Article Text

Abstract
Background Few if any studies of the association between pulmonary tuberculosis (TB) and lung function loss have had access to premorbid lung function values.
Methods Using a retrospective cohort design, the study recruited employed South African gold miners who had undergone a pulmonary function test (PFT) between January 1995 and August 1996. The ‘exposed’ group comprised 185 miners treated for pulmonary TB after the initial PFT and the ‘unexposed’ group comprised 185 age-matched miners without TB. All participants had a follow-up PFT between April and June 2000. The outcome of interest was decline in lung function during the follow-up period as measured by forced vital capacity (FVC) and forced expiratory volume in 1 s (FEV1).
Results After controlling for age, height, baseline lung function, silicosis, years of employment, smoking and other respiratory diagnoses, pulmonary TB during the follow-up period was associated with a mean excess loss of 40.3 ml/year in FEV1 (95% CI 25.4 to 55.1) and 42.7 ml/year in FVC (95% CI 27.0 to 58.5). Lung function loss was greater among those with more severe or later clinical presentation of TB. Breathlessness was twice as common among TB cases (OR 2.20, 95% CI 1.18 to 4.11).
Conclusion There is a need for greater clinical recognition of the long-term respiratory consequences of treated pulmonary TB. Early detection of TB would help to reduce these sequelae and remains a priority, particularly in a workforce already subject to silica dust disease. However, strategies such as dust control, worker education about TB and dust and TB preventive therapy are also needed to avert the disease itself.
- Tuberculosis
- silicosis
- mining
- lung function
- occupational lung disease
- tuberculosis
Statistics from Altmetric.com
Introduction
In both occupational and non-occupational settings, a number of studies have demonstrated an association between pulmonary tuberculosis (TB) and subsequent lung function loss, regardless of treatment.1–7 However, none of these studies was able to assess lung function in the same subjects both before and after the occurrence of TB.
The question of whether and to what extent TB contributes to excessive lung function decline is particularly relevant to South Africa's gold mining industry, which employs over 150 000 miners,8 with a reported TB incidence exceeding 4000 episodes per 100 000 miners per year.9 Known TB risk factors among gold miners include silica dust exposure, silicosis10 11 and HIV infection.12 Studies in the past decade have recorded a prevalence of silicosis of 19% in older active miners13 and up to 27% in former miners,14 and HIV seroprevalences of 24–30% in the general gold mining workforce.9
Silicosis alone has been shown to accelerate lung function loss, with the extent of decline proportional to the degree of silicosis.7 15 With regard to TB, it has been shown cross-sectionally that the proportion of gold miners with residual airflow impairment (defined as forced expiratory volume in 1 s (FEV1) <80% of predicted) was 18.4% after one episode of TB, 27.1% after two episodes of TB and 35.2% after three or more episodes of TB.3
Lung function testing was incorporated into the gold mining industry's occupational health surveillance in 1994.16 This provided an opportunity to quantify the excess loss of lung function after an episode of TB relative to miners without TB, and to identify TB-related clinical predictors of excess lung function decline as well as any increased prevalence of chronic respiratory symptoms.
Methods
Study population and cohort selection
The study population consisted of black male gold miners at a single gold mining company in South Africa's Free State province. This is a largely migrant workforce from rural South Africa and neighbouring countries, 90% of whom work underground. During the period of the study the mine hospital provided the sole source of tertiary care and also managed the TB control programme. This entailed maintenance of a TB database, which included data on occurrence and clinical characteristics of TB episodes. Every employee underwent annual radiological screening for TB. Pulmonary function tests (PFTs) were required at the start of employment, every 3 years thereafter and upon discharge.
Previous work at the study site identified the longitudinal spirometry values from January 1995 through August 1996 as having acceptable reliability.16 Eligibility was thus restricted to miners who received a PFT during this time period (‘baseline’ PFT). To ensure that all participants were free of TB at baseline, miners diagnosed with TB within 2 months of their baseline PFT were excluded. In addition, only miners still employed on 12 December 1999 were considered eligible.
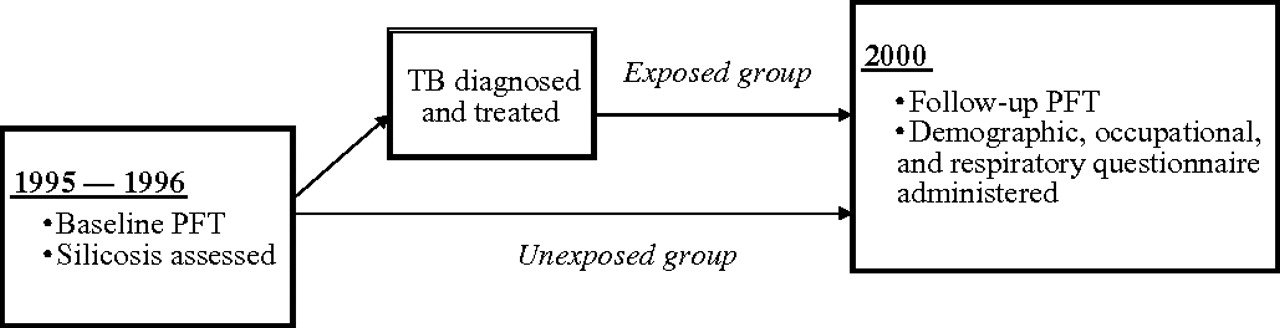
The study used a matched retrospective cohort design (figure 1). The mine's TB database was used to identify eligible miners who were diagnosed with and completed treatment for pulmonary TB during the study period (1995–2000). Participants were in the employ of the mining company during the entire study. In addition to checking the TB database, routine checks against mine health service laboratory and pharmacy electronic records were carried out to identify possible TB cases. Participants were also asked about past TB during the questionnaire interview (see below).

Study timeline (1995–2000). PFT, pulmonary function test; TB, tuberculosis.
Men with a documented TB history constituted the exposed group. This group also included 47 miners who had successfully completed treatment for a previous TB episode prior to the baseline PFT. Age-matched individuals were selected from the group of eligible miners still employed in 2000 with no documented history of TB in the TB database (the unexposed group).
All subjects underwent a follow-up PFT. A questionnaire eliciting respiratory, smoking and occupational information was completed between April and July 2000 (ie, at follow-up only). Asthma, pneumonia or bronchitis were recorded if the participant had ‘ever been told by a doctor’ that he had the condition. The date of first employment and contract renewals were obtained from the recruitment agency. Any corrections were made using company data and by verification with the participants.
Pulmonary function testing
Baseline PFTs were conducted between January 1995 and August 1996 and follow-up PFTs were performed between April and July 2000. Both PFTs were performed at the same location using the same machine and procedures. Maximal forced expiratory manoeuvres were performed in the seated position using a Hans Rudolph pneumotachograph (Flowscan, Electromedical Systems Inc, Nyon, Switzerland). Following calibration and validation with a 3.0 litre syringe, the subject's flow–volume loop was recorded from which the FEV1 and forced vital capacity (FVC) were documented. At each PFT the test date, birth date, weight and height in stocking feet were recorded. The FEV1 and FVC from the manoeuvre which produced the best FVC were recorded for the study using the pneumotachograph's software procedure. Baseline testing was conducted by trained technicians at the mine's occupational health centre and follow-up testing by study personnel trained in spirometry. No bronchodilator was administered.
Silicosis
Silicosis status was assessed at the time of the baseline PFT using mass miniature radiography, a method previously tested against subsequent autopsy in gold miners using the International Labour Organization (ILO) classification system.17 18 That study showed a sensitivity of 71% and a specificity of 96% for finding ≥5 palpable nodules at autopsy, when silicosis was defined as ILO profusion ≥1/1.18 In the current study a single experienced reader evaluated the x-rays for the presence and grade of silicosis using the ILO classification system. This is based on four major grades (0–3), denoting increasing profusion of rounded opacities on the x-ray, and allows for intermediate (minor) grades such as 1/0.18 ILO categories 1/1 and above were considered silicosis positive.
Tuberculosis
Diagnosis of TB occurred either through active surveillance via the mine's radiographic screening programme or self-presentation at the occupational health centre. Three sputum specimens were collected for microscopic examination and culture from miners with suspected TB. Concentrated smears were stained with auramine for evaluation by fluorescent microscopy and further assessed using Ziehl–Neelsen staining. After decontamination with 4% sodium hydroxide, sputum samples were inoculated onto Lowenstein–Jensen (LJ) slopes and incubated for up to 8 weeks. Colorimetric ribosomal RNA hybridisation (Accuprobe Mycobacterium tuberculosis Complex Culture Identification Test; Gen-Probe, San Diego, California, USA) was employed to confirm the presence of M tuberculosis on LJ slopes with >5 colonies. Positive cultures were sent to the South African Institute for Medical Research mycobacteriology laboratory for identification of non-tuberculosis mycobacterium and drug susceptibility testing.
All miners diagnosed with TB received directly observed therapy in accordance with national TB guidelines. The treatment regimens for new and retreatment cases have been described previously.19 Subjects with suspected TB had standard sized chest x-rays done at diagnosis, after 2 months of treatment and at treatment completion. The non-TB group did not have follow-up x-rays as part of the study.
Patients were categorised as culture positive for TB if a positive sputum culture was obtained and the subject presented with compatible clinical features. Culture negative TB was diagnosed if compatible clinical and radiological changes were present, plus at least one of the following: (1) smear positive or (2) no response to amoxicillin and a positive radiological response to TB treatment. Subjects were considered new TB cases if they had never previously been treated for TB and retreatment cases otherwise. Cured TB cases were those who completed treatment with documented smear conversion; those who completed treatment without documented conversion were classified as completed only.
HIV testing
Confidential HIV testing with pre- and post-test counselling was offered to all TB suspects, although not to the non-TB comparison group. HIV infection was diagnosed if both the screening (Enzymun-Test Anti-HIV 1+2+subtype O, Boehringer Mannheim Immunodiagnostics, Mannheim, Germany) and confirmatory ELISA (IMx system HIV-1/HIV-2 III Plus, Abbott Diagnostics, Illinois, USA) tests were positive.
Data analysis
SAS Version 9.1 software was used for analysis. The main outcome of interest was the difference between baseline and follow-up PFT measures. To control for the effect of height on lung function, the PFT measurements were standardised to an average height by multiplying by an adjustment factor (1.692/ht2).3 Unadjusted differences in characteristics between the TB and non-TB groups were expressed as the difference between means for numerical variables and ORs for categorical variables. Multivariable linear regression was used to test the mean differences between the TB and non-TB groups in change in lung function as the outcome variable adjusting for covariates. These covariates included lung function and silicosis at baseline and age, history of asthma, bronchitis or pneumonia, employment duration and current smoking (current vs past or never) at follow-up. Residuals were inspected to confirm that the error terms were independent with respect to each covariate and normally distributed around zero.
Results
Cohort characteristics
A total of 27 660 miners underwent a PFT during the baseline period. Of these, 5683 were still employed on 12 December 1999 and eligible for inclusion into the study. The mine's TB database showed that 270 of these miners experienced pulmonary TB following the baseline PFT; 185 were enrolled in the study. Among the 85 miners excluded, the most common reasons were termination of employment for reasons other than health (n=34), determination that they did not have TB (n=14) or the occurrence of two episodes of TB during the study period (n=11). The unexposed group constituted 185 age-matched participants (figure 2).

{kind=link}
{kind=link}
Selection of study participants. TB, tuberculosis.
Descriptive characteristics of the TB and non-TB groups are shown in tables 1 and 2. There were no significant differences between the groups in baseline PFT and age or employment duration at follow-up. The prevalence of silicosis was greater among miners diagnosed with TB, as was a history of asthma. The odds of being a current smoker were twice as great among the TB group. In both groups approximately 90% of the subjects worked underground; during the study six miners (four TB cases, two non-TB participants) were transferred to surface work.
Cohort characteristics (n=370)*
Pulmonary function* characteristics of cohort (n=370)†
Loss of lung function (unadjusted)
At baseline the two groups had similar height-adjusted mean FEV1 and FVC values (table 2). Both groups experienced significant decline over the follow-up period. The non-TB group had a mean decline in FEV1 of 72.2 ml/year over an average of 4.7 years and the TB group had a significantly greater mean decline of 119.3 ml/year over an average of 4.5 years, a difference of 47.1 ml/year (95% CI 32.4 to 61.9). For FVC, the mean decline in the non-TB group was 9.7 ml/year compared with 56.1 ml/year in the TB group, a difference of 46.4 ml/year (95% CI 30.9 to 61.9).
Clinical characteristics of TB group
The clinical features of the subjects with TB are shown in table 3. The majority of the TB episodes were either smear or culture positive or both at diagnosis (72.9%, 77.3% and 59.4%, respectively), and a little more than half were diagnosed through the mine's radiological screening programme.
Clinical characteristics of participants diagnosed with tuberculosis (TB) (n=185)
Multivariable regression
Multivariable linear regression was used to determine whether occurrence of TB was associated with excess decline in lung function after adjustment for potential confounders (table 4). Even after adjustment the occurrence of TB during the study period was significantly associated with excess decline in lung function. Relative to the non-TB group, the TB group experienced an adjusted mean excess loss of 40.3 ml/year in FEV1 and 42.7 ml/year in FVC.
Association between lung function decline and TB adjusting for covariates (n=370)
These findings were robust when tested in alternative models (table 4). Exclusion of history of bronchitis, asthma or pneumonia from the model, on the grounds that some of this history may have been TB related, resulted in slightly greater mean excess losses (46.0 ml/year in FEV1 and 46.9 ml/year in FVC). In addition to the 47 TB cases with known previous TB, nine of non-TB group reported previous TB not documented in the database. Exclusion of all participants with a previous history of TB as a potential confounder reduced the mean excess loss in FEV1 to 35.4 ml/year with no change in FVC.
All lung function tracings were reviewed at the time of data analysis. Of 370 subjects, 59 (16%) were identified in whom the highest two FVC or FEV1 readings were more than 200 ml apart, contrary to ATS recommendations.20 When the analysis was repeated without these participants, the mean excess losses were slightly greater.
The association between selected TB clinical variables and loss of lung function was evaluated separately in the TB group (table 5). In this group, extensive radiological change at diagnosis predicted a mean loss in FEV1 of 63.5 ml/year and a much smaller loss in FVC of 27.4 ml/year, adjusting for the other clinical predictors. Covariate variables associated with excess mean lung function loss in both FEV1 and FVC were sputum smear positive status and self-presentation at the mine hospital (as opposed to detection by routine radiological screening). HIV status at the time of TB diagnosis was not associated with loss of lung function.
Association between lung function decline and TB clinical characteristics among TB cases* (n=185)
TB and persistent respiratory symptoms
The persistence of symptoms related to an episode of treated TB is of interest. After controlling for baseline silicosis status, duration of follow-up, employment duration, age and current smoking status, the odds of cough, breathlessness and wheezing were all increased in the TB group (table 6, model 1). Further adjustment for a history of bronchitis, asthma or pneumonia significantly attenuated the ORs for all the symptoms, with breathlessness retaining the strongest association with TB (table 6, model 2).
Association between respiratory symptoms at follow-up and TB (n=370)
Discussion
The association between pulmonary TB and reduced lung function has been reported in a number of settings.1–7 To our knowledge, this study is the first to quantify lung function in the same participants both before and after the occurrence of pulmonary TB.
After controlling for other variables associated with lung function loss, the occurrence of TB during the study period was significantly associated with excess decreases in both FEV1 and FVC. With expected annual absolute declines in FEV1 of about 30 ml/year,21 both the TB and non-TB groups experienced abnormally high FEV1 declines (119.3 and 72.2 ml/year, respectively). Given the relatively low tobacco consumption in the black miner population,22 silica dust exposure and silicosis are more likely explanations of this excessive decline in FEV1 in both groups.7 15 However, the greater decline in the TB group indicates additional lung damage due to pulmonary TB, with a clinically relevant associated loss of approximately 40 ml/year in FEV1 and 43 ml/year in FVC. This is consistent with the finding that TB cases had more than double the odds of breathlessness at follow-up.
Our results build on previous studies. This study found little difference between FEV1 and FVC loss attributable to TB. This contrasts with a net obstructive effect noted in other studies of gold miners,3 7 although even in those studies the loss in FVC attributable to TB was substantial. Clinical studies2 23 suggest that FEV1 and FVC are significantly reduced at the time of TB diagnosis but improve by the end of short course therapy, with FVC recovering more than FEV1.2 Hnizdo3 was able to investigate the effect of time since treatment and found that both FEV1 and FVC improved during the first year with the excess loss stabilising thereafter. Hnizdo's results also suggest that the net obstructive effect may increase with time. In summary, it is likely that there is differential recovery in FEV1 and FVC during treatment and in the first year or so thereafter which would explain some of the differences between studies with varying follow-up times. This study was not able to show a difference in loss by time since TB diagnosis.
It is unsurprising that subjects with TB with more extensive radiological disease at diagnosis incur greater residual lung change and lung function loss at the end of treatment resulting in permanent loss despite bacteriological cure.1 2 An interesting finding was that sputum smear positive status and, to a lesser extent, detection through self-presentation were significantly associated with excess lung function decline after controlling for extent of radiological change at diagnosis. Detection through self-presentation as opposed to screening can be regarded as a proxy for later diagnosis, while sputum positive cases may have more cavitary disease than smear negative cases23 and thus reflect more severe disease. Finally, the excess in respiratory symptoms among treated TB cases is additional evidence that pulmonary TB may impair health and well-being regardless of treatment outcome.
The study has certain limitations. Since a large proportion of miners who underwent a baseline PFT were no longer employed at the time of the follow-up PFT (figure 2), a ‘healthy survivor’ effect may have resulted in an underestimate of lung function loss due to TB. Another limitation was that the baseline PFT was recorded on average 2.25 years before TB diagnosis which would contribute ‘unexposed’ person-time to the TB group. As a result, the estimate of excess yearly lung function decline due to TB is likely to be further underestimated.
There is always the potential for error when lung function testing is performed at different times and under different conditions. Quality control measures were in place during both routine (baseline) and research (follow-up) phases, and the intrasubject reliability over time during the baseline phase has been previously confirmed.16 Nevertheless, reproducibility of expiratory efforts did not meet the ATS criteria20 in a number of cases. Although there was no effect on the results when these records were removed from the analysis, it is possible, for example, that better expiratory efforts at follow-up than at baseline might have resulted in an underestimate of lung function loss. This would be more the case for FVC than FEV1 because early termination of expiration is a more likely shortcoming in mass screening.
HIV infection, which has been shown to be associated with lung function loss in a North American veteran cohort,24 was tested only in the TB group and could therefore not be analysed as a confounder in the full analysis. However, in the TB group, HIV infection had no influence on lung function loss. It is also likely that in this population a major part of an HIV effect on lung function would be mediated via TB.
Although radiological silicosis and duration of mining exposure were controlled for as potential confounders in the analysis, it is possible that there remains some degree of confounding by sub-radiological silicosis and cumulative silica dust exposure. A more than additive interaction between silica dust, silicosis and TB on lung function is also possible but would be difficult to observe in a sample of this size. Miners with both silicosis and TB are also more likely to be selected out of employment than those with one disease alone.
Conclusions
The results have implications for understanding and managing pulmonary TB among miners in the South African gold mines and in comparable populations. An episode of pulmonary TB, even if fully treated, should be regarded not as a discrete illness but rather as an event with long-term respiratory effects. This and other studies show that the excess loss persists over several years. Longer term studies are needed to determine the effect over a longer period (ie, ≥10 years).
Additionally, we found independent associations between excess decline in FEV1 and FVC and radiological abnormality at diagnosis, sputum smear positive status and self-presentation at the mine hospital as opposed to detection by screening. While early detection and treatment are central to all TB control strategies, this study implies further that, besides reducing the pool of infectious people, early intervention would reduce chronic respiratory impairment among those successfully treated.
In the South African gold mining industry with its high prevalence of dust disease, TB prevention requires more than early detection. Control of silica dust should be an explicit goal of any TB control programme.25 The use of isoniazid preventive therapy to reduce the risk of TB should also be considered. Targeting preventive therapy at miners with silicosis or HIV infection could reduce the risk of developing TB by more than half, for example.26 27 Finally, ongoing education is needed to increase worker awareness of TB risk factors (dust, silicosis and HIV) as well as the personal health benefits of early detection.
Acknowledgments
We would like to thank Sr B Magadla and Mr I Mantsoe for conducting the respiratory questionnaires and performing the spirometry, radiographic reading preparation and data entry. Dr J Smith (AngloGold Health Services, Free State) was the co-reader for the TB films. Mr P Heselman assisted with the ILO grading of the miniature chest radiographs. Funding from the Safety in Mines Research Advisory Committee (SIMRAC; now Mine Health and Safety Council) to undertake this project is gratefully acknowledged.
References
Footnotes
N White died on 6 November, 2004.
Funding Mine Health and Safety Council, South Africa.
Competing interests RIE has written expert reports for use in silicosis litigation. GJC was employed by the AngloGold Ashanti gold mining company at the time of the study. The remaining authors have no competing interests.
Ethics approval This study was conducted with the approval of the AngloGold Health Services Medical Research Ethics Committee and the University of the Witwatersrand Committee for Research on Human Subjects and all participants gave written informed consent.
Provenance and peer review Not commissioned; externally peer reviewed.