than double) the amount among individuals without asthma. Together, asthma and asthma comorbidity (the extra comorbidity found in individuals with asthma) were found to be associated with 6% of the 2.2 million hospitalisations, 9% of the 4.7 million emergency room visits and 6% of the 131.3 million ambulatory care visits in Ontario in 2005. To the best of our knowledge, this is the first large-scale study to measure the burden of asthma and asthma comorbidity and reveal its full impact on individuals and society.17–19
Our findings suggest that, despite asthma being a disease of younger and healthier populations and despite it having few proven causal links with other diseases, asthma comorbidity is common and has a significant impact on individuals and healthcare systems. Our findings can help clinicians appreciate the likelihood that their own patients with asthma suffer from asthma comorbidity and, through its recognition and management, provide them with means to improve their care. On a population level our findings offer an alternative, and probably more accurate, estimate of the burden of asthma on the healthcare system that may be used to conduct effective healthcare planning. Finally, our findings emphasise the importance of asthma comorbidity and the need for more investigation into its pathophysiology and management.
We are not aware of any previous studies that have empirically estimated the amount of comorbidity associated with asthma. There have, however, been studies that have compared certain types of comorbidity in individuals with and without asthma and reported results consistent with our findings. Soriano et al found significantly higher rates of comorbidity in most major organ systems—including respiratory, cardiac, injuries and poisonings, and neurological—in individuals with asthma compared with those without asthma.1 Adams et al found that individuals with asthma were almost twice as likely to report having diabetes, arthritis, heart disease, stroke, cancer and osteoporosis.20 Other studies have demonstrated an association between many different types of comorbidity, such as back problems, obesity and psychosocial stress, and asthma.21–23 Our study builds on these previous findings by empirically quantifying the overall amount of different types of asthma comorbidity combined.
Comorbidity may occur in patients with asthma for several reasons and since our study was descriptive causality could not be determined. First, asthma itself may cause or contribute to comorbidity. For example, asthma control is often suboptimal and the consequent physical activity limitations and disturbed sleep could contribute to depression, osteoporosis and obesity.24 Secondly, treatments for asthma may also cause or contribute to comorbidity. Oral corticosteroids are well known to produce significant adverse effects, but even inhaled corticosteroids may predispose to osteoporosis, increased fracture risk and pneumonia.25–27 Thirdly, some comorbidity such as allergic rhinitis and atopic dermatitis may be linked to asthma via common genetic and environmental factors as part of a larger diathesis. Fourthly, some comorbidities may increase the risk or severity of asthma. This has been well documented for allergic rhinitis and, more controversially, may also be true for gastro-oesophageal reflux and obesity.23 28 29 Fifthly, some comorbidity may represent diagnostic confusion or lack of precision. Codings for ‘bronchitis’ or ‘chronic obstructive pulmonary disease’ in claims data may fall into this category. Future studies exploring the reason for increased comorbidity in individuals with asthma would be important to learn how best to prevent and manage it.
The strengths of this study were its population base, wide generalisability and comparison of individuals with asthma with a non-asthma reference group. Its main limitation was its use of health services as a surrogate marker for comorbidity. While this is a valid association supported by the literature, there are other reasons why individuals with asthma may use health services.10 11 First, use of health services relies on access, and individuals with asthma may have established some form of access for their treatment and therefore may be more likely to use healthcare services than individuals without asthma. In Canada, universal healthcare paid for by the government ensures that lack of money is not a barrier to access; however, other barriers such as lack of time and education may still exist. Secondly, using healthcare may be a learned behaviour, and individuals who have consistent contact with their physician because of their asthma may have learned to use, and perhaps overuse, healthcare resources, while those who have not might be more likely to self-treat. Nonetheless, it seems implausible that the substantial burden of asthma comorbidity seen in the current study would be explained solely by these factors. Future studies investigating the reasons for increased health services use in individuals with asthma would help determine if they are contributors. Finally, even though our health administrative case definition has been validated, some individuals with asthma may have been misclassified as non-asthma, and vice versa. However, any such misclassification would have caused the asthma group and the non-asthma group to be more similar than they actually were. Since our measures of asthma comorbidity were based on the differences between these groups, mixing of these groups would mean our results were an underestimate of the true asthma comorbidity. Likewise, any misclassification between the ‘active’ and ‘less active’ asthma groups would have also led to an underestimate of the true differences between them.
In conclusion, asthma comorbidity appears to be common and have significant impact on individuals with asthma and on the healthcare system. Future study should confirm these findings in clinical populations, determine which conditions are responsible for the greatest burden and explore how prevention and optimisation of asthma comorbidity could decrease the overall burden of disease in the population.
Acknowledgments
The authors gratefully acknowledge Drs Kenneth Chapman MD, University Health Network, Toronto, Ontario, Canada and Matthew Stanbrook MD, University Health Network, Toronto, Ontario, Canada for their helpful comments and suggestions in the drafting of the manuscript.
References
Footnotes
Funding ASG is supported by a Career Scientist Award from the Ontario Ministry of Health and Long Term Care, and was supported by a Research Fellowship from the Canadian Institutes of Health Research, Institute of Population and Public Health and The Public Health Agency of Canada while working on this study. TT is supported by The Dales Award in Medical Research from the University of Toronto, Toronto, Ontario, Canada. Funding for this project was made available through the Canadian Institutes of Health Research (PHE - 85212); Government of Ontario; and the Public Health Agency of Canada who had no role in study design, collection, analysis, interpretation of data, writing of the report or in the decision to submit the report for publication. This study was also supported by the Institute for Clinical Evaluative Sciences (ICES), which is funded by an annual grant from the Ontario Ministry of Health and Long-Term Care. The opinions, results and conclusions reported in this paper are those of the authors and are independent from the funding sources. No endorsement by ICES or any of the funding sources is intended or should be inferred and none had any role in study design, collection, analysis, interpretation of data, writing of the report, or in the decision to submit the report for publication.
Competing interests None.
Ethics approval This study was conducted with the approval of the The Hospital for Sick Children and Sunnybrook Health Sciences Centre, Toronto, Ontario, Canada.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Airwaves