Article Text

Abstract
Background Statins have anti-inflammatory actions which in theory are potentially beneficial in asthma. Small trials have failed to show a significant benefit, but a systematic study to evaluate the steroid-sparing effect of statin treatment has not been carried out.
Methods A randomised, placebo-controlled, crossover trial was conducted of simvastatin 40 mg at night with simultaneous stepwise reduction of fluticasone propionate dose until loss of control occurred, followed by an increase until regain of control (‘minimum’ dose required) in 51 patients with asthma and sputum eosinophils (steroid-free) ≥2%.
Results 43 patients completed the study. There was no significant difference in ‘minimum’ inhaled corticosteroid (ICS) dose requirement between simvastatin and placebo: (median (IQR) 50 μg daily (0–250) vs 100 μg daily (0–250), p=0.931). ‘Minimum’ dose distribution was similar (p=0.269). The fluticasone dose at which loss of control occurred did not differ significantly between simvastatin and placebo (p=0.404). In patients with loss of control in both treatment arms, fluticasone dose at loss of control was similar with simvastatin and placebo (median (IQR) 50 μg daily (0–100) for both, p=0.620). In those patients who reached 0 μg/day (n=18), Astma Control Questionnaire (ACQ) was lower (p=0.037), forced expiratory volume in 1 s (FEV1) higher (p<0.01) and sputum eosinophils lower with simvastatin compared with placebo (9.5% compared with 25.4%, p=0.033).
Conclusions Simvastatin does not have clinically important steroid-sparing effects in patients with eosinophilic asthma. In the absence of steroid, simvastatin is associated with minor improvements in symptoms and lung function, and a reduction in sputum eosinophils.
Clinical trial number ACTRN12606000531516.
- Asthma
- eosinophil
- phenotype
- simvastatin
- asthma pharmacology
Statistics from Altmetric.com
Introduction
Statins have anti-inflammatory as well as cholesterol-lowering effects.1 They may be beneficial in cardiovascular disease,2 multiple sclerosis3 and rheumatoid arthritis.4 In chronic obstructive pulmonary disease (COPD),5 their use is associated with reduced decline in lung function,6 improved survival following exacerbations7 and increased exercise capacity.8
In asthma, there are theoretical reasons why statins might exert therapeutic effects. Their actions include reducing both T cell proliferation and activation, and leucocyte migration.9 In animal models, statins inhibit eosinophilic infiltration into the lung,10 11 reduce airway hyper-responsiveness (AHR)12 and reverse impaired β-adrenoceptor responsiveness induced by airway inflammation.13 In human tissue, statins reduce mast cell degranulation,14 enhance inflammatory cell apoptosis15 and inhibit airway smooth muscle proliferation.16
To our knowledge, only two clinical studies investigating statins in asthma have been published.17 18 The scope of these was limited. The first was of short duration (1 month), with a small number of patients (n=16).17 In the second, inhaled corticosteroid (ICS) treatment was continued, and anti-inflammatory and steroid-sparing effects may have been masked.18
Our aim was to assess the steroid-sparing effects of simvastatin in patients with asthma. Our hypothesis was that with simvastatin, patients would require lower doses of ICS to maintain control. We conducted a randomised, double-blind, placebo-controlled, crossover study of simvastatin in which down-titration of ICS treatment was systematically undertaken.
Methods
See also the Online repository.
Patients
Patients with stable persistent asthma were enrolled. Exclusion criteria are given in the Online repository.
Phase1
All patients completed a 2-week run-in on regular medications, then ICS treatment was withdrawn until loss of control (LOC) or 28 days. This was followed by an open-label trial of inhaled fluticasone (1000 μg daily for ≥28 days). The aim of Phase 1 was to define the off-steroid inflammatory cell phenotype and the magnitude of steroid responsiveness. For further details. see Cowan et al.19
Phase 2
Patients proceeded to randomisation if, off steroid, they demonstrated one of the following: a provocation dose of hypertonic saline causing a 15% fall in forced expiratory volume in 1 s (FEV1) (PD15) of <12 ml20; a provocation dose of methacholine causing a 20% fall in FEV1 (PD20) of <8 μmol 21; or an increase in FEV1 postbronchodilator ≥12%.22 All randomised patients had sputum eosinophilia ≥2% 23: non-eosinophilic patients were excluded.
Study design
This was a randomised, double-blind, placebo-controlled, crossover trial of simvastatin, with stepwise down-titration of ICS dose during each treatment arm. Patients took a capsule containing either active drug (simvastatin 40 mg; Lipex, Merck Sharp Dohme, Auckland, New Zealand) or matching placebo once daily at night. The investigators were blinded to treatment allocation. In addition, each month, patients were supplied with two inhalers (A and B) and took one puff of inhaler A in the morning and one puff of inhaler B in the evening. The ICS dose was blinded to the patient by coupling unlabelled inhaler sleeves with actuators containing fluticasone 50, 125 or 250 μg, or placebo (0 μg) (Flixotide, GlaxoSmithKline, Greenford, UK). Different A and B combinations provided for daily doses of 0, 50, 100, 250 or 500 μg.
Patients were commenced at a dose of fluticasone of 500 μg/day. If asthma was not controlled during the first month, the dose was stepped up to 1000 μg/day for 1 month before commencing down-titration. If asthma was controlled, patients were given the next treatment pack and returned a month later. The dose of fluticasone was then stepped down at monthly intervals until LOC based on a priori criteria 24 (figure 1). At LOC, or after 1 month taking 0 μg/day fluticasone, sputum induction and AMP challenge were performed. Patients with no LOC at 0 μg/day were crossed over to the alternative treatment and the sequence was repeated. Patients who experienced LOC then received fluticasone at a dose one step up from the one at which LOC had occurred. They were reviewed monthly with stepwise increases in fluticasone until control was regained (deemed to be the ‘minimum dose requirement’). Sputum induction and AMP challenge were repeated at the ‘minimum’ dose, and patients then proceeded to the alternative arm. Daytime symptoms, night waking, bronchodilator use and peak flows were recorded daily.

Protocol for the first arm of study (second arm identical). Patients were randomised to either simvastatin 40 mg at night or placebo during the first arm, and were crossed over to receive the alternative treatment in the second arm. Monthly changes in daily fluticasone dose are shown in boxes. Subjects commenced on 500 μg daily, and stepwise reduction occurred each month until either loss of control (LOC) or 0 μg/day was reached. Sputum induction and AMP challenge were then performed. Subjects reaching 0 μg without LOC (‘minimum required’ dose = 0 μg/day) then proceeded to the second arm. Subjects with LOC were provided with the fluticasone dose one step up from that at which LOC occurred. They were reviewed monthly with stepwise increase in fluticasone dose each month until regain of control (ROC) occurred (‘minimum required’ dose), at which time sputum induction and AMP challenge were repeated before progressing to the second arm. *Criteria for loss of control were based on diary data and spirometry from the last 2 weeks of the Phase 1 trial of fluticasone. ACQ, Asthma Control Questionnaire; AQLQ, Asthma Quality of Lfe Questionnaire; FENO, fraction of exhaled nitric oxide; FEV1, forced expiratory volume in 1 s; ICS, inhaled corticosteroid (fluticasone).
Procedures at monthly reviews
Patients completed the Asthma Control Questionnaire (ACQ), Asthma Control Test (ACT) and Asthma Quality of Life Questionnaire (AQLQ) before having their fraction of exhaled nitric oxide (FENO) and spirometry measured.
Ethical and safety considerations
All patients gave written informed consent. Safety procedures, including adverse drug event monitoring, are documented in the Online repository. Ethical approval was obtained from the Lower South Regional Ethics Committee, New Zealand.
This study was registered with the Australian New Zealand Clinical Trials Registry (ACTRN12606000531516).
Study size and statistical analyses (see Online repository)
The primary end point was ‘minimum’ ICS dose requirement. Secondary end points were ICS dose at LOC, and number of patients without LOC after ICS withdrawal. Based on previous data,25 and using a SD of 200 μg for mean daily fluticasone dose requirement, it was calculated that to demonstrate the superiority of simvastatin in reducing the ‘minimum’ dose requirement by 100 μg, 33 patients would be required (power=80%, α=0.05 and β=0.2). Additional patients were recruited to allow for a drop-out rate of 25%. Paired survival analysis was used to compare the proportions of patients who reached LOC at each treatment step on simvastatin and placebo, using Cox proportional hazards regression clustered on the individual. Proportions with LOC on simvastatin and placebo were compared using McNemar test. ICS dose at LOC and ‘minimum’ ICS dose on simvastatin and placebo were compared using Wilcoxon signed rank sum tests. Other comparisons were made using paired t tests and Wilcoxon signed rank sum tests. For the purposes of the study, asthma control was deemed to be the absence of the criteria used to define LOC. Statistical correction for multiple comparisons was not undertaken and the possibility exists that some results occurred by chance despite a p value <0.05.
Results
Fifty-one subjects were randomised; 43 completed both treatment arms. Baseline characteristics are shown in table 1. There were eight withdrawals: three before commencing treatment (pregnancy, deranged liver function, withdrawal of consent); four during the simvastatin arm (muscle pain, rash, troublesome asthma, relocation); and one during the placebo arm (pregnancy). Data for these eight subjects were not analysed; their baseline characteristics did not differ from those who completed the study. Following the prerandomisation trial of fluticasone, as expected, there were significant changes for ACQ (mean (SD) −1.2 (0.9) points, p<0.001), FEV1 (mean (SD) +0.67 (0.41) litres, p<0.001) and PC20AMP (mean (SD) doubling dose increase 3.7 (2.8), p<0.001; table R1, Online repository).
Characteristics of study participants at study entry
LOC during stepwise ICS dose reduction
With down-titration, the number of subjects who lost control at each treatment step did not differ significantly between simvastatin and placebo (p=0.404; figure 2). LOC occurred in 26 subjects (60%) during both simvastatin and placebo arms, in 3 (7%) during the simvastatin arm only, and in 6 (14%) during the placebo arm only. There was no order effect. In 8 (19%), LOC did not occur in either arm (p=0.508), and thus for this subgroup, ‘minimum’ ICS dose was 0 μg/day with both simvastatin and placebo. In patients with LOC during both treatment arms (n=26), the fluticasone dose at LOC was not significantly different between the simvastatin and placebo arms; median (IQR) for both, 50 μg/day (0–100) (p=0.620).
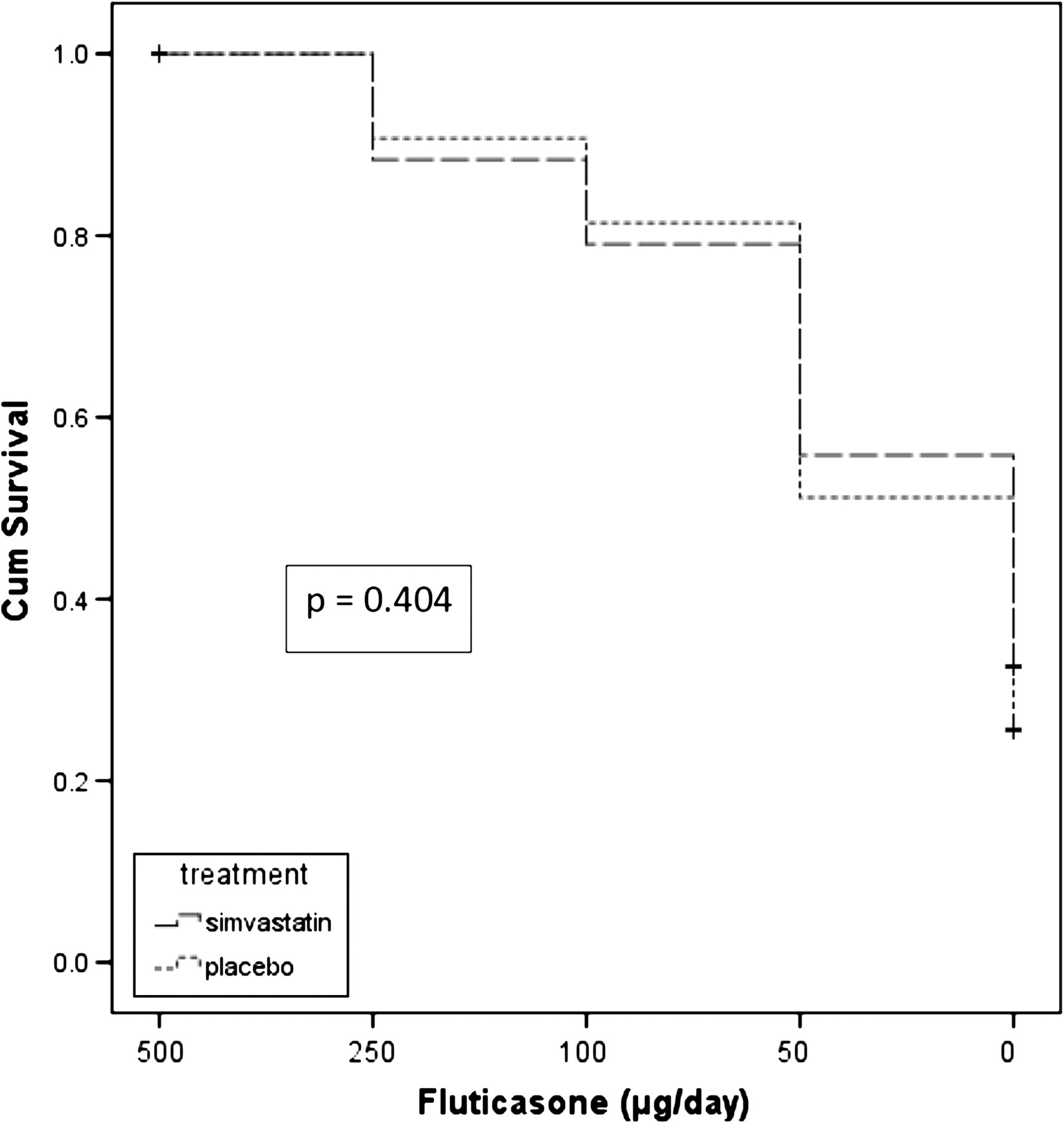
Kaplan–Meier plot showing the number of subjects without loss of control at each fluticasone dose during monthly stepwise dose reduction from 500 μg/day to 0 μg/day with simvastatin and placebo. There was no significant difference between simvastatin and placebo (p=0.404).
‘Minimum’ fluticasone dose and asthma control
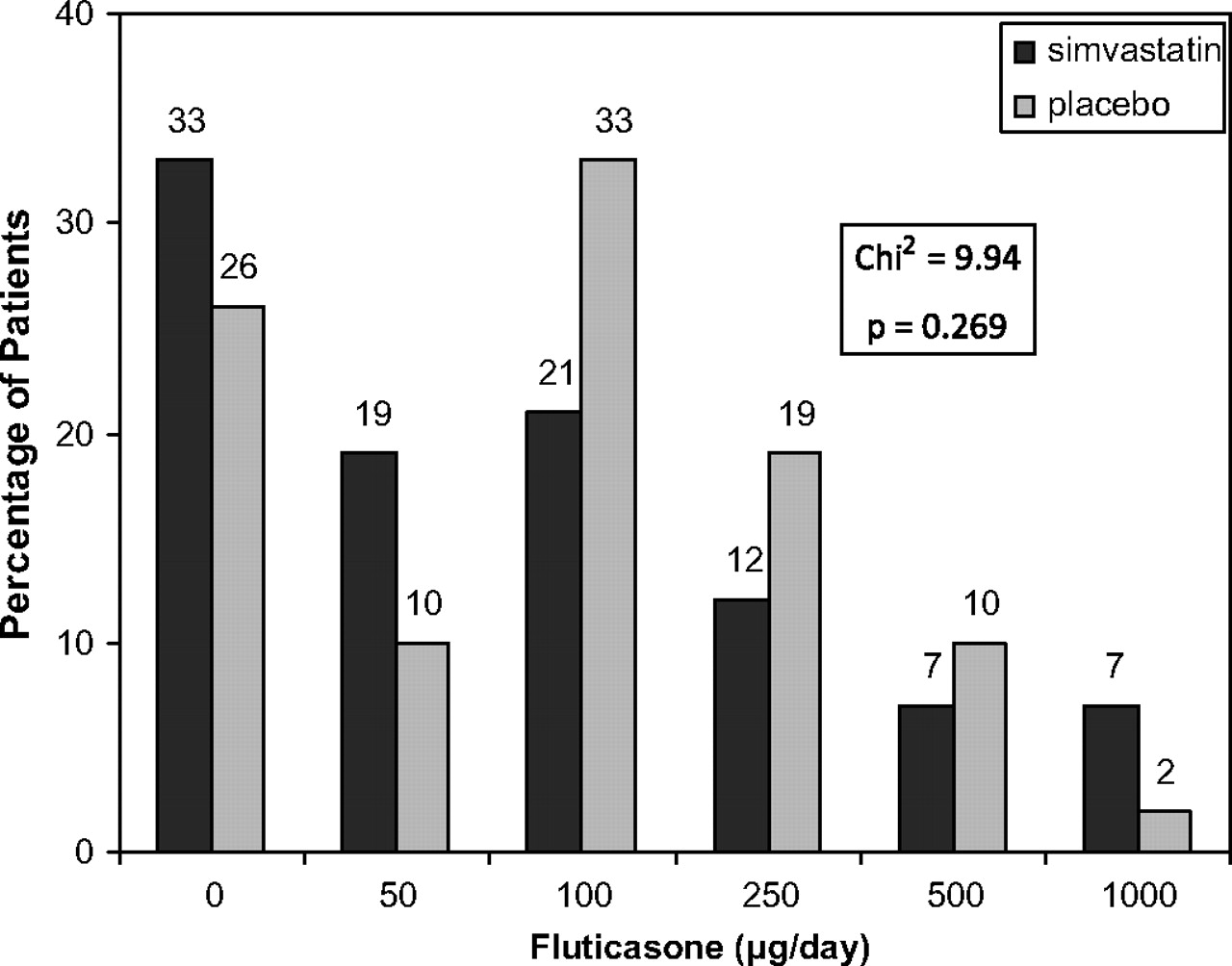
At ‘minimum’ fluticasone dose, ACQ was similar with both simvastatin and placebo (median (IQR) 0.3 (0.0–1.1) and 0.7 (0.3–1.2), respectively, p=0.171) (table 2). There was no significant difference in the ‘minimum’ fluticasone dose between the simvastatin and placebo arms; median (IQR) 50 μg/day (0–250) and 100 μg/day (0–250), respectively (p=0.931). The distribution of ‘minimum’ doses with simvastatin or placebo did not differ significantly (χ2 = 9.94, p=0.269; figure 3). Similarly, ACT, AQLQ, FEV1 and AHR were not significantly different between treatment arms at ‘minimum’ fluticasone dose (table 2). However, at ‘minimum’ dose, sputum eosinophils were lower (median (IQR) 9.9% (5.7–27.0) vs 22.7% (13.4–37.8), p=0.047) with simvastatin than placebo. None of the mediators in sputum supernatant differed significantly between the two treatment arms (table R2, Online repository).
Comparison of symptoms (ACQ, ACT), quality of life (AQLQ), bronchodilator use, lung function (PEF and FEV1), airway hyper-responsiveness (PC20AMP) and airway inflammation (FENO and sputum cells) in all patients at ‘minimum’ dose while taking concomitant simvastatin 40 mg at night or placebo
{kind=link}
{kind=link}
{kind=link}
Number of patients (%) whose ‘minimum’ maintenance dose of inhaled fluticasone was 0, 50, 100, 250, 500 and 1000 μg/day while taking simvastatin 40 mg at nightor placebo.
Comparisons at each fluticasone dose step
Paired data were available at each fluticasone dose as follows: 500 μg, n=43; 250 μg, n=43; 100 μg, n=36; 50 μg, n=30; 0 μg, n=18 (table 3). At 500 μg, morning peak expiratory flow (PEF) was significantly higher on placebo than on simvastatin (p=0.007). At 0 μg/day, ACQ was significantly lower (p=0.037), and both prebronchodilator and postbronchodilator FEV1 were significantly higher on simvastatin than on placebo (p<0.001 and p<0.01, respectively). No other significant differences were seen.
Measures of asthma control during stepwise reduction in ICS dose while taking simvastatin and placebo
AHR, sputum cells and cytokines
In the subgroup who were down-titrated to 0 μg fluticasone (n=18, of whom 8 did not experience LOC), PC20AMP was similar with both simvastatin and placebo (table 4). Sputum eosinophils were significantly lower (p=0.033) and lymphocytes significantly higher (p=0.003) with simvastatin. There were no significant differences in any of the sputum mediators between simvastatin and placebo (table R3, Online repository).
Comparison of airway hyper-responsiveness (PC20AMP) and sputum cells at 0 μg fluticasone daily in the subgroup (n=18) reaching this dose after stepwise reduction while taking concomitant simvastatin 40 mg at night or placebo
Discussion
This is the first study to assess the steroid-sparing effects of simvastatin in patients with eosinophilic, steroid-responsive asthma. Our principal finding was that simvastatin was not associated with a clinically important steroid-sparing effect. The ‘minimum’ steroid dose required to establish asthma control was the same whether taking simvastatin or placebo. Similarly, the dose at which LOC occurred following steroid reduction was comparable in both treatment arms, and in patients who experienced LOC in both arms, the steroid dose at which it occurred was no different.
In patients in whom steroid treatment was reduced to 0 μg/day (n=18, of whom 10 lost control), simvastatin was associated with minor improvements in ACQ and FEV1 (table 3). Simultaneously, sputum eosinophils were reduced with simvastatin (from 25.4% to 9.5%, p=0.033). In all patients, when taking their ‘minimum required’ fluticasone dose, sputum eosinophils were significantly lower with simvastatin (9.9% vs 22.7%, p=0.047), despite the fact that the mean ‘minimum’ dose was almost identical (168 vs 157 μg/day). Taken together, these data suggest that although an anti-inflammatory effect may occur with simvastatin, it was insufficient to have any significant impact on steroid requirements. Our data pertaining to sputum eosinophilia are in keeping with animal-based studies10 11 which showed reduced eosinophils after allergen challenge in statin-treated mice.
Despite a reduction in sputum eosinophils with simvastatin, there were no differences in AHR or sputum mediators (interleukin 4 (IL-4), IL-5 or eotaxin). The dissociation between changes in inflammatory cells versus AHR and symptoms has been reported with anti-IL-5 treatment.26 In an in vitro study of eosinophils from patients with asthma, simvastatin induces apoptosis,27 and lovastatin enhances phagocytic clearance of apoptotic cells.15 Thus the reduction in sputum eosinophils with simvastatin may result from apoptosis induction and/or increased eosinophil clearance.
At ‘minimum required’ fluticasone dose, sputum eosinophils remained increased. Despite unresolved sputum eosinophilia, the median ACQ was 0.3 with simvastatin and 0.7 with placebo (non-significant), indicating adequate asthma control.28 Changes in sputum eosinophils may be out of phase with asthma control by up to 20 days.29 In addition, steroid withdrawal may result in ‘rebound’ eosinophilia.30 These phenomena may explain why sputum eosinophils remained elevated at ‘minimum’ dose, yet with relative suppression of eosinophils with simvastatin compared with placebo.
Non-eosinophilic patients were excluded so that the effect of treatment specifically on the eosinophilic phenotype could be assessed. We avoided recruiting ‘all-comers’ in whom treatment response is more likely to be variable.31 Asthma is pathologically heterogeneous, as is the response to disease-modifying treatments. Ideally clinical trials should include patients with a similar pathological phenotype. This is illustrated in studies of the anti-IL-5 antibody, mepolizumab.26 32 33 Whereas outcomes in unselected patients were disappointing,33 in later studies patients with an eosinophilic phenotype were selected26 32 and positive outcomes were achieved, indicating that matching treatment to phenotype is important. Further studies are needed to investigate the effects of statins in non-eosinophilic asthma in the light of promising outcomes in COPD.5–7 34 35
There are only two clinical studies that have previously assessed statins in asthma.17 18 In the first small study (n=16),17 simvastatin was given for 4 weeks. In the second18 (n=54), atorvastain (40 mg daily) was administered for 8 weeks, but regular ICS treatment was continued. Neither study demonstrated important differences between statin and placebo for symptoms, spirometry or AHR, although sputum leukotriene B4 and macrophages decreased significantly with atorvastatin.18 However, there are weaknesses in their design. First, treatment duration was relatively short.17 In our study, length of treatment depended on when/whether a patient reached LOC, but all received a minimum of 3 months treatment. Secondly the study by Menzies et al17 was, by the authors' own admission, underpowered to detect changes in airway inflammation. Thirdly, in the study by Hothersall et al,18 patients continued ICS throughout, and masking of any anti-inflammatory effect of statin was therefore possible. In the Menzies study,17 even after ICS withdrawal, the sputum eosinophil count was 2%, suggesting minimal eosinophilic airway inflammation. By recruiting a broad spectrum of patients, neither study was designed to evaluate statin treatment in specific inflammatory phenotypes.
We used simvastatin at a dose of 40 mg daily. Data from several studies supported the selection of simvastatin as the trial drug. In murine models, simvastatin reduces eosinophilic inflammation10 12 and AHR,12 while in vitro human studies indicate that simvastatin induces eosinophil apoptosis27 and inhibits proliferation of airway smooth muscle cells.16 The choice of dose (40 mg daily) was based on data demonstrating anti-inflammatory effects (reduced serum IL-6, IL-8 and monocyte chemoattractant protein-1) at this dose.36 We cannot exclude that lack of clinical effect may be because the dose of simvastatin was too low.
A subgroup of patients had no LOC after ICS withdrawal: this occurred in 8 (19%) in both treatment arms, in 6 (14%) with simvastatin and 3 (7%) with placebo; their ‘minimum’ ICS dose requirement was 0 μg/day. Arguably, the inclusion of patients with mild asthma may have reduced the potential to show a treatment effect. However, at the study outset, of 43 patients who were enrolled, 42 (98%) were taking regular ICS and 17 (40%) were also taking a regular long-acting β-agonist. Moreover, after ICS withdrawal in Phase 1, 36 (84%) demonstrated LOC, indicating that they were ‘steroid requiring’. The duration of each step during ICS dose reduction was 1 month. If the interval between adjustments had been longer, LOC may have occurred in these patients, and consequently the calculated ‘minimum dose’ requirement would have been higher. Reassuringly, a posthoc analysis of patients who experienced LOC during ICS reduction (n=36, 84%) revealed no significant difference between simvastatin and placebo (Online repository: figure R1).
In conclusion, our results suggest that statin treatment is unlikely to be beneficial in managing specifically eosinophilic asthma. No clinically important steroid-sparing effects were demonstrated. In the absence of steroid, simvastatin is associated with minor improvements in symptoms and lung function, together with reduced sputum eosinophils, the relevance of which is unclear. Given the apparent benefits of statin treatment reported in epidemiological studies of COPD, it may be that in other airways disease phenotypes, statins may have a role.
Acknowledgments
We thank Ms Sarah Featherston for her administrative support, Dr Sarah Young for her expertise in measurement of sputum supernatant fluid mediators, and Professor G. Peter Herbison and Dr Erik Landhuis for their statistical advice. We are grateful to Professor Louis-Philippe Boulet who provided helpful comments on this manuscript.
References
Supplementary materials
Web Only Data thx.2010.138990
Files in this Data Supplement:
Footnotes
Funding Lottery Health New Zealand, the Asthma and Respiratory Foundation of New Zealand and the Dean of the Dunedin School of Medicine (Distinguished Researcher Award).
Competing interests None.
Patient consent Obtained.
Ethics approval This study was conducted with the approval of the Lower South Island Ethics Committee, New Zealand.
Provenance and peer review Not commissioned; externally peer reviewed.