Article Text

Statistics from Altmetric.com
- Bronchoscopy
- cryptococcus
- eosinophilia
- imaging/CT MRI etc
- multiple pulmonary nodules
- opportunist lung infections
- respiratory infection
A 22-year-old woman was admitted unwell with headache, fever and encephalopathy. She was born in the UK to parents from Hong Kong. She had a past history of asthma, perennial rhinitis and atopic dermatitis for which she took a budesonide 100 μg turbohaler and beclomethasone nasal spray. Three weeks before admission she had returned from holiday in Valencia and shortly after her return developed a flu-like illness followed by worsening asthma symptoms. Despite increasing usage of her corticosteroid turbohaler to eight puffs a day, her cough and wheeze worsened. Her GP prescribed a 5-day course of prednisolone 50 mg daily (approximately 1 mg/kg). Her asthma symptoms improved but she developed a headache 2 days after finishing the corticosteroid course. Over the next 5 days she became more unwell with worsening headache and presented to hospital.
On admission she was drowsy with signs of meningism. MRI brain showed a few small hyperintense foci bilaterally. Blood tests showed an eosinophil count of 16.8×109/l (total white cell count 24.4×109/l) and IgE level of 5553 kU/l. Lumbar puncture opening pressure was over 40 cm of water. Cerebrospinal fluid (CSF) white cell count was 33/mm3, with numerous lymphocytes and eosinophils. Serology for HIV-1 and 2 antibodies was negative and HIV RNA was undetectable. Testing for anti-neutrophil cytoplasmic antibodies and anti-nuclear antibodies was negative. A whole body CT scan showed multiple, small, randomly distributed pulmonary nodules (figure 1) and small volume lymphadenopathy in the chest.
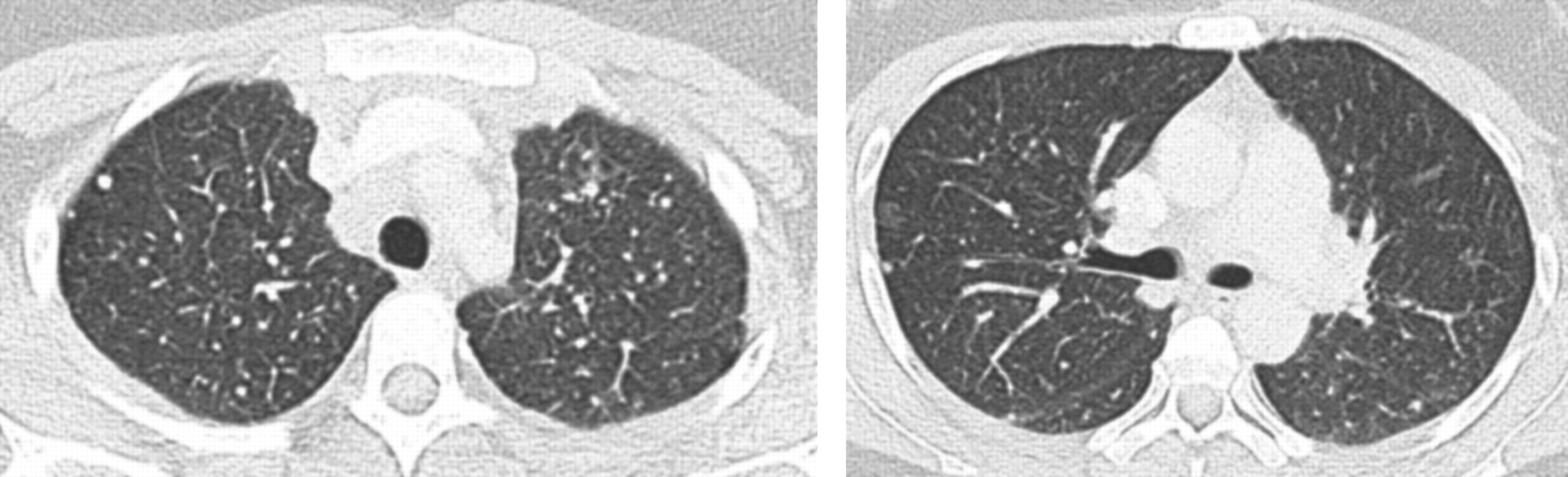
Cross-section (1.5 mm) CT chest images showing pulmonary nodules.
Questions
What is the differential diagnosis of the nodular lesions on CT?
What is the next investigation?
See page 1085 for answers
Answers
From the questions on page 1066
India ink staining of CSF demonstrated cryptococcus and she was started on flucytosine and amphotericin. Cryptococcus neoformans was cultured from the blood (figure 2) and CSF. The differential diagnosis for the pulmonary nodules includes pulmonary cryptococcus, sarcoidosis, disseminated tuberculosis and Wegener's granulomatosis. Sarcoidosis, a common cause of nodular pulmonary shadowing and lymphadenopathy, has an association with cryptococcus.1 This association is due to impaired T-cell function and pulmonary T-cell sequestration in sarcoidosis. In immunocompetent patients pulmonary cryptococcus usually presents on CT as multiple nodules of variable size, although it can present as a solitary nodule and rarely cavitating nodules.2 3 Lymphadenopathy is less common and eosinophilia is recognised.4

India ink preparation (×400 magnification) showing numerous capsulated yeasts, typical of Cryptococcus neoformans.
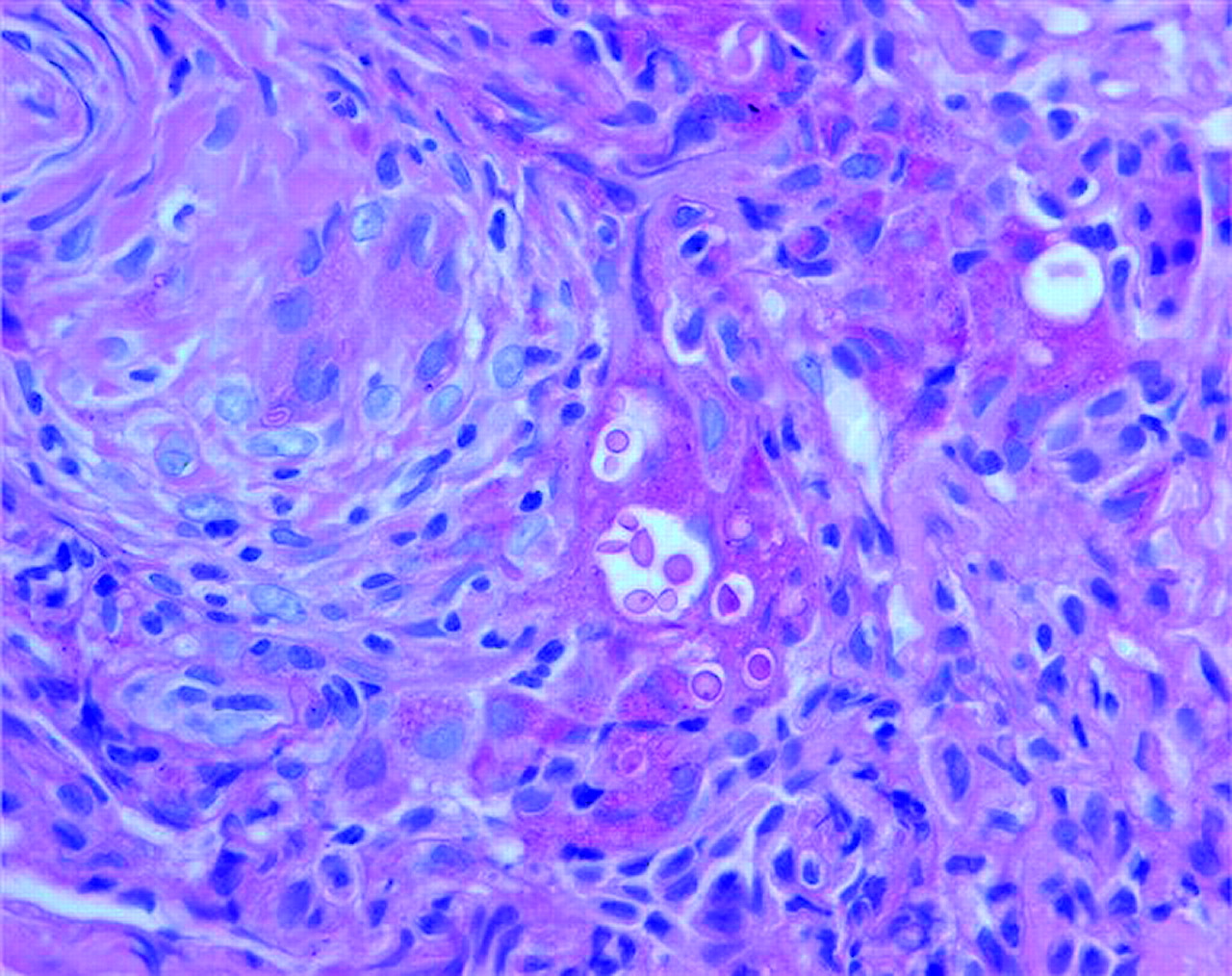
The next investigation is bronchoscopy with washings, endobronchial and transbronchial biopsy. Transbronchial lung biopsy demonstrated granulomata with cryptococci (figure 3)—the final diagnosis is disseminated cryptococcosis with pulmonary nodules and meningitis.

{kind=link}
{kind=link}
{kind=link}
Transbronchial lung biopsy with periodic acid Schiff stain (×400 magnification) showing round cryptococcus within lung parenchyma and adjacent granuloma.
She required repeat lumbar punctures to reduce CSF pressure. After 1 month of treatment for cryptococcosis her IgE level halved to 2817 kU/l, eosinophilia decreased and headaches abated. Her antifungal treatment was changed to fluconazole. A repeat CT scan showed resolution of the multiple pulmonary nodules and decreased volume of lymphadenopathy. Three months later her IgE level was 1040 kU/l and eosinophilia resolved.
No cause of immunodeficiency was found on extensive investigation including T-cell subset analysis and dynamic T-cell function tests. The serum IgE was markedly elevated. Atopic status, with associated T-helper type 2 dominant immune responses, may predispose to invasive fungal infection.5 It is likely that the patient was colonised by cryptococcus with subsequent dissemination after high-dose steroid immunosuppression. Pulmonary cryptococcal infection may increase allergic inflammation and airway responsiveness.6 Cryptococcus is a yeast found worldwide, particularly in soil and bird excrement. It is increasingly recognised to be a cause of disease in immunocompetent as well as immunodeficient individuals. There is a spectrum of cryptococcal lung disease, which may well be underdiagnosed.
Footnotes
Competing interests None.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.