Article Text

Abstract
Background In patients with chronic obstructive pulmonary disease (COPD), interval exercise has gained recent attention as a possible means of achieving greater physiological training effects compared with continuous exercise. The primary aim of this systematic review was to compare the effects of interval versus continuous training on peak oxygen uptake, peak power, 6 minute walk test (6MWT) distance and health-related quality of life in individuals with COPD.
Methods Randomised controlled trials comparing the effects of interval versus continuous training in patients with COPD were identified after searches of six databases and reference lists of appropriate studies in May 2009. Two reviewers independently assessed study quality. Weighted mean differences (WMD) with 95% CIs were calculated using a random effects model for measures of exercise capacity and health-related quality of life.
Results: Eight randomised controlled trials, with a total of 388 patients with COPD, met the inclusion criteria. No significant differences were found for peak power (WMD 1 W, 95% CI −1 to 3) or peak oxygen uptake (WMD −0.04 l/min, 95% CI −0.13 to 0.05) between interval and continuous training. The WMD for the Chronic Respiratory Questionnaire dyspnoea score was −0.2 units (95% CI −0.5 to 0.0). There was no difference in 6MWT distance between groups (WMD 4 m, 95% CI −15 to 23).
Conclusions Interval and continuous training modalities did not differ in their effect on measures of exercise capacity or health-related quality of life. Interval training may be considered as an alternative to continuous training in patients with varying degrees of COPD severity.
- Chronic obstructive pulmonary disease
- continuous training
- endurance training
- interval training
- rehabilitation
- emphysema
- pulmonary rehabilitation
- exercise
Statistics from Altmetric.com
- Chronic obstructive pulmonary disease
- continuous training
- endurance training
- interval training
- rehabilitation
- emphysema
- pulmonary rehabilitation
- exercise
Introduction
Chronic obstructive pulmonary disease (COPD) is one of the most common causes of death worldwide and is projected to rank third in 2020 in global burden of disease.1 The natural course of COPD is that of progressive airflow limitation, repeated exacerbations, respiratory failure and premature death. In addition to the primary pulmonary pathology, individuals with COPD develop secondary systemic manifestations of the disease including respiratory and peripheral muscle dysfunction, weight loss, osteoporosis, anxiety and depression. These extrapulmonary effects have a significant impact on the quality of life, symptoms and mortality in individuals with COPD.2
There is strong evidence that pulmonary rehabilitation increases exercise tolerance, reduces symptoms and improves health-related quality of life in patients with COPD.3 Although pulmonary rehabilitation includes education, nutritional, social and psychological support, the physical exercise component is considered the cornerstone of rehabilitation.4 While higher intensity training results in greater gains in exercise capacity compared with lower intensity exercise,5 many patients with COPD are unable to sustain a high intensity load for the targeted training duration due to intolerable symptoms.6 7 Therefore, there is increasing interest in strategies, such as interval training, that may provide a tolerable training load while maintaining an effective stimulus for adaptation.8–16
Interval training protocols of repeated bouts of high intensity exercise interspersed with recovery periods have long been demonstrated to be helpful for improving endurance performance and corresponding physiological variables in recreational and elite individuals.17 18 Interval training has also gained recent attention in individuals with chronic heart failure as it has been suggested to produce more favourable cardiovascular effects compared with traditional continuous exercise in these patients.19
In individuals with COPD, it is proposed that interval exercise may increase the tolerance for high intensity work through recovery periods that facilitate a decrease in end expiratory lung volume as well as a reduction in metabolic products from the working muscle that stimulate ventilation.12 14 Several small randomised controlled trials (RCTs) have been conducted in an attempt to determine the most effective training modality for patients with COPD; however, results have been inconclusive.8–11 13 15 16 20 Therefore, the primary aim of this systematic review was to compare the effects of interval versus continuous training on peak oxygen uptake (VO2peak), peak power (Ppeak), 6 minute walk test (6MWT) distance and health-related quality of life in individuals with COPD.
Methods
Search strategy
Study identification began with electronic searching of computerised databases (MEDLINE, PubMed, EMBASE, CINAHL, PEDro and Cochrane) from inception until May, 2009. The Medical Subject Headings used in the search were: “pulmonary disease”, “chronic obstructive”, “lung”, “exercise” and “rehabilitation”. Key terms for the search included “interval/intermittent training”, “continuous training”, “COPD/obstructive lung disease” and “pulmonary/respiratory rehabilitation”. Secondary searches included hand searching reference lists of all identified studies, key author searches and use of the PubMed “related articles” function. Corresponding authors of included RCTs were contacted for missing data where necessary. All authors who were contacted responded.
Inclusion criteria
One member of the research team (MB) performed the search and two members (MB and DB) assessed the studies. Only randomised trials comparing interval with continuous exercise training using standardised protocols (cycle or treadmill at measurable exercise intensity) were considered for inclusion. More than 90% of study participants must have been diagnosed with COPD defined as: (1) a clinical diagnosis of COPD; and (2) one of the following (a) best recorded forced expiratory volume in 1 s (FEV1)/forced vital capacity (FVC) ratio <0.70 or (b) best recorded FEV1 of <80% predicted.21 We considered the following outcome measures: Ppeak and VO2peak measured during an incremental exercise test on a cycle ergometer or treadmill; endurance time measured from a constant power test; functional exercise capacity measured by 6MWT or 12MWT; health-related quality of life as measured by the Chronic Respiratory Questionnaire (CRQ); and anxiety and depression measured by the Hospital Anxiety and Depression scale (HAD). In addition, we extracted data on physiological parameters documenting training effects (lactate threshold, isotime ventilation, heart rate, breathing frequency and symptoms), skeletal muscle adaptations and tolerance to training (eg, compliance, adverse effects). The search identified studies of all languages.
Specific exclusion criteria comprised: (1) not an intervention study with an appropriate comparison group; and (2) only an abstract available with no further information from authors.
Quality assessment
Two members of the review team (MB and DB) independently assessed the internal validity of the studies. The quality assessment was rated according to a 0–5 scale suggested by Jadad22 including items related to randomisation, blinding and withdrawals.
Each trial was also given a score on a 10-point scale using the Physiotherapy Evidence Base Database (PEDro) scale.23 The PEDro assesses quality criteria related to blinding, randomisation, withdrawals, comparability of baseline characteristics and data reporting.
Statistical analysis
Trial data were combined using Review Manager 5.0 (Cochrane Collaboration's Information Management System), with all outcome measures treated as continuous variables. The weighted mean difference (WMD) was selected when estimating the total effect of combined data. The random effects model was used for all analyses, and forest plots were used to depict the results visually. The change due to continuous training was subtracted from the change due to interval training for each outcome; therefore, a positive WMD indicated that the effect for interval training was greater than for continuous training. Heterogeneity was tested with the I2 statistic.
Point estimates and confidence limits for the difference between groups were assessed to see if they exceeded the minimal important difference. We chose 0.5 as the minimal important difference for the CRQ domains of dyspnoea and total score,24 and 54 m for the 6MWT.25
Results
Search results
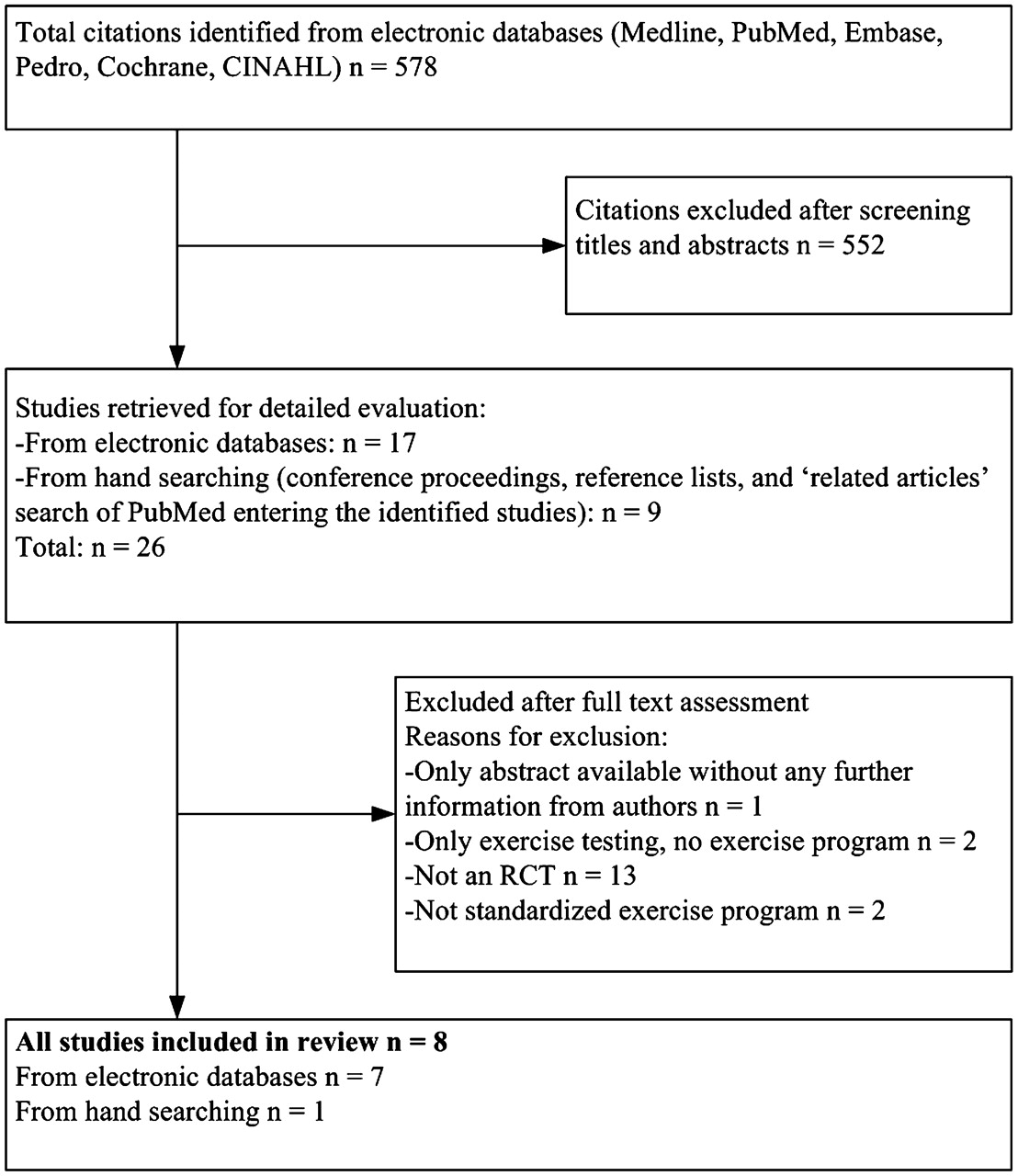
The study selection process is outlined in figure 1. Of a possible 578 trials, eight were included in this review.8–11 13 15 16 20 One study was retrieved as an abstract only26 but information was provided by the author and the full manuscript was published at the time of this review.10 In total, 388 COPD patients were randomised to either interval or continuous training. Table 1 shows the characteristics of those included in the trials. Patients were elderly (mean 67 years) and had moderate to severe COPD (mean FEV1 33–55% predicted). Seven of the eight studies included a majority of male patients,9–11 13 15 16 20 while one study8 included mostly (85%) female patients.

Study flow from identification to final inclusion of studies.
Characteristics of included studies
There was consistent agreement between reviewers for the quality assessment. Study quality ratings based on Jadad and PEDro scales are provided in table 2. The studies achieved a mean Jadad score of 2/5 (range 1–3) and mean PEDro score of 6/10 (range 5–8). Three trials provided details about randomisation,8 9 11 three reported allocation concealment8 10 11 and only two trials10 11 reported blinding of outcome assessors. Only one study included a specific statement regarding adverse events and reported no adverse events with either type of training.13
Quality assessment results
Training protocols
Continuous training protocols used moderate to high intensity exercise of 50–80% of the Ppeak, obtained on an incremental test. Exercise duration ranged from 20 to 45 min. Interval training protocols used high intensity exercise (≥80% of Ppeak, range 80–150%) of 20 s–3 min alternating with low to moderate intensity (30–75% Ppeak) recovery periods of 30 s–3 min (table 1). Two studies9 10 used 1 min intervals of higher intensity exercise (≥90% Ppeak) alternating with 2 min of low intensity exercise (≤75% Ppeak), three trials15 16 20 used 30 s intervals (100%/45% Ppeak), one study11 alternated high (50% Ppeak) and low (10% Ppeak) intensities of 20 and 40 s intervals, and one study13 used 2 min intervals of high intensity exercise (90% Ppeak) alternated with 1 min of low intensity exercise (50% Ppeak). Intensity at the start of training was selected as a proportion of Ppeak achieved during a symptom-limited incremental exercise test in seven studies.8–10 13 15 16 20 In one study,11 Ppeak for interval exercise was defined as 50% of the highest power achieved on a steep ramp test which corresponded to 98% of Ppeak on an incremental test.27
Seven studies8 9 11 13 15 16 20 included exercise on cycle ergometers for both training protocols; however, one study10 included exercise on either a treadmill or cycle ergometer. In this trial, the speed for treadmill training was determined as a percentage of the average speed elicited during the 6MWT. Total work performed during training was matched at baseline between exercise modes in six trials.9 10 13 15 16 20 In these studies, the progression of training was arbitrarily set in each group. Two studies increased the training load (intensity or duration) on an individual basis and reported that patients in interval training groups showed a trend towards less total work than those trained with continuous exercise.8 11
Exercise capacity and response
Ppeak, measured by incremental cycle ergometry, was pooled from all eight included trials (337 patients). The common effect (WMD) in Ppeak was 1 W (95% CI −1 to 3) (figure 2A). The WMD for VO2peak, measured in six trials, was −0.04 l/min (95% CI −0.13 to 0.05) (figure 2B). Oxygen uptake at lactate threshold was measured in four trials, and showed a WMD of 0.01 l/min (95% CI −0.05 to 0.07) (figure 2C).

Comparison of the effect of interval versus continuous training on (A) peak power (Watts), (B) peak oxygen uptake (l/min) and (C) lactate threshold (l/min). The square on the horizontal line represents the point estimate. The size of the square is determined by how much weight the study contributes to the pooled effect estimate. The diamond represents pooled effect estimates.
In all studies, isotime was defined for each individual as the point of termination of the shorter of the baseline and follow-up exercise test; this point most often occurs when the baseline test ends. Isotime minute ventilation (VE) from incremental cycle ergometry was measured in four studies (135 patients) with a WMD of −0.83 l/min (95% CI −5.01 to 3.36). The isotime Borg Dyspnoea Scale was pooled from four studies and showed a WMD of −0.3 (95% CI −1.0 to 0.4) between groups. The WMD for isotime breathing frequency from four studies was 0 breaths/min (95% CI −2 to 2) and isotime heart rate from five studies was 2 beats/min (95% CI −3 to 7).
Two studies (101 patients) used a constant power endurance exercise test and reported isotime responses. A WMD of −2.26 l/min (95% CI −5.59 to 1.07) was found for VE. Only one study10 reported endurance time (between-group difference=−3.7 min; 95% CI −11.8 to 4.4).
The effect of the two training modes on walk distance was measured in four trials (228 patients). Three trials used the 6MWT and one used the 12MWT; as such, data for the 12MWT were divided by two for the purposes of the meta-analysis. The WMD for 6MWT was 4 m (95% CI −14 to 23) (figure 3).

Comparison of the effect of interval versus continuous training on 6 minute walk distance (metres). The square on the horizontal line represents the point estimate. The size of the square is determined by how much weight the study contributes to the pooled effect estimate. The diamond represents pooled effect estimates.
Health-related quality of life, anxiety and depression
The CRQ dyspnoea domain was measured in four studies (218 patients). The WMD showed a non-significant trend (p=0.10) of −0.2 units (95% CI −0.5 to 0.0) between training modes (figure 4). Total CRQ scores were pooled from three studies (162 patients), resulting in a WMD of −0.1 units (95% CI −0.3 to 0.2). HAD scores were pooled from two studies. Common effects for both anxiety and depression subscales were 0.3 (95% CI −0.8 to 1.3) and 0.5 (95% CI −0.5 to 1.5) units, respectively.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Comparison of the effect of interval versus continuous training on the Chronic Respiratory Questionnaire, dyspnoea domain. The square on the horizontal line represents the point estimate. The size of the square is determined by how much weight the study contributes to the pooled effect estimate. The diamond represents pooled effect estimates.
Table 3 summarises the results of the meta-analyses for each outcome. Tests of heterogeneity on all measures of exercise capacity and quality of life were not significant, and I2 ranged from 0% to 13%, indicating that a low percentage of the variability in effect estimates was due to heterogeneity. Quantitative interpretations were limited because of the few studies available for comparison. The small number of studies also precluded the creation of funnel plots to test for the presence of publication bias. Sensitivity analyses were computed as indicated; however, there were no significant effects on the pooled analysis for any outcome.
Results of meta-analyses for interval versus continuous exercise training
Skeletal muscle adaptations
Two studies considered the effect of interval training on skeletal muscle adaptations compared with continuous exercise.10 16 Vogiatzis et al found significantly improved cross-sectional areas of type 1 and type IIa fibres and capillary to fibre ratio in the quadriceps muscle after both interval and continuous training, with no differences between groups.16 Similarly, Mador et al noted improvements in quadriceps fatigability following both types of training, with no differences between training modes.10
Tolerance to training
Attendance rates (reported in five studies) ranged from 83% to 92%, with no differences between training modes.8 10 11 13 15 Drop-outs did not differ between groups, ranging from no drop-outs13 to 40 drop-outs in a larger trial (n=100) by Anardottir and colleagues.8 The most commonly cited reason for study drop-out was exacerbations (35 participants).8 11 Both trials by Vogiatzis and colleagues15 16 reported significantly reduced perceptions of dyspnoea and leg discomfort during interval training compared with continuous training; however, two other studies8 10 noted no significant differences in symptoms between exercise modes. Puhan and colleagues11 reported significantly fewer unintended breaks of ≥1 min in the interval training group (median 2) compared with the continuous training group (median 11). In this study,11 adherence to the planned exercise protocol—that is, the proportion of patients who achieved the target exercise intensity—significantly favoured the interval training group (48% vs 24%).
Discussion
The results of this meta-analysis suggest that there are no differences between the effect of interval and continuous training on measures of exercise capacity or on health-related quality of life in individuals with moderate to severe COPD. While these findings suggest that interval training may be an alternative to continuous training in these patients, limitations in the protocols of the included studies preclude definitive conclusions.
In healthy subjects and in those with chronic heart failure, high intensity interval training has been shown to be as effective as or superior to continuous training with respect to effects on physiological markers of exercise capacity.18 19 Although we note that in the eight studies of patients with COPD included in this review, interval training resulted in significant improvements in exercise capacity and health-related quality of life, the meta-analysis does not suggest greater gains in Ppeak, VO2peak or VE from interval training compared with continuous endurance training. Two studies also suggest that both training modes elicit similar training responses in the muscles of ambulation.10 16
Several factors may have attenuated any differences observed between continuous and interval training approaches in the included studies. In patients with COPD, interval training has gained attention as a potential means of achieving greater physiological training effects, by increasing the capacity for higher intensity work.12 14 28 However, in six 9 10 13 15 16 20 of the eight studies included in this review, the total work performed for the interval and continuous exercise trained groups was matched. While this approach allows for comparison of responses after the same total work, the physiological benefits of training are more likely to be apparent when both baseline and progression of exercise intensity are individualised. In the two studies8 11 in which the load was individualised to patient tolerance, the interval trained groups performed less total work than the continuous trained groups. Given that total work is an important determinant of training response, future studies are required to determine whether patients with COPD are capable of performing more work at higher intensities with interval training, theoretically leading to greater benefits compared with continuous exercise.
Another confounding factor in the comparison of interval and continuous training was the small absolute difference in power between the high intensity phase of interval training and the continuous load, which ranged from 5 to 15 W. For example, if the average Ppeak from an incremental test is 50 W, a high intensity interval of 80% Ppeak (40 W) is only 5 W greater than a targeted continuous intensity set at 70% Ppeak (35 W). Therefore, short duration intervals at relatively moderate intensities probably place the interval group under considerably less physiological stress unless more work is performed. Furthermore, the duration of the exercise programmes in six of the studies9–11 13 16 20 was shorter than the 12 weeks recommended by guidelines for pulmonary rehabilitation.4 In unfit individuals, any exercise is likely to be effective29 and it may therefore be difficult to demonstrate large differences between training approaches during relatively short programmes, regardless of which it might favour. Finally, although a high intensity constant power endurance test provides greater sensitivity to discriminate change than an incremental exercise test,30 only one study10 included this outcome. In this study, the improvement in endurance following continuous training was greater than that following interval training and, although not statistically significant, was more than the clinically meaningful difference.31 32
A typical response following an effective exercise regimen is a post-training decrease in ventilation for any given workload. In this review, post-training pooled results for breathing frequency, heart rate, dyspnoea and VE at isotime did not show between-group differences for interval versus continuous exercise. However, if the high intensity bouts in interval training provide adequate stimulus for adaptation without causing a ventilatory response,12 14 this type of training may be better suited for patients with more severe ventilatory limitation. In fact, the mean FEV1 in the two studies8 16 that demonstrated a benefit in favour of interval training was lower (≤40% predicted) than in the other trials, providing support for this theory.
In all studies, interval and continuous training were both well tolerated and feasible among patients with COPD, with no between-group differences in withdrawals or training attendance. Puhan and colleagues11 noted superior adherence to the prescribed training protocol and less frequent rest periods in patients undergoing interval training compared with continuous exercise. However, measuring rest periods in a protocol with built in rest intervals may compromise the validity of this outcome. In contrast to the findings of Mador and Anardottir of no difference in symptoms between training modes,8 10 both trials by Vogiatzis15 16 reported reduced dyspnoea and leg fatigue during interval training sessions compared with continuous exercise. As the reports of Puhan11 and Vogiatzis15 16 included the shortest interval durations (20/40 and 30 s intervals, respectively), it is possible that interval exercise of <1 min at ≥100% of Ppeak is better tolerated than high intensity continuous exercise.
It is well established that pulmonary rehabilitation, including endurance exercise training, results in significant and clinically meaningful improvements in health-related quality of life.3 While pooled results for the CRQ total score and HAD subscales were not different between continuous and interval training, the common effect for CRQ dyspnoea showed a trend in favour of continuous training. The minimally important difference of 0.5 for this measure24 also falls within the lower end of the confidence interval, suggesting a larger benefit from continuous training. Therefore, this review has not ruled out the possibility that continuous training is more effective in changing the CRQ dyspnoea score than interval exercise.
Limitations of the meta-analysis include the heterogeneity of the training protocols as well as small sample sizes in the primary trials. The duration of the intervals ranged from 30 s to 3 min of high intensity exercise. Rehabilitation programme lengths ranged from 3 to 16 weeks and training frequencies ranged from two to five times per week. Likewise, there was a wide range in the intensity and duration of continuous training protocols. However, despite the heterogeneous nature of the training parameters, the effects were similar, suggesting that differences in adjusting several training parameters are unlikely to have a major effect on exercise performance and quality of life.10 In addition, heterogeneity as measured by the I2 statistic suggested that a low percentage of the variability in effect estimates was due to heterogeneity rather than chance sampling error. Other study design limitations included the lack of blinding of outcome assessors, high drop-out rates and poor concealment of allocation.
In conclusion, evidence from the eight trials included in this review suggests that there are no differences between the effect of interval and continuous training on improving exercise capacity and health-related quality of life in individuals with COPD. Interval training may therefore be considered as a training option or complement to continuous exercise in patients unable to tolerate high intensity continuous exercise. Patient preference should also be considered in choice of protocol as it may impact adherence to treatment. Studies of high methodological quality with large numbers of participants are required to establish which types of interval training protocols are most efficacious and to evaluate the response to training in specific subgroups of patients, particularly in those with greater disease severity.
Acknowledgments
We would like to thank the authors of the primary studies for their responses to our information requests.
References
Footnotes
Funding DB is supported by a Canada Research Chair, MB by the Ontario Respiratory Care Society and the Canadian Respiratory Health Professionals, and RG by the University of Toronto NSA Chair in Respiratory Rehabilitation Research. Other funders: CIHR, Ontario Respiratory Care Society, Canadian Respiratory Health Professionals and the University of Toronto.
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Airwaves