Article Text

Abstract
Background Psychological functioning is an important determinant of health outcomes in chronic lung disease. To better define the role of anxiety in chronic obstructive pulmonary disease (COPD), a study was conducted of the inter-relations between anxiety and COPD in a large cohort of subjects with COPD and a matched control group.
Methods Data were used from the FLOW (Function, Living, Outcomes, and Work) cohort of patients with COPD (n=1202) and matched controls without COPD (n=302). Anxiety was measured using the Anxiety subscale of the Hospital Anxiety and Depression Scale.
Results COPD was associated with a greater risk of anxiety in multivariable analysis (OR 1.85; 95% CI 1.072 to 3.18). Among patients with COPD, anxiety was related to poorer health outcomes including worse submaximal exercise performance (less distance walked during the 6-min walk test: −66.3 feet for anxious vs non-anxious groups; 95% CI −127.3 to −5.36) and a greater risk of self-reported functional limitations (OR 2.41; 95% CI 1.71 to 3.41). Subjects with COPD with anxiety had a higher longitudinal risk of COPD exacerbation in Cox proportional hazards analysis after controlling for covariates (HR 1.39; 95% CI 1.007 to 1.90).
Conclusion COPD is associated with a higher risk of anxiety. Once anxiety develops among patients with COPD, it is related to poorer health outcomes. Further research is needed to determine whether systematic screening and treatment of anxiety in COPD will improve health outcomes and prevent functional decline and disability.
- COPD epidemiology
- COPD exacerbations
- psychology
Statistics from Altmetric.com
Chronic obstructive pulmonary disease (COPD) is an important cause of respiratory symptoms, disability and other poor health outcomes. Recent clinical trials have advanced the treatment of COPD by establishing a beneficial effect of inhaled medications on longer term health outcomes.1–4 Nonetheless, many patients continue to suffer from marked respiratory symptoms and activity limitation despite optimal medical management.
A conundrum of COPD treatment is that patients with a given level of lung function may differ substantively in their symptom burden and activity limitation. Other factors beyond the respiratory system must exert important impacts on clinical outcomes.5 Psychological functioning in particular may influence why two patients with the same degree of lung function impairment have different health outcomes.6
Anxiety is likely to be a problem for many patients with COPD. The symptom of dyspnoea, which is a cardinal manifestation of COPD, can be a potent stimulus for anxiety.7 Inability to perform daily activities or fulfil expected social roles may also lead to anxiety. Cigarette smoking, which is the primary cause of COPD, has also been strongly linked to anxiety symptoms.8 Furthermore, some COPD treatments such as β agonists and theophylline-containing medications may increase symptoms of anxiety and panic.
There remain significant unanswered questions about the prevalence and impact of anxiety among patients with COPD. Although the prevalence of anxiety is probably high in COPD, most studies have not included an adequate control group to estimate the RR.9 A recent workshop conducted by the American College of Chest Physicians concluded that further research was needed to assess the impact of anxiety on health outcomes.9 In particular, the influence of COPD severity on the risk of anxiety has not been adequately characterised. Moreover, the impact of anxiety on the risk of COPD exacerbations is not clear.10
To evaluate these issues, we studied the inter-relations between anxiety and COPD in a large cohort of subjects with COPD and a matched control group. We theorised that COPD increases the risk of anxiety and that, among patients with established disease, greater disease severity increases the likelihood of anxiety which, in turn, leads to poorer health outcomes. The FLOW (Function, Living, Outcomes, and Work) study, which was designed to evaluate the development of disability in COPD, prespecified this analysis of anxiety and COPD.
Methods
The FLOW study of COPD is an ongoing prospective cohort study of adult members of an integrated healthcare delivery system with a physician's diagnosis of COPD and an accompanying matched control group. Recruitment methods have been previously reported in detail (see online supplement).5 6 11 12 We recruited a cohort of 1202 members of the Kaiser Permanente Medical Care Program who had recently been treated for COPD using a validated algorithm based both on healthcare utilisation and pharmacy dispensing for COPD.13 A control group of 302 subjects without COPD matched by age, sex and race to the cohort members were also recruited. At baseline assessment, structured telephone interviews that ascertained sociodemographic characteristics, COPD clinical history and health status were conducted.5 11 12 Research clinic visits included spirometry and other physical assessments.
Measurement of anxiety
We used a concept of anxiety based on the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV) as a state characterised by cognitive features (fearful thoughts, difficulty concentrating), emotional response (apprehension, nervousness), behavioural symptoms (agitated movements, hand wringing, pacing) and physiological arousal (sweating, palpitations, muscle tension).14 Anxiety was measured using the 7-item anxiety subscale of the Hospital Anxiety and Depression Scale, which is a widely used validated instrument designed to detect clinically significant anxiety among patients who attend outpatient medical clinics.15 16 The anxiety scale score ranges from 0 to 21, with higher scores reflecting more severe anxiety. We used the recommended optimal cutting point of 8/9 points to identify subjects with significant anxiety.17 In secondary analysis we also used the suggested score ranges to define moderate (11–14 points) and severe anxiety (15–21 points). The scale has been previously used to measure anxiety in COPD.10 18 19 We have previously reported our findings for depression in COPD.6
Assessment of COPD severity
A combined approach was used to measure COPD severity. We used a disease-specific COPD severity score that we had previously developed and validated for use in epidemiological and outcomes research.20 Based on survey responses, the COPD severity score comprises five overall aspects of COPD severity: respiratory symptoms; systemic corticosteroid use; other COPD medication use; previous hospitalisation or intubation for respiratory disease; and home oxygen use. Each item was weighted based on clinical aspects of the disease and its expected contribution to overall COPD severity. Possible total scores range from 0 to 35, with higher scores reflecting more severe COPD.
We also used the validated BODE index, which is a multimodal measure of disease severity.21 The BODE index is based on the body mass index (B), the degree of airflow obstruction (O) measured by forced expiratory volume in 1 s (FEV1), grade of dyspnoea (D) assessed by the modified Medical Research Council (MRC) dyspnoea scale22 and exercise capacity (E) measured by the 6-min walk test. Each component is assigned a specific index and the total score ranges from 0 to 10 points (higher scores indicate greater severity). The BODE index predicts death and other poor outcomes in COPD.21 23 24 We have reported elsewhere that the BODE and COPD severity instruments provide independent explanatory power in relation to disease status.25 Because we posited that dyspnoea may be an important cause of anxiety, the MRC dyspnoea scale score was also evaluated as a separate measure.
Pulmonary function impairment
To assess respiratory impairment, spirometric measurements were conducted according to American Thoracic Society (ATS) guidelines.26 27 We used the EasyOne Frontline spirometer (ndd Medical Technologies, Chelmsford, Massachusetts, USA), which is known for its reliability, accuracy and durability.28 29 The Easyone spirometer has been used by large-scale multicentre international epidemiological studies of COPD.29 30 Because research clinic examinations were conducted by trained non-medical personnel, we did not administer bronchodilators for study purposes. However, 90% of subjects had taken their own short-acting bronchodilator within 4 h of spirometry or had taken a long-acting bronchodilator earlier in the same day.
Patient-centred health outcomes
At the time of the telephone interview, generic physical health status was measured with the Short Form (SF)-12 Physical Component Summary (PCS) score. The SF-12 is derived from the Medical Outcomes Study SF-36 instrument, which is the most widely used measure of generic health status. Defined from the eight SF-36 subscales by factor analysis, the PCS score reflects an underlying physical dimension of physical health-related quality of life (HRQL).31 Higher scores reflect more favourable health states. We also used the Airways Questionnaire 20 revised (AQ-20R) to measure disease-specific HRQL.32 33 This validated instrument has excellent psychometric properties for assessing HRQL in persons with airway disease including COPD. Higher scores correspond to poorer HRQL.32 34
Submaximal exercise performance was measured using the 6-min walk test which has been widely used in studies of COPD.35 36 We used a standardised flat straight course of 30 m in accordance with ATS guidelines.37 Subjects who routinely used home oxygen or who had a resting oxygen saturation <90% were supplied with supplemental oxygen during the test. Every 2 min the technician used standardised phrases to encourage effort, as recommended by the ATS guidelines. The primary outcome measured was the total distance walked in 6 min.
Self-reported functional limitation was measured using a previously validated approach.38 The scale is comprised of 10 questions that assess the degree of difficulty in multiple domains of basic physical functioning such as pushing, stooping, kneeling, getting up from a standing position, lifting lighter or heavier objects, standing, sitting, standing from a seated position, walking up stairs and walking in the neighbourhood. Subjects who indicate “a lot of difficulty” with one or more functions or not doing a function because they were unable or they were told by a doctor not to do so are defined by this measure as having a self-reported functional limitation.38
Longitudinal COPD outcomes: COPD exacerbations
Emergency department (ED) visits and hospitalisation for COPD were used as proxy measures of severe disease exacerbation. ED visits and hospitalisations were ascertained from Kaiser Permanente computerised healthcare databases that capture complete healthcare utilisation at its facilities. These outcomes were measured from the time of completion of the baseline interviews until the time of data acquisition. The median duration of follow-up was 2.1 years (25th–75th IQR 1.7–2.6 years). During the follow-up period there were 76 hospitalisations and 244 ED visits for COPD.
COPD-related hospitalisation was defined as those with a principal ICD-9 discharge diagnosis code for COPD (491,492, or 496). COPD-related ED visits were identified as those with an ICD-9 code for COPD. A composite outcome for hospital-based care was defined as either an ED visit or hospitalisation for COPD.
Covariates
We selected covariates that may be related to anxiety. These included sociodemographic characteristics such as age, sex, educational attainment and income, which were measured as previously described.5 6 11 12 Cigarette smoking was assessed using questions developed for the National Health Interview Survey.39 Because cardiovascular conditions may be associated with anxiety, we assessed comorbid cardiovascular conditions using survey items modified from the National Health Interview Survey.40 These include a reported physician's diagnosis of coronary artery disease, congestive heart failure and hypertension.
Statistical analysis
Statistical analysis was conducted using SAS software Version 9.1 (SAS Institute Inc). Bivariate analysis was conducted with the t test for continuous variables and χ2 test for dichotomous variables. Multivariable logistic regression analysis was used to examine the impact of COPD on the risk of anxiety compared with controls without COPD after controlling for potential confounders.
In our theoretical model of anxiety and COPD we posit that greater disease severity increases the risk of anxiety which, in turn, leads to poorer health outcomes. Moreover, anxiety may also feed back to increase disease severity and indirectly affect health outcomes. Logistic regression analysis was used to assess the impact of COPD severity on the risk of anxiety. Multivariable analysis was performed to control for the potential confounding effects of age, sex, race, educational attainment, income and smoking history. Continuous predictor variables were scaled by dividing by one-half SD which corresponds approximately with the minimal clinically important difference.41
We then examined the impact of anxiety on patient-centred outcomes using multivariable linear regression for continuous outcome variables (PCS-12 scores, AQ-20R scores and SMWT distance) and logistic regression for binary outcome variables (functional limitations). Cox proportional hazards analysis was used to evaluate the longitudinal relationship between baseline anxiety and the subsequent risk of COPD exacerbation. Schoenfeld residuals were used to evaluate the proportional hazards assumption; no evidence of violation was found.42 Kaplan–Meier curves were also generated to display the risk of COPD exacerbation for subjects with COPD with and without anxiety.
To test for an exposure-response relationship between degree of anxiety and the risk of COPD exacerbation, we defined an ordinal variable based on the total anxiety score (no anxiety=0, mild=1, moderate=2, severe=3). Consequently, the HR is expressed for a one-category increase in anxiety level.
We evaluated the impact of concurrent depression, as measured by the Geriatric Depression Scale Short-Form, on the results for anxiety. The impact of depression on COPD-related health outcomes in the FLOW cohort has been previously reported in detail.6 Substantive depressive symptoms occurred in less than half of the subjects with COPD with anxiety (44%). To examine the effect of depression we repeated the analysis of anxiety and health outcomes (both patient-centred outcomes and longitudinal risk of COPD exacerbations) with inclusion of an interaction term for anxiety and depression (in the respective linear regression and Cox proportional hazards analysis).43 The Wald χ2 test was used to test the statistical significance of interaction terms. There was no statistical evidence for interaction in any case (p>0.20), indicating that depression did not modify the impact of anxiety on health outcomes. Consequently, depression was not further considered in the analysis.
Results
COPD and the risk of anxiety
The unadjusted prevalence of anxiety was higher among those with COPD (15%) than in controls (6%; p<0.0001) (table 1). As shown in table 1, anxiety was associated with several demographic and other personal factors including younger age, female sex, non-white race, lower socioeconomic status and current smoking. The pattern of results was similar for control subjects without COPD, although only age was statistically significant owing to the smaller size of the control group. Figure 1 shows the prevalence of mild, moderate and severe anxiety among those with and without COPD.
Baseline characteristics and anxiety

Prevalence of mild, moderate and severe anxiety in patients with chronic obstructive pulmonary disease (COPD) and controls (referents). The overall prevalence of anxiety is 15% and 6%, respectively, among those with COPD and referents. The bars show the proportion of anxious patients in the mild (8–10 points), moderate (11–14 points), and severe (15–21 points) categories in subjects with COPD (green bars) and referents (blue bars). In each category the likelihood of anxiety was higher in the COPD group (p=0.0001).
COPD was associated with a greater risk of anxiety in both unadjusted (OR 2.64; 95% CI 1.62 to 4.31) and multivariable analysis (OR 1.85; 95% CI 1.072 to 3.18) (table 2). When FEV1 was additionally added to the multivariable model to account for lung function differences among subjects with COPD and controls, COPD remained related to a higher risk of anxiety (OR 2.23; 95% CI 1.26 to 3.96) (data not shown).
Chronic obstructive pulmonary disease (COPD) and the risk of anxiety
COPD severity and risk of anxiety
Higher COPD severity, as measured by the COPD severity score and BODE index, was associated with a greater risk of anxiety among persons with COPD (table 3). A higher degree of dyspnoea was also related to a greater risk of anxiety. Lung function impairment was not clearly related to anxiety (p=0.13).
Disease severity and risk of anxiety among 1202 subjects with COPD
Impact of anxiety on patient-centred health outcomes in COPD
Anxiety was associated with poorer patient-centred outcomes including physical health status and disease-specific HRQL (table 4). It was also related to poorer distance walked during the 6-min walk test (−66.3 feet for anxious vs non-anxious groups; 95% CI −127.3 to −5.36) and a greater risk of self-reported functional limitations (OR 2.41; 95% CI 1.71 to 3.41).
Impact of anxiety on patient-centred outcomes in COPD
Anxiety and the prospective risk of COPD exacerbation
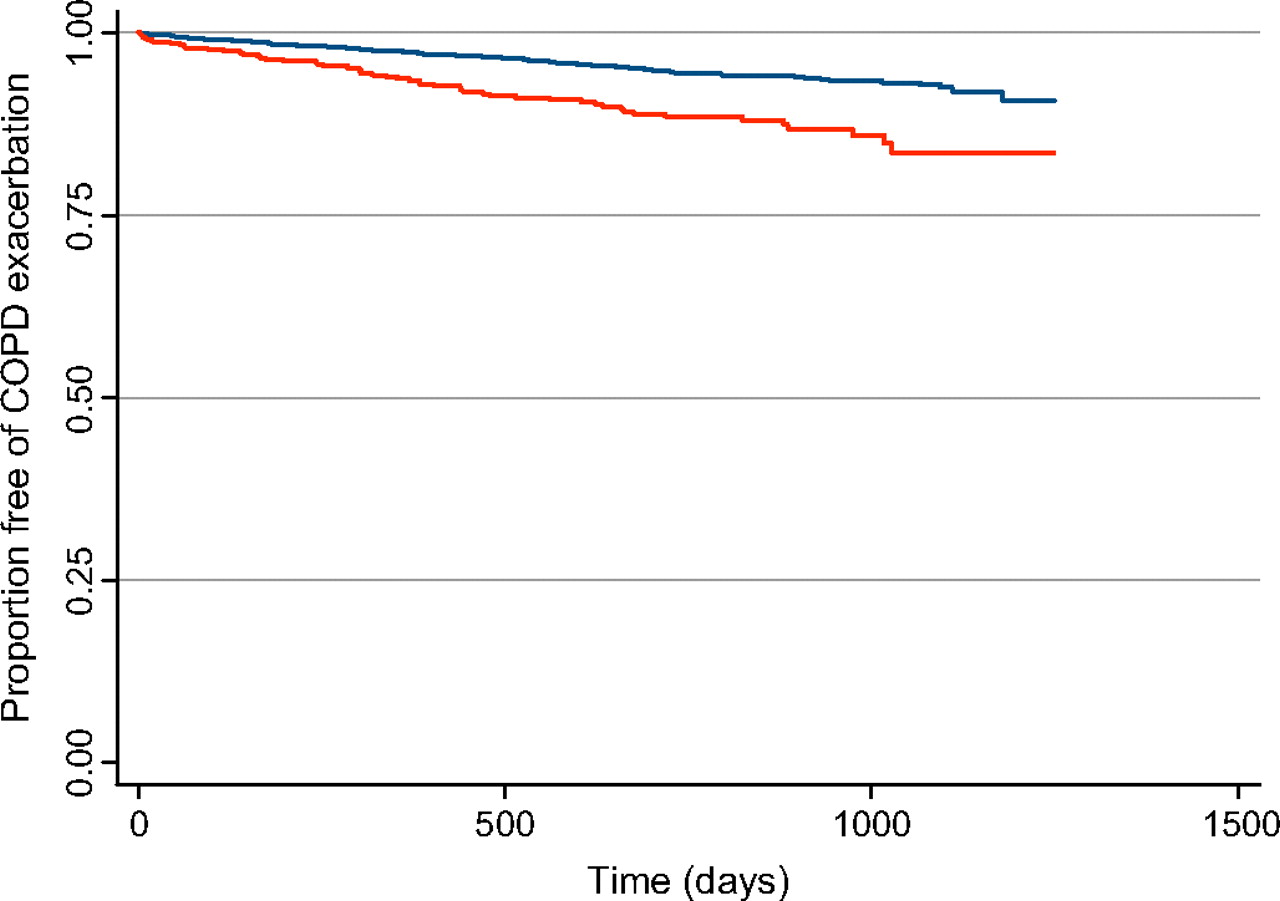
Kaplan–Meier analysis indicated that subjects with COPD with baseline anxiety had a greater risk of COPD exacerbation than those without anxiety (log-rank test, p=0.017, figure 2). Subjects with COPD with baseline anxiety had a higher longitudinal risk of COPD exacerbation in Cox proportional hazards analysis after controlling for covariates (HR 1.39; 95% CI 1.007 to 1.90) (table 5).
Anxiety and longitudinal risk of an exacerbation of chronic obstructive pulmonary disease (COPD)
{kind=link}
{kind=link}
Anxiety and the risk of an exacerbation of chronic obstructive pulmonary disease (COPD) requiring emergency healthcare utilisation. The red line represents subjects with anxiety And the blue line represents subjects without anxiety. p=0.017 (log-rank test) for difference between the two groups.
There was evidence of an exposure-response relationship between severity of anxiety and the risk of COPD exacerbation. For each increment of anxiety category (ie, mild vs none, moderate vs mild, severe vs moderate) the risk of COPD exacerbation increased (HR 1.27; 95% CI 1.09 to 1.49). The overall p value for exposure-response trend was 0.0025.
Anxiety and COPD-related outcomes: COPD severity as a potential mediator
To examine whether the impact of anxiety on COPD-related health outcomes was mediated by COPD severity, we repeated the multivariable analyses after adding the COPD severity score and BODE index as disease-specific severity measures (table 6). The impact of anxiety on distance walked in 6 min and the risk of COPD exacerbations appeared to be mediated completely by COPD severity in that the effect estimates decreased markedly and became statistically non-significant. The association between anxiety and physical health status, disease-specific quality of life and risk of self-reported physical limitations was partly, but not completely, mediated by COPD severity (ie, effect estimates were reduced but not eliminated).
Anxiety and COPD-related health outcomes: potential mediation by disease severity
Discussion
Study findings and integration with previous literature
COPD was associated with a higher risk of anxiety than a matched control group without the condition. Among a large cohort of patients with COPD, disease severity—as measured by the COPD severity score and BODE index—increased the risk of anxiety. Dyspnoea in particular had the strongest association with the risk of anxiety. Anxiety, in turn, had a negative impact on the patient-centred outcomes of physical health status, disease-specific HRQL, submaximal exercise performance and functional limitations. It also increased the prospective risk of COPD exacerbations requiring hospital-based care. The relation between anxiety and COPD-related health outcomes was mediated by COPD severity for some outcomes (submaximal exercise performance and COPD exacerbation) and partially mediated for others (physical health status, disease-specific HRQL and self-reported functional limitations). Thus COPD appears to increase the likelihood of anxiety, especially as the disease becomes more severe; once established, anxiety exerts a negative impact on health outcomes.
Several studies have found a high prevalence of anxiety among persons with COPD.9 44 These estimates have been limited by small sample size, inclusion of patients with advanced or end-stage disease and the lack of a control group. This study advances the field by establishing that COPD is associated with a higher risk of anxiety compared with a matched control group in a large number of patients with a broad range of disease severity.
Although COPD severity increased the risk of anxiety, there was no clear impact of physiological impairment of lung function. This observation extends those from a small study of 122 patients with COPD in which the BODE index, and not the GOLD stage based on lung function, was related to anxiety.18 A larger Nordic study also found no relationship between GOLD stage and anxiety among patients with severe COPD.45 Our findings reinforce the concept that a comprehensive measure of disease severity, and not just physiological impairment, is required to study the impact of psychosocial factors in COPD.
Our analysis clarifies the impact of anxiety on COPD exacerbation. Although depression has been established as a risk factor for COPD exacerbation, the role of anxiety has been less clear.6 10 46 47 In the FLOW cohort study, which has more statistical power than previous investigations, anxiety was a prospective risk factor for COPD exacerbation requiring emergency healthcare utilisation. This effect was, however, entirely explained by the impact of anxiety on greater COPD severity.
Anxiety has a broad negative impact on patient-centred health outcomes in COPD. We theorise that the cognitive aspects of anxiety (which include concentration difficulty and fearful thoughts) will have a major impact on HRQL and exacerbations whereas the symptoms of physiological arousal such as sweating and muscle tension may greatly affect physical health status, exercise performance and functional limitations. We expect the emotional and behavioural correlates of anxiety to have a more global impact on health outcomes. Future work is needed to parse out these specific effects of anxiety on health outcomes.
Implications for treatment of COPD
The mediation analysis has implications for treatment. For some health outcomes (submaximal exercise capacity and COPD exacerbation), the impact of anxiety appeared to be mediated entirely by COPD severity. In our theoretical framework, higher levels of anxiety lead to increased COPD severity which, in turn, adversely affects health outcomes. Consequently, comprehensive treatment of COPD with the aim of decreasing its severity should be the initial goal to improve exercise performance and reduce exacerbations. If response to treatment is partial or inadequate, then treatment of anxiety may be indicated. For physical health status, disease-specific HRQL and functional limitations, treatment of anxiety may improve outcomes even after maximising treatments aimed at reducing COPD severity.
Study limitations
Our study has several limitations. Although we used a reliable and valid measure of anxiety, it is not a clinical diagnosis of generalised anxiety disorder or any other specific DSM-IV diagnosis. We were also not able to evaluate change in anxiety over time. In addition, there is some possibility of misclassification of COPD, although we took rigorous steps to avoid this. The inclusion criteria required a physician diagnosis of COPD, healthcare utilisation for COPD and dispensing of COPD medications, which was designed to increase the accuracy of case ascertainment. We have previously demonstrated the validity of our approach using medical record review.13 Nonetheless, we acknowledge this potential limitation.
In addition, we acknowledge that the causal pathway between anxiety and COPD is complex. We theorised that the most important pathway is that worse COPD symptoms and disease severity increase the risk of anxiety which then leads to poorer health outcomes; anxiety also feeds back to increase disease severity and affect health outcomes. Alternatively, it is possible that the primary mechanism could be anxiety increasing disease severity and, consequently, poorer health outcomes. COPD exacerbations may also mimic anxiety which further increases the complexity. Our results must be interpreted in light of the theoretical framework upon which they are based.
Conclusions
COPD is associated with a higher risk of anxiety; once anxiety develops, it is related to poorer health outcomes, some of which are mediated by disease severity. Further research is needed to determine whether systematic screening and treatment of anxiety in COPD will improve health outcomes and prevent functional decline and disability.
References
Footnotes
Funding National Heart, Lung, and Blood Institute/National Institutes of Health R01HL077618 and K24 HL 097245. Other funders: NIH.
Competing interests None.
Ethics approval The study was approved by the University of California, San Francisco Committee on Human Research and the Kaiser Foundation Research Institute's institutional review board and all participants provided written informed consent.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Airwaves