Article Text

Statistics from Altmetric.com
A 55-year-old Caucasian man who worked in the recycling industry presented with a 7-month history of non-productive cough and no other symptoms. He had no significant previous medical history and took no medications. He had never smoked and had no history of travel outside the UK. He described symptoms of a lower respiratory tract infection 5 months previously which had been treated with antibiotics and steroids. A chest x-ray at the time had shown consolidation consistent with infection which had subsequently resolved. Physical examination was normal.
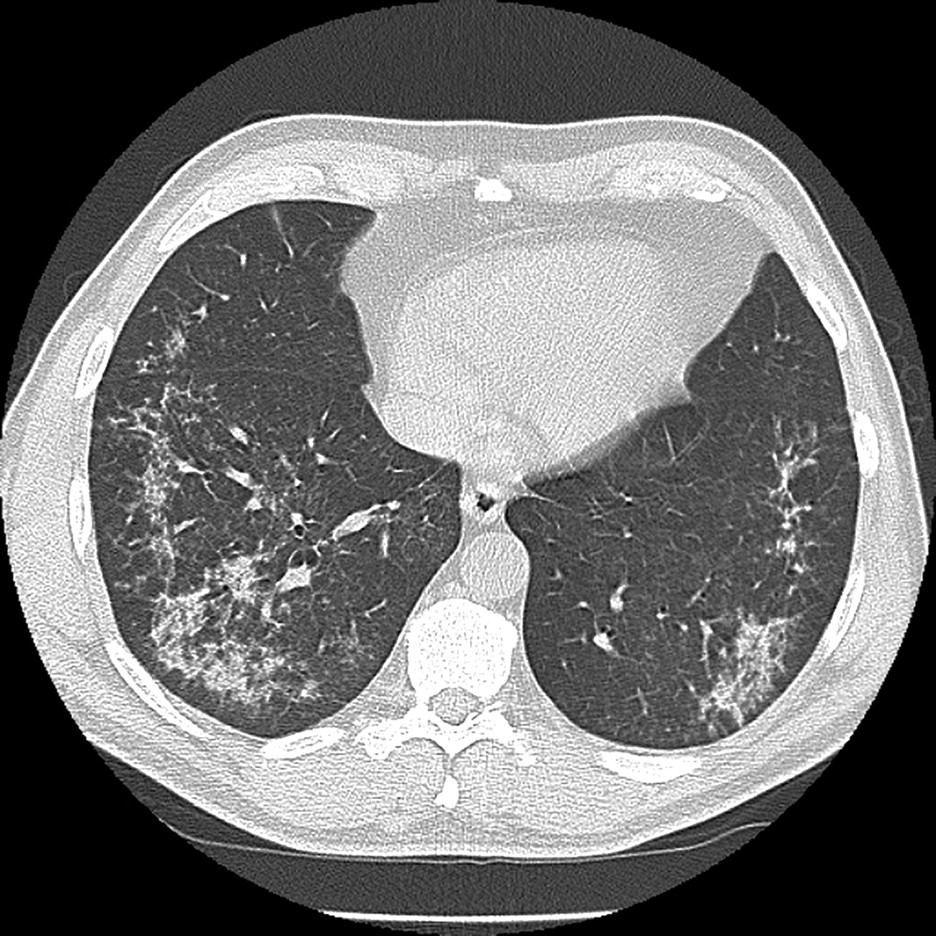
Spirometry and transfer factor were normal. Full blood count showed isolated eosinophilia of 12.7×10−9/l. The blood film revealed an unremarkable cell morphology. The erythrocyte sedimentation rate was elevated at 92 mm/h. Urea and electrolytes, liver function tests and serum immunoglobulin E (IgE) were normal. Aspergillus precipitins, antineutrophil cytoplasmic antibodies, rheumatoid factor and antinuclear antibodies were negative. Stool culture and microscopy were negative. A repeat chest x-ray was normal but a high-resolution CT scan showed bilateral patchy bronchocentric consolidation (figure 1) and mild splenomegaly. Bronchoscopy revealed no endobronchial abnormality with negative results for culture and cytology.

{kind=link}
High-resolution CT scan showing bilateral patchy bronchocentric consolidation.
The patient's cough became so debilitating that he was unable to work. His eosinophil count rose to 18×10−9/l and he was referred for haematology review. A bone marrow trephine was performed and peripheral blood was sent for cytogenetic testing which gave the diagnosis. Within 2 weeks of commencing treatment his cough had resolved and his eosinophil count was 0.
Question
What is the diagnosis and what treatment caused his dramatic clinical improvement?
See page 1024 for answer
Answer
From the question on page 1009
The combination of blood eosinophilia persisting for more than 6 months, end-organ damage as demonstrated by lung consolidation and an identified clonal chromosomal abnormality (ie, the FIP1L1/PDGFRA gene arrangement) fulfils the diagnostic criteria for chronic eosinophilic leukaemia (CEL).1 In the absence of clonal chromosomal abnormalities, our patient would fulfil the criteria for an idiopathic hypereosinophilic syndrome (HES). The lack of relevant travel history along with normal IgE excluded tropical pulmonary eosinophilia as the diagnosis.2
The FIP1L1-PDGFRA fusion protein is a constitutively activated tyrosine kinase3 which occurs due to a deletion on chromosome 4q12. Expression of FIP1L1-PDGFRA in haematopoietic progenitors induces cytokine-independent differentiation of several myeloid lineages, not just eosinophils. Murine studies show that overexpression of interleukin 5 (IL-5) in the presence of FIP1L1-PDGFRA is required to induce eosinophilic tissue infiltration,4 with studies of human CD34 cells further suggesting that IL-5 helps induce the phenotype but alone is insufficient to induce HES/CEL-like disease.5
Treatment was with the tyrosine kinase inhibitor imatinib. Fifteen-year survival in HES prior to imatinib was around 42%. However, imatinib has been shown to induce clinical, haematological and molecular remission in the majority of patients and it is anticipated that long-term survival will significantly improve.3
The mechanism for cough in CEL is unknown. We did not demonstrate eosinophilic lung infiltration (no bronchial biopsies or bronchoalveolar lavage were performed), but suggest that the pulmonary infiltrates seen on the CT scan represent eosinophilic infiltration. This would be consistent with a case of FIP1L1/PDGFRA-related disease who presented with cough,6 in whom CT scanning showed thickened airways and endobronchial biopsy showed eosinophilic inflammation. The patient also had normal spirometry and a negative histamine challenge test but a sensitive cough response to inhaled capsaicin. We hypothesise that eosinophils or their degranulation products are the cause of the cough, but further studies are required to elucidate exactly how eosinophils induce cough.
Footnotes
Competing interests None.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.