Article Text

Abstract
Background Recommendations for diagnostic testing in hospitalised patients with community-acquired pneumonia remain controversial. The aim of the present study was to evaluate the impact of a therapeutic strategy based on the microbiological results provided by urinary antigen tests for Streptococcus pneumoniae and Legionella pneumophila.
Methods For a 2-year period, hospitalised patients with community-acquired pneumonia were randomly assigned to receive either empirical treatment, according to international guidelines, or targeted treatment, on the basis of the results from antigen tests. Outcome parameters, monetary costs and antibiotic exposure levels were compared.
Results Out of 194 enrolled patients, 177 were available for randomisation; 89 were assigned to empirical treatment and 88 were assigned to targeted treatment. Targeted treatment was associated with a slightly higher overall cost (€1657.00 vs €1617.20, p=0.28), reduction in the incidence of adverse events (9% vs 18%, p=0.12) and lower exposure to broad-spectrum antimicrobials (154.4 vs 183.3 defined daily doses per 100 patient days). No statistically significant differences in other outcome parameters were observed. Oral antibiotic treatment was started according to the results of antigen tests in 25 patients assigned to targeted treatment; these patients showed a statistically significant higher risk of clinical relapse as compared with the remaining population (12% vs 3%, p=0.04).
Conclusions The routine implementation of urine antigen detection tests does not carry substantial outcome-related or economic benefits to hospitalised patients with community-acquired pneumonia. Narrowing the antibiotic treatment according to the urine antigen results may in fact be associated with a higher risk of clinical relapse.
- Community-acquired pneumonia
- urinary antigen detection tests
- diagnostic methods
- therapeutic strategy
Statistics from Altmetric.com
Introduction
A decade ago, when blood and sputum cultures constituted the routine diagnostic approach in community-acquired pneumonia, several studies concluded that these conventional diagnostic tests did not contribute significantly to patient disease management.1 2
More recently, urinary antigen tests to diagnose pneumonia caused by Legionella pneumophila or Streptococcus pneumoniae have been introduced.3 4 Antigen tests have substantially increased the percentage of patients with aetiological diagnoses and, consequently, they have become one of the most highly employed diagnostic methods for community-acquired pneumonia.5–7 However, the clinical benefits derived from the routine application of antigen tests have not been fully evaluated, and the validity of a strategy of targeted antimicrobial therapy based on the results of these tests has not been established. The existence of polymicrobial infections, the possibility of false-positive antigen results, the potential benefits attributed to combination therapies in cases of severe or bacteraemic pneumonia and the inability to determine the antimicrobial susceptibility of pathogens have led to questions about the cost-effectiveness of this practice.8 9
Given these unresolved issues and the lack of scientific evidence, guidelines suggest a potential value of antigen testing in certain subgroups of patients, especially those with underlying conditions or those with a more severe clinical picture; alternatively, they leave the decision in the hands of physicians according to clinical or epidemiological circumstances.10 11
The purpose of our study was to perform an overall evaluation of clinical and economic consequences derived from the routine implementation of urinary antigen tests in hospitalised patients with community-acquired pneumonia.
Methods
Study setting and patient selection
A prospective, randomised, comparative trial was conducted from April 2006 to March 2008. We recruited study participants from the Internal Medicine Department in the Hospital Universitari Arnau de Vilanova in Lleida, Catalonia, Spain. All adult patients admitted from the Emergency Department with a diagnosis of community-acquired pneumonia were eligible to enter in the study.
Inclusion criteria were:
Age ≥18 years.
Clinical and radiological evidence of pneumonia consisting of two or more of the following clinical manifestations: fever, chills, cough, sputum production, pleuritic chest pain and signs of lung consolidation; along with the presence of an infiltrate in the chest radiograph that was consistent with acute infection.
Class IV or V of the Pneumonia Severity Index or the presence of additional circumstances that justify hospital admission.
Clinical stability between 2 and 6 days after admission, defined as the condition in which all the following threshold values were achieved for a 24 h period: temperature, ≤37.2°C; heart rate ≤100 beats/min; respiratory rate, ≤24 breaths/min; systolic blood pressure, ≥90 mm Hg; and oxygen saturation of ≥90% or arterial oxygen partial pressure of ≥60 mm Hg when the patient was not receiving supplemental oxygen.12
Exclusion criteria were:
Misdiagnosis at admission.
Nosocomial-, nursing home- or healthcare-associated pneumonia.
Risk factors for infection due to Pseudomonas aeruginosa, anaerobia or other microorganisms that require alternative therapeutic regimens.
Infection caused by tuberculosis or opportunistic microorganisms.
Empyema at admission.
Immunosuppression, for reasons including HIV infection, haematological neoplasms, solid-organ and bone-marrow transplantation, neutropenia and immunosuppressive treatments.
Patients provided written informed consent to participate in the trial. The study was approved by the scientific and ethic committees of our institution.
Procedures and treatment
Therapeutic strategy at admission was identical for all patients and based on international guidelines.10 11 Thus, patients received one of the following two intravenous regimens upon entry: (1) β-lactam (ceftriaxone, 2 g daily, or amoxicillin–clavulanate, 1 g three times daily) plus macrolide (azithromycin, 500 mg daily) or (2) fluoroquinolone (levofloxacin, 750 mg daily), according to the preferences of the attending physician.
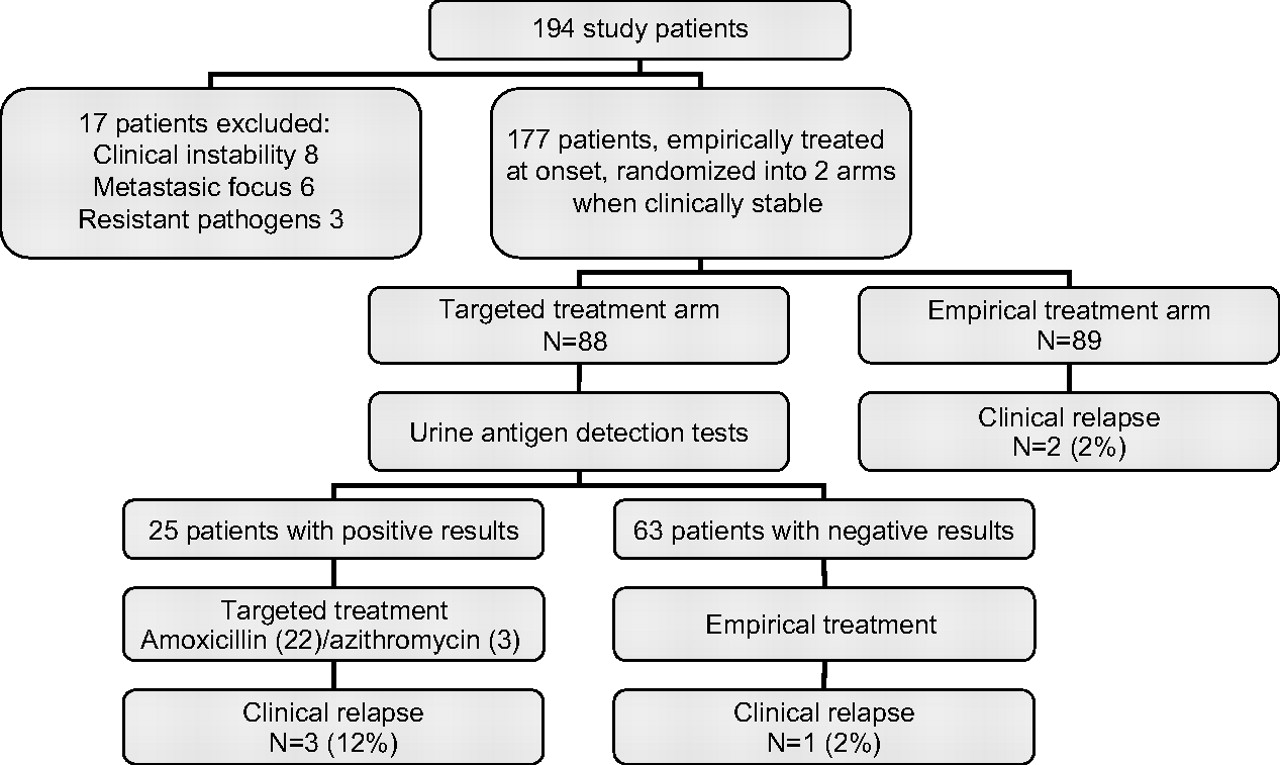
Patients underwent a daily clinical assessment during their hospital stay and at least one follow-up visit took place 1 month after discharge. Patients who achieved clinical stability between 2 and 6 days after admission and could tolerate oral food were randomly assigned to one of two treatment arms in order to receive either empirical treatment (ET) or targeted treatment (TT) (figure 1), and were treated as follows:
{kind=link}
Randomisation of 194 hospitalised patients with community-acquired pneumonia and clinical relapses according to different therapeutic strategies.
Subjects assigned to the ET arm were treated according to recommendations from international guidelines. Those patients initially treated with a combination of β-lactam plus macrolide were switched to receiving a broad-spectrum oral β-lactam (amoxicillin–clavulanate, 875/125 mg three times daily or cefditoren, 400 mg twice daily) to complete a 10 day course, plus oral macrolide (azithromycin, 500 mg daily) to complete 5 days of treatment. Alternatively, patients who had received intravenous levofloxacin completed a course of 10 days with the same antibiotic (levofloxacin, 750 mg daily).
Patients assigned to the TT arm were switched to oral amoxicillin, 1 g three times daily, to complete a 10 day course, if the pneumococcal urine antigen test was positive or to oral azithromycin, 500 mg daily to complete a 5 day course, if the L pneumophila urine antigen test was positive. Conversely, for patients with negative urinary antigen tests, oral treatment was the same as for patients assigned to the ET group.
In the absence of additional medical circumstances, patients were discharged between 24 and 48 h after switching from intravenous to oral treatment.
Microbiological tests
A microbiological study was performed upon entry, before randomisation, including the following samples:
Two sets of blood for conventional cultures.
Sputum for Gram stain and culture, when a good quality sample was available.
Pleural fluid, if present, for Gram stain and culture in conventional media.
Paired serum samples, at presentation and 4–8 weeks later, for serological studies to detect the presence of antibodies against Mycoplasma pneumoniae, Chlamydophila pneumoniae, Chlamydophila psittaci and Coxiella burnetii.
Urine for detection of antigens of S pneumoniae or L pneumophila by using a rapid test (BinaxNow test, Leti Laboratories, Barcelona, Spain).
Endpoints and definitions
The following endpoints were evaluated:
Outcome parameters: mortality, clinical relapse, admission to the intensive care unit, incidence of adverse events, length of hospital stay and readmission. Clinical relapse was considered to occur when clinically stable patients who were starting follow-up oral treatment regained clinical instability (temperature, >37.2°C; heart rate, >100 beats/min; respiratory rate, >24 breaths/min; systolic blood pressure, <90 mm Hg; or oxygen saturation of <90% or arterial oxygen partial pressure of <60 mm Hg on room air) and developed or worsened one or more clinical manifestations of respiratory infection, not attributable to alternative causes.Adverse events were subjectively reported by the patients or were observed by the clinical staff during therapy and for the 30 day period posttherapy. They were defined as symptoms or signs that could not be attributed to the pneumonia, beginning after the start of antibiotic treatment.
Economic parameters: cost of hospital stay, cost of antimicrobial treatment and cost of diagnostic procedures. All costs were calculated in Euros. The cost of hospital stay was calculated from the perspective of the Hospital Financial Department. Thus, costs were derived from the cost per day over the years 2005 and 2006 including room stay and basic diagnostic and therapeutic procedures (€210), multiplied by the mean number of days of hospital stay. The daily costs of antimicrobial treatments was calculated from the perspective of the Hospital Pharmacy. The respective daily costs of antimicrobials were: €1.20 for 2 g of intravenous ceftriaxone; €45.75 for 750 mg of intravenous levofloxacin; €21.50 for 500 mg of intravenous azithromycin; €0.92 for 3 g of intravenous amoxicillin–clavulanate; €4.08 for 750 mg of oral levofloxacin; €7.90 for 800 mg of oral cefditoren; €2.12 for 2.62 g of oral amoxicillin–clavulanate; €3.10 for 500 mg of oral azithromycin and €0.88 for 3 g of oral amoxicillin. Finally, the cost of microbiological tests was calculated from the perspective of the Hospital Laboratory of Microbiology. The cost of the pneumococcal antigen test was €16.30, and the cost of the Legionella antigen test was €21.00.
Exposure to antimicrobials: length of the overall antimicrobial treatment, length of intravenous antimicrobial treatment and exposure to broad-spectrum and narrow-spectrum antimicrobials. Exposure to individual antibiotics was measured using the number of defined daily doses (DDD) per 100 patient days. The number of DDD of each antibiotic was calculated using the total grams of individual antibiotics dispensed to study patients for each route of administration divided by the value of one DDD. Ceftriaxone, amoxicillin–clavulanate, cefditoren and levofloxacin were considered broad-spectrum antimicrobials. Amoxicillin and azithromycin were considered narrow-spectrum antimicrobials.
Statistical analysis
First analysis of the endpoints was performed on all randomised patients distributed in the two treatment arms, according to the intent-to-treat principle. We also performed a subanalysis of patients according to the real strategy employed, by comparing empirically treated patients with patients treated according to antigen test results.
We compared continuous variables between groups by the Mann–Whitney U test, and proportions between groups by the χ2 test or Fisher exact test. All statistical tests were two tailed, and the threshold of statistical significance was a p value <0.05. We performed all statistical analysis with SPSS software, version 12.0 (SPSS, Chicago, Illinois, USA).
Results
From a total of 194 eligible patients with community-acquired pneumonia, 17 were excluded for the following reasons: eight patients did not reach clinical stability, six developed a metastatic infectious focus (five, empyema; and one, endocarditis) and three had infection caused by resistant microorganisms (P aeruginosa was isolated from sputum in one case, and Klebsiella pneumoniae and Escherichia coli were each isolated from blood in two remaining patients). Consequently, 177 patients were finally entered and randomised; 89 were assigned to the ET arm, and 88 to the TT arm. Baseline demographic and clinical characteristics of patients are presented in table 1.
Intent-to-treat analysis of demographic and baseline characteristics of the study patients distributed in two arms: empirical treatment and targeted treatment
No statistically significant differences in outcome parameters were found between groups (table 2). A greater incidence of minor adverse events was observed in the ET group (16 events (18%) vs 8 events (9%) in the ET and the TT arms, respectively), mainly referred to the gastrointestinal tract (p=0.12). Treatment of one patient in each arm was stopped because of major adverse events potentially related to drugs (hepatitis in one patient in the ET arm, who had received levofloxacin; and leucocytoclastic vasculitis in one patient in the TT arm, who had received amoxicillin).
Intent-to-treat comparative analysis of the outcomes of study patients distributed in two arms: empirical treatment and targeted treatment
The mean overall cost of patient care was €1657.00 among subjects in the TT arm (hospital stay, €1481.40; consumption of antimicrobials, €138.30; and urine antigen tests, €37.30) and €1617.20 among subjects in the ET arm (hospital stay, €1470.70; and consumption of antimicrobials, €146.50) (p=0.28).
Table 3 details the antibiotic consumption in both subsets of patients. Exposure to intravenous antimicrobials was similar in both groups. In contrast, a small increase in the use of oral broad-spectrum antimicrobials was observed for patients assigned to the ET arm.
Intent-to-treat evaluation of exposure to antimicrobials in study patients distributed in two arms: empirical treatment and targeted treatment
Antigen detection tests were positive in 25 patients (25%) assigned to the TT arm (S pneumoniae, 22; and L pneumophila, 3). As a consequence, 152 patients were in fact empirically treated. In comparative analyses between these subsets of patients (tables 4 and 5) no differences were found for most of the outcome parameters. However, patients treated according to their urine antigen results showed a higher incidence of clinical relapse, seen in 3 of 25 patients (12%), all receiving amoxicillin. These three patients were men; 60, 61 and 91 years old, respectively; and only one had a non-severe chronic obstructive pulmonary disease as underlying co-morbidity. They initially received the combination β-lactam plus macrolide and, between 2 and 4 days after admission, when clinically stable, initiated the oral regimen with amoxicillin, 1 g three times daily, but were found to be clinically unstable 24–48 h later, manifested by fever and many of the symptoms that they showed at entry. Although daily monitoring of biological parameters was not performed, the three patients also showed, during relapse, high C-reactive protein levels (84.3, 107.3 and 221.5 mg/l, respectively). None of these patients developed empyema, parapneumonic effusion or other metastatic foci. In all cases, the outcome was favourable only on restarting the initial empirical regimen. An amoxicillin-resistant E coli was later isolated from initial blood cultures in one case, but all complementary microbiological tests provided negative results for the remaining two patients. In contrast, only 3 of 152 empirically treated patients (2%) experienced a clinical relapse with the oral regimen (p=0.04). Small reductions in the incidence of adverse events, and in the use of oral broad-spectrum antimicrobials (levofloxacin, amoxicillin–clavulanate and cefditoren), mainly replaced by oral amoxicillin, were found in patients treated according to positive antigen tests.
Comparative analysis of outcomes between subsets of patients according to the therapeutic strategy employed
Evaluation of exposure to antimicrobials in both subsets of patients according to the therapeutic strategy employed
Discussion
In this prospective, randomised study, we evaluated the overall consequences of the implementation of urine antigen detection tests in order to establish infection by S pneumoniae or L pneumophila in a cohort of hospitalised patients with community-acquired pneumonia. Our results suggest that this microbiological information does not provide benefits in terms of patient outcome or cost-effectiveness. In fact, only small reductions in the incidence of adverse events and exposure to broad-spectrum antimicrobials were observed. Conversely, the narrowing of therapy on the basis of antigen test results may carry a higher risk of clinical relapse.
It has been extensively demonstrated that the implementation of pneumonia guidelines produces substantial benefit to patients. Guideline-concordant antibiotic treatment has been associated with improved in-hospital survival, shorter time to clinical stability, shorter time to switch therapies and reduced hospital stay.13–16 Therefore, the findings from our study, showing the absence of patient outcome benefits based on the use of urine antigen tests, were somewhat predictable. No benefits in terms of mortality, pneumonia-related complications and length of hospitalisation, as compared with patients treated according to guidelines, were seen.
The most remarkable finding of our study is related to the risk of treatment failure after starting oral treatment guided by antigen test results. Twelve per cent of clinically stable patients who were switched to oral amoxicillin in concordance with a positive urine antigen test showed a clinical relapse (as compared with only 2% of empirically treated subjects). In one patient, an amoxicillin-resistant E coli infection was later isolated from samples of blood obtained at admission. We can only speculate as to whether this patient had a dual infection or a false-positive result of pneumococcal urine antigen test. In other cases, no microbiological causes to justify the poor outcomes were found; however, similarly, dual infections or false-positive results from urine antigen detection tests are the most reasonable explanations. The inclusion of additional rapid tests in the initial strategy in order to detect atypical agents could reduce the risk of uncovered agents in mixed infections; however, we know that a high proportion of pathogens remain undetected in community-acquired pneumonia, even employing a wide battery of diagnostic tests. Finally, we believe that, given current levels of S pneumoniae penicillin resistance, it seems more difficult to attribute treatment failure to potential amoxicillin resistance of pathogens.17 18
Hospital stay is the most important determinant of the total costs for hospitalised patients with community-acquired pneumonia.19–21 Therefore, it is unlikely that a strategy that is not associated with a reduction in the hospital stay would be able to reduce costs. In our study, which showed no statistically significant differences in the length of hospitalisation, costs of diagnostic procedures exceeded the reduction of costs for antimicrobials in patients with TT. In fact, four sets of antigen tests were needed to facilitate the use of narrow-spectrum antimicrobials in one patient, and this strategy was only applicable between 2 and 4 days after admission. Certainly, earlier introduction of pathogen-directed therapy, even within the first 24 h period, would increase economic benefits, but, according to our experience, this strategy is risky in patients with severe pneumonia; additionally, several studies concluded that the maintenance of macrolides in combination with β-lactams could reduce morbidity and mortality in patients with severe pneumococcal pneumonia.9 22 The relative insensitivity of the antigen detection techniques and the limitation of the method to Legionella serogroup 1 also contribute to reducing the expected benefits.
On the positive side, we only can include more questionable benefits. First, we found a non-statistically significant reduction in the incidence of adverse events, although we suspect that the difference could reach statistical significance if we increased the sample size. These adverse events were non-severe, mainly related to the gastrointestinal tract and not associated with a withdrawal of treatment. Secondly, increased use of narrow-spectrum antimicrobials undoubtedly carries ecological benefits, reducing the pressure for sustained antibiotic resistance. However, in clinical practice, the real impact of this strategy appears to be very slight taking into consideration that this policy was only applicable to 25% of the patients, for approximately half of the treatment duration and mainly for a period of outpatient care. Finally, we must recognise the epidemiological value of results provided by urine antigen tests, although they are limited by the lack of information about antimicrobial susceptibilities of the aetiological agents.
Previous reports in this field are quite scarce. Guchev et al reported a non-randomised study that evaluated a therapeutic approach based on the results of the pneumococcal urinary antigen test in young immunocompetent patients with non-severe pneumonia.23 Subjects who had a positive test were treated with amoxicillin and the remaining patients received clarithromycin. The difference in clinical success rates between groups was not statistically significant, although treatment failed for 10% of patients receiving amoxicillin (as opposed to 6% of patients receiving clarithromycin). On the other hand, van der Eerden et al published a randomised, controlled trial that compared empirical antibiotic treatment and pathogen-directed treatment. In their study, therapeutic decisions were taken on the basis of clinical presentation and microbiological results, including results of urine antigen detection tests.24 The authors were unable to associate pathogen-directed antibiotic strategy with statistically significant benefits in terms of mortality or additional outcome parameters, except for a reduction in minor adverse events. In this study, 15 of 62 patients (24%) treated according to rapidly obtained microbial results suffered failure of their treatment.
In summary, our results suggest that the routine implementation of urine antigen tests for early detection of S pneumoniae and L pneumophila, pathogens with patterns of antimicrobial susceptibility covered by recommended regimens in guidelines, would not greatly benefit hospitalised patients with community-acquired pneumonia.
References
Footnotes
See Editorial, p93
Linked articles 124156.
Funding Ciber de Enfermedades Respiratorias (Ciberes 06/06/0028) Spain.
Competing interests None.
Ethics approval This study was conducted with the approval of the Scientific and ethic committees of Hospital Universitari Arnau de Vilanova, Lleida, Spain.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.