Article Text

Statistics from Altmetric.com
S117 EGFR AND KRAS MUTATION ANALYSIS BY ENDOBRONCHIAL ULTRASOUND-GUIDED TRANSBRONCHIAL NEEDLE ASPIRATION IN NSCLC
1G. Santis, 2R. Breen, 2A. Quinn, 2E. McLean, 2K. Tobal. 1Kings College London, London, UK, 2Guy’s & St Thomas NHS Foundation Trust, London, UK
Introduction Somatic mutations in the epidermal growth factor receptor (EGFR) are associated with significant clinical responses to tyrosine kinase inhibitors (TKIs) in patients with non-small cell lung cancer (NSCLC). Somatic mutations in the KRAS gene that encodes a signalling protein activated by EGFR are also found at high rates in NSCLC. KRAS mutations confer primary resistance to EGFR-TKIs, irrespective of EGFR mutation status. Endobronchial ultrasound (EBUS)-guided transbronchial needle aspiration (TBNA) of mediastinal and hilar lymph nodes is being increasingly used in the diagnosis and staging of lung cancer.
Objectives The purpose of this study was to assess the feasibility of detecting EGFR and KRAS mutations in samples obtained by EBUS-TBNA.
Methods EBUS-TBNA samples were obtained via a 22 g needle placed under suction. A Consultant Cytopathologist immediately examined the obtained samples on-site to ensure adequacy of sampling for histological diagnosis. Mutation analysis was performed by “cold” PCR to amplify exons 18, 19, 20 and 21 for the EGFR gene and the regions surrounding codons 12, 13, 59 and 61 for the KRAS gene, followed by direct sequencing of these amplicons. “Cold” PCR enables the preferential amplification of mutant alleles, as compared with normal PCR.
Results Mutation analysis has thus far been performed in 17 consecutive patients with NSCLC (10 females/7 males] with confirmed lymph node metastases (9/17 (53%) adenocarcinoma; 6/17 (35%) squamous cell; 2/17 (12%) poorly differentiated). EGFR mutations were detected in 4/17 samples (24%). Three mutations were in adenocarcinoma subtype and one in poorly differentiated NSCLC (TTF-1, CK5, CK7, CK20, p63 negative by immunohistochemistry). There were three point mutations (two in exon 21, one in exon 20) and one in-frame 15 bp deletion in exon 19. KRAS point mutations at codon 12 and 61, respectively, were identified in 2/17 patients (12%) (1 adenocarcinoma and 1 squamous cell histology). KRAS mutations were identified in samples with the wild-type EGFR sequence.
Conclusion EGFR and KRAS mutation analysis can be successfully performed in metastatic lymph nodes sampled by EBUS-TBNA. The results of the present study have important implications for patient selection for EGFR-TKI therapy in NSCLC.
S118 CHEMOKINE RECEPTOR EXPRESSION IN TUMOUR ISLETS AND STROMA IN NON-SMALL CELL LUNG CANCER
C. M. Ohri, A. Shikotra, R. H. Green, D. A. Waller, P. Bradding. Institute for Lung Health, Glenfield Hospital, Leicester, UK
Introduction Increased numbers of macrophages in tumour islets of patients with non-small cell lung cancer (NSCLC) are associated with extended survival. This study investigated the association between the microlocalisation of chemokine receptors in tumour islets and stroma with macrophage density and patient survival in NSCLC.
Methods We used immunohistochemistry to identify cells expressing CXCR1, CXCR2, CXCR3, CXCR4, CXCR5 and CCR1 in tumour islets and stroma in 20 patients with surgically resected NSCLC. Cell counts were correlated with survival and macrophage expression. The patients were divided into 10 patients with extended survival (ES) and 10 patients with poor survival (PS).
Results The mean survival was 90.8 months for the ES group and 7.9 months for the PS group. There was increased expression of CXCR2, CXCR3 and CCR1 in the tumour islets of ES compared with PS patients (median 6.5 vs 2.6 (p = 0.007), 12.7 vs 3.2 (p = 0.01) and 24.3 vs 2.4 cells/mm2 (p = 0.002), respectively). There was greater expression of CXCR2, CXCR3 and CXCR4 in the stroma of ES compared with PS patients (median 8.9 vs 1.6 (p = 0.04), 51.4 vs 5.9 (p<0.001), 24.9 vs 3.1 cells/mm2, (p = 0.004), respectively). There was a positive association between survival and tumour islet CXCR2 (p = 0.02), CXCR3 (p = 0.003) and CCR1 (p<0.001) density as well as between survival and stromal CXCR3 (p = 0.003) density. Chemokine receptor-expressing cell counts were correlated against islet and stromal macrophage counts and there were positive correlations for CXCR3 (rs = 0.520, p = 0.02) in the islets and negative correlations for CXCR2 (rs = −0.455, p = 0.04), CXCR3 (rs = −0.844, p<0.001) and CXCR4 (rs = −0.606, p = 0.005) in the stroma. Kaplan–Meier survival curves demonstrated that patients with above median expression of CXCR2, CXCR3 and CCR1 in their tumour islets had increased 5-year survival.
Conclusions Above median expression of CXCR2, CXCR3 and CCR1 in the tumour islets is associated with increased 5-year survival. Increased expression of CXCR3 correlates with increased macrophage expression in the tumour islets and therefore this receptor may be involved in the pathway that attracts cytotoxic M1 macrophages into the tumour islets.
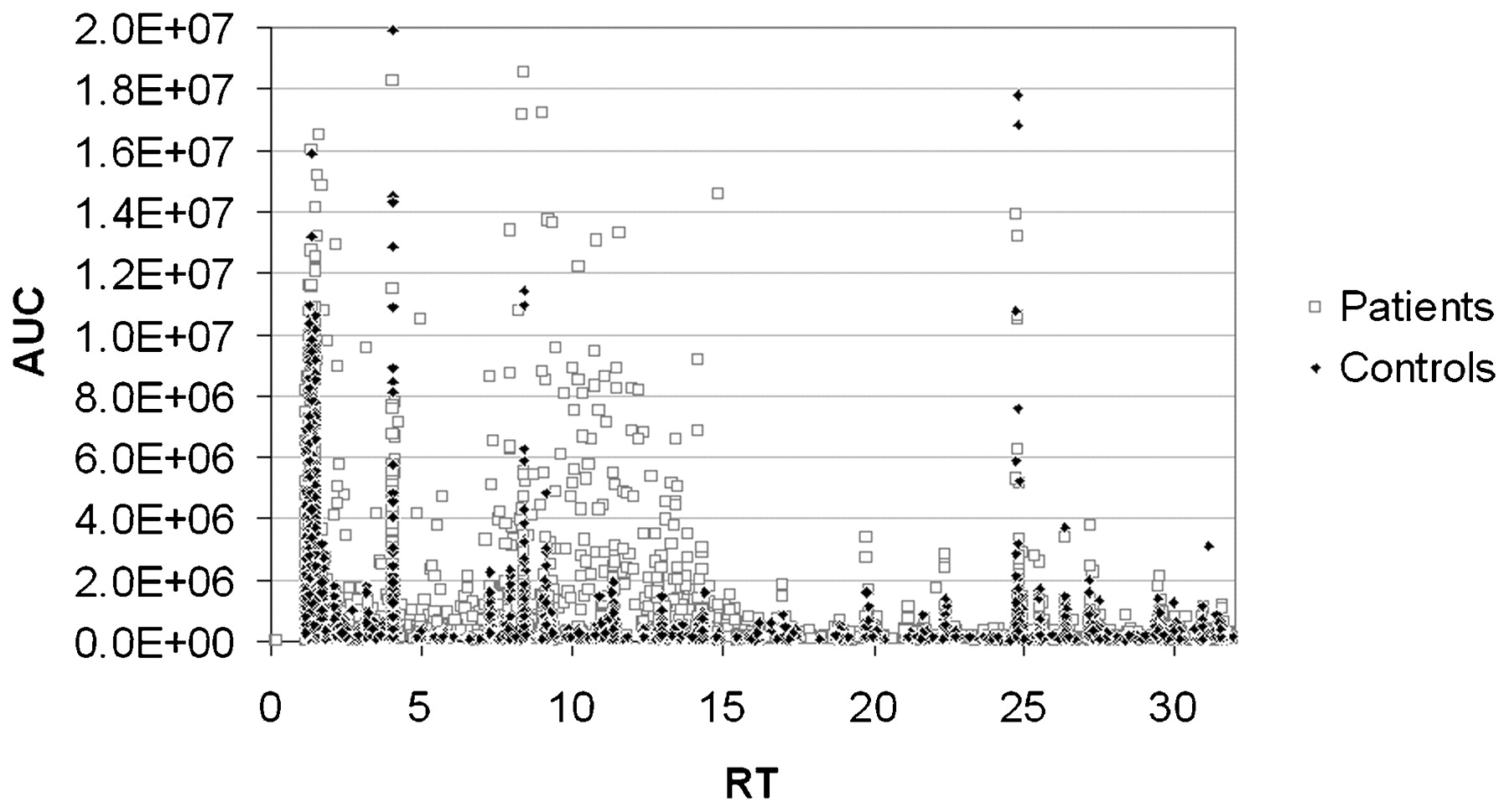
S119 DIFFERENCES IN PROFILES OF VOLATILE ORGANIC COMPOUNDS IN THE BREATH OF LUNG CANCER PATIENTS VS CONTROLS
1K. E. Lewis, 2C. O. Philips, 3H. Shukla, 1R. Ghosal, 3P. J. Kloer, 1J. G. Mullins, 2T. Claypole. 1Swansea School of Medicine, Swansea, UK, 2School of Printing and Engineering, Swansea University, Swansea, UK, 3Respiratory Unit, Prince Philip Hospital, Llanelli, UK
Introduction Studies have shown patterns of exhaled volatile organic compounds (VOCs) can differentiate patients with lung cancer (LC) from controls, with varying accuracy. Unlike previous work, we validated smoking status, standardised for effects of fasting, and applied novel metabolomic statistical approaches.
Methods A pilot observational study. 48 patients with LC (29 non-small cell lung cancer, 3 small-cell, 16 radiological/clinical diagnosis) and 50 healthy controls were fasted for 4 h, had exhaled CO recorded, then exhaled deeply into a Bio-VOC Breath Sampler (Markes International, UK) until their lungs were as empty as possible. The final 129 ml of trapped (alveolar) air sample was displaced (via a plunger) into a sorbent tube to trap the VOCs, and subsequently desorbed using a thermal desorption unit (Unity, Markes International). Samples were analysed by gas chromatography (Agilent Technologies 6890N) and mass spectrometry (5973 network mass selective detector). Automated detection calculated peak area and retention time for each compound and compared them with the NIST 98 mass spectral library, to identify the compounds. VOCs from simultaneous ambient air samples were subtracted from each sample.
Analysis Prior to full data mining, we applied constraining (polynomial) equations to develop mathematical curves that best separated LC cases from controls. The entire spectrum for each individual (LC and controls) was tested against these equations, using the relative deviation from each of the curves to check a final discrimination method.
Results We have found two distinct zones representing certain VOCs, which contain ∼27% of LC patients but 0% of controls, and so may represent true abnormal biological pathways. Two polynomial equations have been generated and the area of greatest deviation between the LC and control curves corresponds to multiple VOCs having a retention time in the gas chromatography of 8–17 s. The regression (R2) is several fold higher than for any linear or exponential relationship tested. See fig 1.
Conclusion After allowing for potential confounders, we can still discriminate between patterns of VOCs in the breath of LC vs controls. A larger prospective study is now testing these predictive models and categorising VOC profiles by histological subgroup, smoking status and following treatment.
{kind=link}
AUC, area under the curve; RT, retention time.
S120 TUMOUR NECROSIS FACTOR α EXPRESSION IN TUMOUR ISLETS CONFERS A SURVIVAL ADVANTAGE IN NON-SMALL CELL LUNG CANCER
C. M. Ohri, A. Shikotra, R. H. Green, D. A. Waller, P. Bradding. Institute for Lung Health, Glenfield Hospital, Leicester, UK
Introduction The role of tumour necrosis factor α (TNFα) in cancer development and progression is complex, with both protumourigenic and antitumourigenic roles proposed. In patients with non-small cell lung cancer (NSCLC), infiltration of tumour epithelial cell islets by macrophages confers extended survival. We therefore hypothesised that the anatomical microlocalisation of TNFα is critical for its function. This study investigated the expression of TNFα in the tumour islets and stroma in NSCLC with respect to survival.
Methods We used immunohistochemistry to identify cells expressing TNFα in the tumour islets and stroma in 133 patients with surgically resected NSCLC. Patients were divided according to survival into above median survival (AMS) and below median survival (BMS) groups. To assess whether TNFα+ cells were localised to macrophages or mast cells, a double-stain technique was used.
Results There was increased expression of TNFα in the tumour islets of patients with AMS compared with those with BMS (median 27.2 vs 18.8 cells/mm2, respectively, p = 0.006). There was no significant difference in expression in the stroma of AMS compared with BMS patients (23.8 vs 16.8 cells/mm2, p = 0.31). Using multivariate Cox proportional hazards analysis, increasing tumour islet TNFα density emerged as a favourable independent prognostic indicator (p = 0.048) and, conversely, stromal TNFα density was an independent predictor of reduced survival (p = 0.007). Patients with high TNFα expression (upper tertile) were noted to have a significantly higher 5-year predicted survival as opposed to patients with low TNFα expression (lower tertile) (43% vs 22%, p = 0.01). In patients with AMS, 100% of TNFα+ cells were macrophages and mast cells, compared with only 28% in the islets and 50% in the stroma of BMS patients (p<0.001).
Conclusion Increased expression of TNFα in the tumour islets of patients with NSCLC is associated with improved survival, suggesting a role in the host antitumour immunological response. The microantomical site of TNFα expression, and its expression by specific cells (macrophages and mast cells), is critical for this effect.
S121 CLINICAL IMPLEMENTATION OF AN 84-GENE SIGNATURE PREDICTING EARLY RECURRENCE AFTER RESECTION FOR NSCLC
1B. M. Muehling, 2H. Kestler, 3K. H. Holzmann, 1L. Sunder-Plassmann. 1Department of Thoracic and Vascular Surgery, University of Ulm, Ulm, Germany, 2Department of Internal Medicine, University of Ulm, Ulm, Germany, 3Centre for Clinical Research, University of Ulm, Ulm, Germany
Background Gene expression-based prediction of survival has been described to be an accurate tool to predict survival in non-small cell lung cancer (NSCLC). Yet clinical experience with this method is limited. For this reason, to test the accuracy of gene signatures in the clinical setting we performed a gene expression-based analysis in tissue specimens of patients with NSCLC who had surgical tumour resection in our department.
Methods Tissue specimens from 47 patients were selected from our bio-bank and stratified according to time of recurrence: early (ER) and late (LR) recurrence. Cut-off for early/late recurrence was set at 12 months according to Chen.1 We performed a hierarchical cluster analysis using Affymetrix U133A gene chips. Results were correlated to histopathological tumour stages and early/late tumour recurrence. For statistical analysis the positive predictive value (PPV) of our gene signature was determined.
Results We analysed 19 patients with ER and 28 patients with LR with a median follow-up time of 15 and 28.5 months, respectively. We identified an 84-gene signature with a PPV of 87% after cross-validation. The 84-gene signature was significantly correlated to median time of recurrence: 7 vs 23 months; p<0.001. The PPV of our gene signature in T1 patients was 80%, and in N0 patients 88%.
Summary and Conclusion After surgical resection of NSCLC a gene signature-based analysis represents an adequate tool to predict recurrence accurately. Especially in T1 and N0 patients, PPV is high. By this means patients at risk could be identified. To justify routine implementation of this technique it should be validated in a prospective clinical trial.
References
S122 DELIVERY OF MAGNETIC NANOPARTICLES BY MESENCHYMAL STEM CELLS FOR HYPERTHERMIC TREATMENT OF LUNG CANCER
1M. R. Loebinger, 1P. G. Kyrtatos, 1M. F. Lythgoe, 2P. Southern, 2M. Kallumadil, 1A. N. Price, 2Q. A. Pankhurst, 1S. M. Janes. 1University College London, London, UK, 2The Royal Institution of Great Britain, London, UK
Introduction Lung cancer is the biggest cancer killer. The ability of mesenchymal stem cells (MSCs) to home specifically to tumours has suggested their potential use as a delivery vehicle for cancer therapeutics. We hypothesised that human MSCs could be labelled with superparamagnetic iron oxide (SPIO) nanoparticles, which can then be used for real-time in vivo tracking by magnetic resonance imaging (MRI) and tumour treatment by targeted localised hyperthermia with application of magnetic fields.
Methods Human MSCs were labelled with SPIO in culture with 0.5 mg/ml Chemicell NC-D nanoparticles and the amount of iron quantified using a superconducting quantum interference device (SQUID). In vivo subcutaneous and systemically delivered metastatic lung xenograft cancer models were performed in NOD/SCID mice. MRI images were acquired on a 9.4 T horizontal bore Varian VNMRS system. Heating of the SPIO-MSCs was performed with exposure to an AC magnetic field (150–200 Oe) for 20 min.
Results MSCs were labelled with up to 32 pg/cell of SPIO (SPIO-MSC), with no effect on proliferation, survival, differentiation or tumour homing capacity of the cells. As few as 1000 SPIO-MSCs could be detected by MRI 1 month after their co-injection with MDAMB231 breast cancer cells, which formed subcutaneous tumours. Intravenously injected SPIO-MSCs could also be tracked in vivo to multiple lung metastases using MRI, observations that were confirmed histologically. The SPIO nanoparticles produced localised hyperthermia (up to 20°C increase) when placed in an AC magnetic field, and this localised heating effect was also seen with the in vitro SPIO-MSCs. The SPIO-MSCs were then injected in vivo into established MDAMB231 subcutaneous tumours and the mice were placed in an AC magnetic field. Localised tumour heating with up to a 6°C relative temperature increase of the tumour was demonstrated, and tumour histology showed localised tumour necrosis.
Conclusion This is the first study to utilise MRI to track MSCs to lung metastases in vivo, and the first to use SPIO-MSCs to deliver targeted tumour heating. This technique has the potential to track the homing of SPIO-MSCs to tumours and allow the specific delivery of heat, which may have a future role in cancer therapeutics.