Article Text

Abstract
Aim To examine the relationship between birth weight and risk of asthma in a population of twins.
Methods Birth weight of all live twins (8280 pairs) born in Denmark between 1994 and 2000 was linked to information on asthma obtained from parent-completed questionnaires at age 3–9 years. Conditional logistic regression was used to calculate the risk of asthma.
Results Subjects with a history of asthma at age 3–9 years weighed on average 122 g (95% CI 85 to 160) less at birth than subjects who had not developed asthma, p<0.001. There was a linear increase in asthma risk with decreasing birth weight, OR (per 100 g) 1.04 (95% CI 1.03 to 1.05), p<0.001. Within twin pairs, the lower birthweight twin had a significantly increased risk of asthma compared with the heavier co-twin (11.3% vs 9.9%), OR 1.30 (95% CI 1.10 to 1.54), p=0.002. The result remained significant after adjusting for sex, birth length and Apgar score, OR 1.31 (95% CI 1.03 to 1.65), p=0.027. The risk tended to be higher in monozygotic co-twins compared with dizygotic co-twins, especially for high birth weight differences.
Conclusions Low birth weight is a risk factor for asthma independently of gestational age, sex, birth length and Apgar score, but this may be due, in part, to residual non-genetic confounding factors. This finding lends support to the “fetal origins hypothesis” suggesting undisclosed prenatal determinants for the risk of asthma.
- Asthma
- birth weight
- twins
- fetal origins hypothesis
Statistics from Altmetric.com
Introduction
A higher concordance for asthma and atopy in monozygotic (MZ) than in dizygotic (DZ) twins has been taken as evidence of a significant genetic component for these diseases.1 However, there is increasing evidence that the prenatal environment, particularly impaired fetal growth, plays an important role in determining a person's risk of disease later in life.2 Notably, conditions such as diabetes and cardiovascular disease have been linked to impaired intrauterine growth leading to the formulation of the “fetal origins hypothesis’; that is, that these diseases may begin as a result of abnormal development during fetal life rather than, or in addition to, a genetic predisposition.3
Several studies have examined the association between birth anthropometry and atopic diseases, but with conflicting results. In particular, low birth weight has been associated with atopic diseases in a large proportion of the studies,4–9 but not in all,10–15 whereas a number of studies have reported a higher risk of atopic diseases in subjects with high birth weight.4 5 7 8 16–18 Birth length has also been associated with asthma in one study,13 but not in others,14 as has high ponderal index.10 11 17 Furthermore, a large head circumference at birth has been associated with hay fever,19 high immunoglobulin E (IgE)13 20 and development of asthma,13 14 although evidence is circumstantial.11
Twin studies offer a powerful approach to examine the impact of genes and environment on human diseases. Particularly, studies of twin pairs discordant for a disease outcome or an exposure can be used to detect whether an association between exposure and outcome is influenced by genetic and non-genetic confounding factors. The aim of this study was to examine the association between birth weight and asthma in a Danish nationwide twin cohort and to test for underlying genetic and non-genetic confounding between these traits.
Methods
Study population
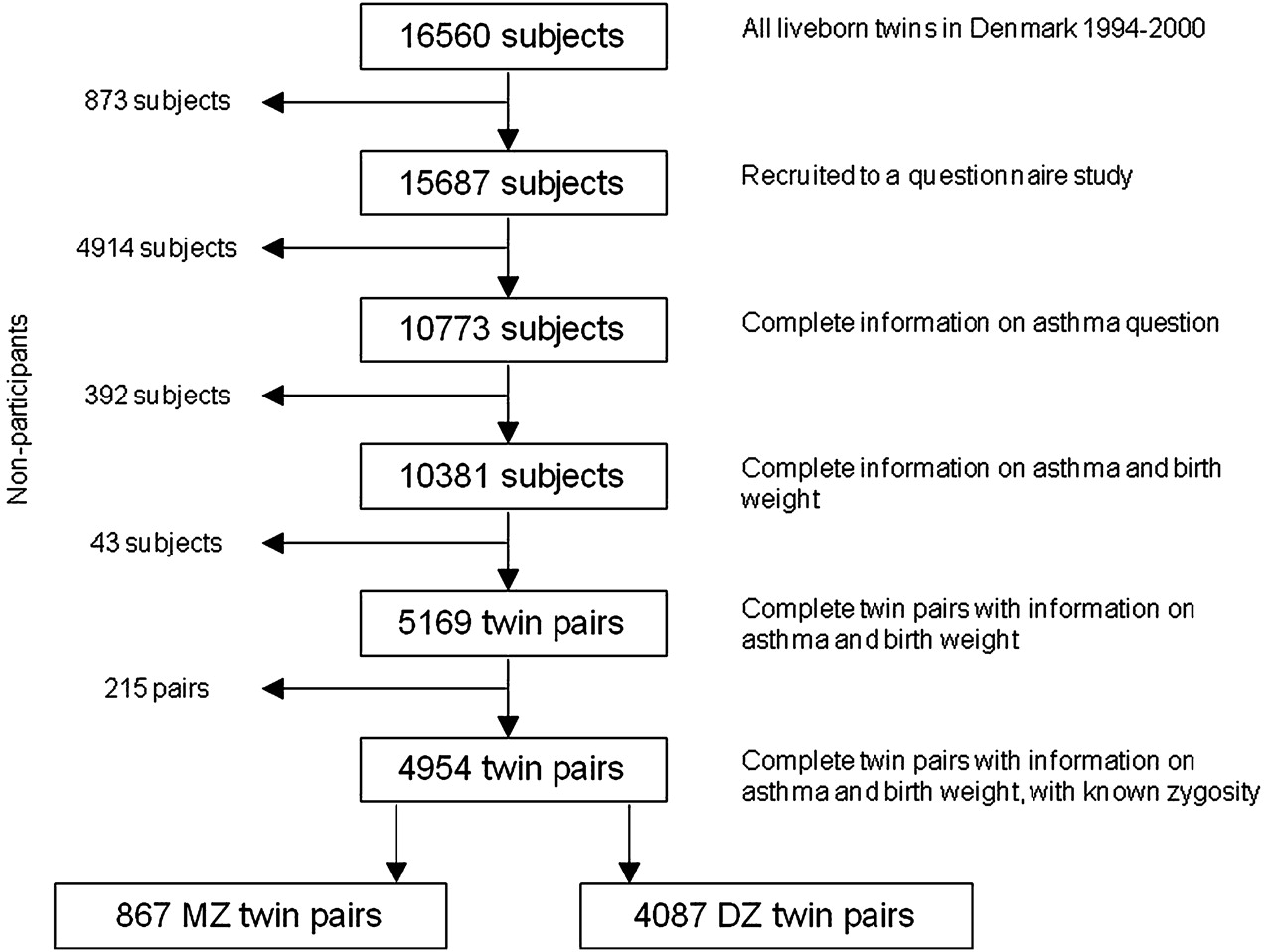
The study population comprised all live-born twins (8280 pairs) who were born in Denmark between 1994 and 2000 and included in the nationwide Danish Twin Registry. In 2003, a multidisciplinary questionnaire on health and disease was sent to these twin cohorts to be answered by the parents of the twins. Zygosity of same-sex twins was established using four similarity questions, which assign zygosity correctly in >95% of cases.21 Subjects with a history of asthma were identified on the basis of an affirmative response to the question “Has your child ever had asthma?” Information about birth weight, birth length, gestational age and Apgar score was acquired from the Danish Medical Birth Registry. Body mass index (BMI) was calculated as birth weight (kg) divided by the square of birth length (m). Apgar score is a measure of physical condition after delivery and is based on five criteria (skin colour, heart rate, reflex irritability, muscle tone and respiration). Data on birth weight were available for 15 908 subjects (96.1%), on asthma for 10 773 subjects (65.1%) and on zygosity for 13 154 subjects (79.4%); a total of 5169 twin pairs had complete data on both birth weight and asthma, and of these 4954 also had known zygosity (867 MZ and 4087 DZ twin pairs) (figure 1).
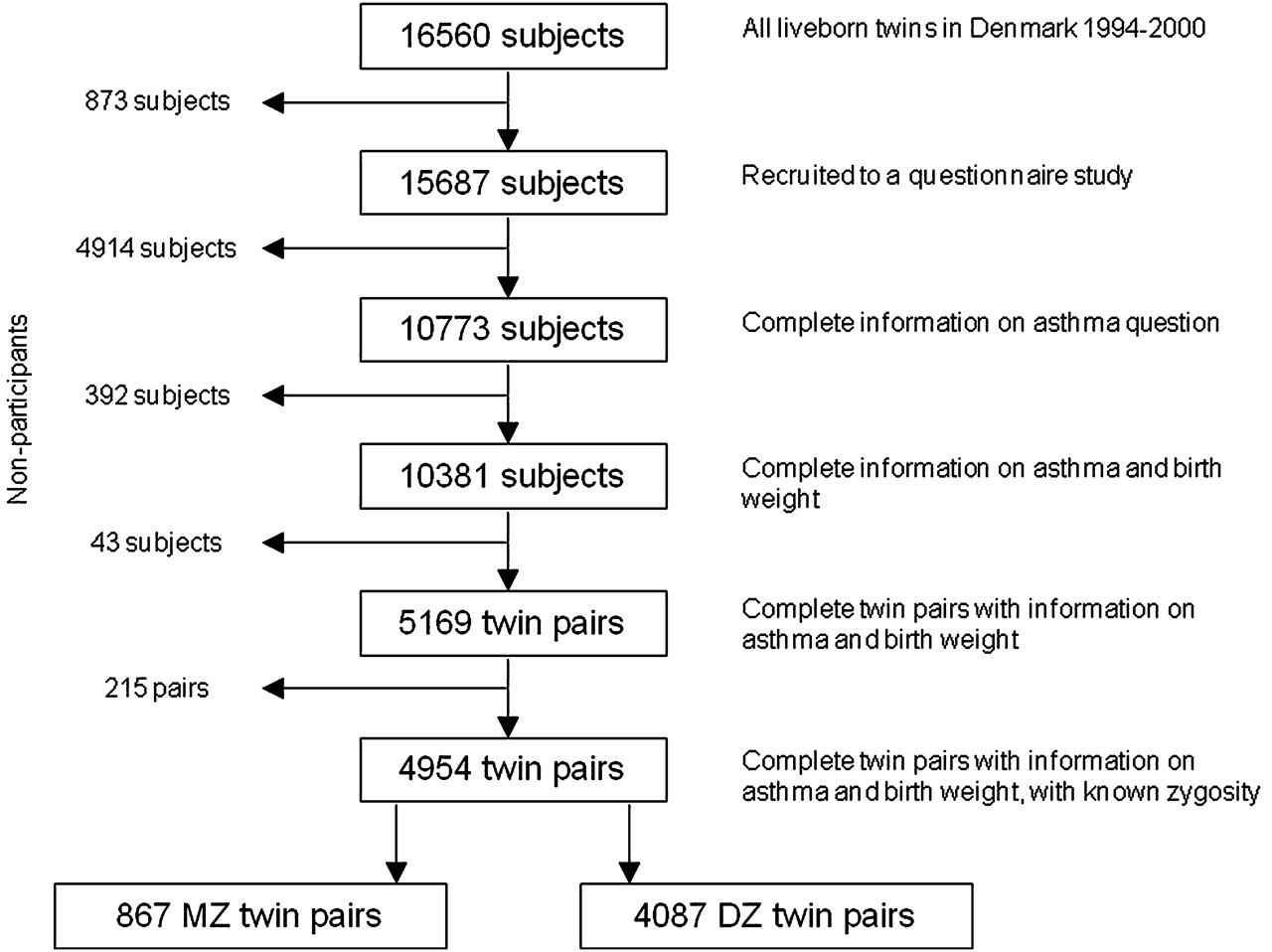
Flowchart of available information in the study. DZ, dizygotic; MZ, monozygotic.
Statistical analysis
χ2 and t tests were used to compare the distribution of birth characteristics between groups. A 1:1 matched conditional logistic regression analysis (co-twin control analysis) was applied in order to estimate the impact of birth weight on the risk of asthma. The matching was done with the lower birthweight twin in each pair being the case and the higher birthweight twin being the control. Risk estimates were given as the OR with 95% CI. DZ same-sex and DZ opposite-sex twin pairs were pooled in the analysis, and sex, birth length and Apgar score were included as covariates. In the co-twin control analysis, a higher risk of asthma in DZ co-twins compared with MZ co-twins indicates genetic confounding between birth weight and asthma, whereas a higher risk of asthma in MZ co-twins compared with DZ co-twins indicates non-genetic confounding between birth weight and asthma.22 Data were analysed with the statistical package SPSS 16.0 (SPSS, Chicago, Illinois, USA). The local Scientific Ethical Committee approved the protocol.
Results
Birth characteristics of the studied sample are given in table 1. A total of 42% of the population weighed <2500 g at birth and 49% were born preterm (before 37 weeks). The intrapair correlation in birth weight was 0.80 among MZ twins and 0.73 among DZ twins, and the intrapair correlation in birth length was 0.83 in MZ twins and 0.74 in DZ twins. The correlation between birth weight and birth length within the same individual was 0.87. In total, 10.7% of the population had a history of asthma at age 3–9 years.
Birth characteristics of a sample of Danish twin pairs, 3–9 years of age
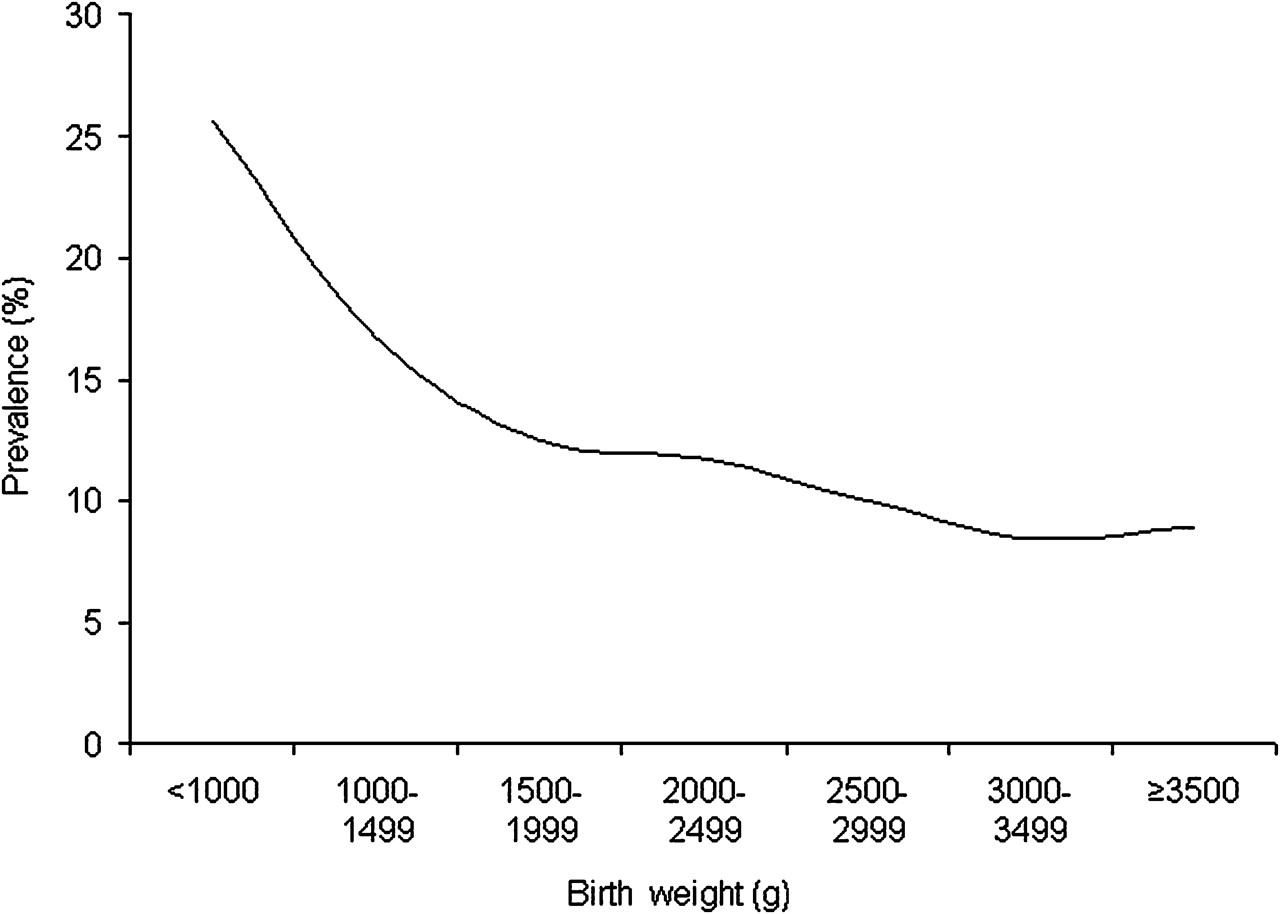
Subjects with a history of asthma weighed on average 122 g (95% CI 85 to 160) less at birth than subjects who had not developed asthma, p<0.001 (table 2). There was a linear increase in asthma prevalence with decreasing birth weight, OR (per 100 g) 1.04 (95% CI 1.03 to 1.05), p<0.001 (figure 2). Significant differences between subjects with and without asthma were also observed for sex, age at examination, birth length, birth BMI and gestational age (table 2).
{kind=link}
{kind=link}
Prevalence of asthma according to birth weight in Danish twin pairs, 3–9 years of age.
Birth characteristics of subjects with and without asthma in a sample of Danish twin pairs, 3–9 years of age
Co-twin control analysis showed that the lower birthweight twin had a history of asthma in 11.3% of the cases, whereas his or her heavier co-twin had a history asthma in 9.9% of the cases, OR 1.30 (95% CI 1.10 to 1.54), p=0.002. The result remained significant after adjusting for sex, birth length and Apgar score, OR 1.31 (95% CI 1.03 to 1.65), p=0.027. The risk tended to be attenuated in DZ twins compared with MZ twins, indicating some degree of confounding due to non-genetic risk factors, particularly for large differences in birth weight. However, formal tests for heterogeneity of risks between MZ and DZ twins were not statistically significant (table 3). We subsequently tested for effects of birth length and birth BMI on the risk of asthma using the same co-twin control methodology. The risk of asthma in the shorter twin at birth relative to the longer twin adjusted for sex, birth weight and Apgar score was OR 1.35 (95% CI 1.01 to 1.80), p=0.046, whereas the risk of asthma in the twin with the lowest BMI at birth adjusted for sex and Apgar score was OR 1.22 (95% CI 1.02 to 1.45), p=0.031. Tests for effects in twin pairs with larger differences in these measures were unreliable due to limited information in the data, but there was an indication of attenuated effect sizes in DZ twins relative to MZ twins, consistent with the findings for birth weight. Since there was no marginal effect of Apgar score, we did not test for a main effect of this parameter in the co-twin control analysis.
Risk of asthma in the lower birthweight twin relative to the higher birthweight twin in a sample of Danish twin pairs, 3–9 years of age
Discussion
This study showed that subjects with a history of asthma at age 3–9 years weighed significantly less at birth compared with subjects without asthma. The risk of asthma increased linearly with decreasing birth weight. The effect of birth weight was independent of sex, birth length, Apgar score and gestational age. However, residual non-genetic confounding factors may play a role in the association between birth weight and asthma, exemplified by the observation that the risk of asthma in birthweight-discordant MZ twins tended to be higher than in DZ twins, particularly for large differences in birth weight between the two twins in a pair. This finding substantiates the “fetal origins hypothesis”; that is, that the risk of common chronic diseases later in life may be the result of fetal programming rather than, or in addition to, genetic vulnerability.
Impaired fetal growth has, besides atopic diseases, been associated with a range of disorders such as, for example, diabetes, cardiovascular disease and schizophrenia.3 23 These observations indicate that programming of major hormonal systems during fetal life and adaptations made by the fetus in response to undernutrition could lead to permanent physiological and metabolic changes that increase the subject's risk of disease throughout life.2 Previous studies have suggested a strong genetic component for these diseases based on a higher similarity among MZ than among DZ twins. However, an alternative explanation for these findings may be a more similar early environment in MZ twins compared with DZ twins. MZ twins are monochorionic (and sometimes monoamniotic), share their placentas to a greater extent and have vascular anastomoses between their circulations. A resulting exchange of hormones, signalling and nutritional factors between the two twins during fetal life may therefore facilitate a more similar development of their physiology and a resulting similar risk of disease later in life.2 This being said, there is an undeniably strong hereditary component for asthma.1 Our result must therefore be accommodated in the explanations of the aetiology of asthma bearing this in mind.
When interpreting the results of our study it must be recognised that data on asthma were parent reported, and therefore that bias due to recall and subjective interpretation of disease status is likely. In contrast, anthropometric measures at birth were collected from a central registry with objective data from midwives’ reports and were thus independent of the disease outcome. Furthermore, co-twin control analysis enabled us to adjust indirectly for a range of unmeasured factors, such as genotype, gestational age, and maternal smoking during pregnancy and during the early life of the child. Still, residual confounding could, besides intrauterine factors, be due to respiratory infections, particularly in low birthweight infants, perinatal intensive care, dietary factors, birth order effects and factors relating to household and upbringing.
Twin pregnancies differ from singleton pregnancies in several aspects, which may affect the generalisability of our study. Mothers of twins, especially of DZ twins, tend to be older and of higher parity. Duration of gestation is shorter, twins are of lower birth weight and their neonatal morbidity and mortality is higher than that of singletons. Over 40% of twins are born preterm (before 37 weeks) and ∼50% weigh <2500 g at birth. There is some evidence to suggest differential asthma morbidity in twins compared with singletons.5 24 In particular, some studies have observed a lower prevalence of asthma in twins, possibly in part because of cross-infections between twins resulting in a T helper 1 (Th1)-driven immune response.25
We were left with a relatively low number of MZ twin pairs discordant for asthma (42 in total), which constitute the informative families for the co-twin control study. Furthermore, there was little twin-to-twin variation in birth weight within MZ pairs. Notably, the correlation in birth weight between MZ twins was 0.80, resulting in few twin pairs with high birth weight differences who were also discordant for asthma.
We conclude that low birth weight is a risk factor for asthma independently of gestational age, sex, birth length and Apgar score. However, the association between birth weight and asthma may to some extent be influenced by residual non-genetic confounding factors. This observation lends support to the “fetal origins hypothesis” suggesting undisclosed prenatal determinants for the risk of asthma.
References
Footnotes
Competing interests None.
Ethics approval This study was approved by the local Scientific Ethical Committee.
Provenance and peer review Not commissioned; externally peer reviewed.