Article Text

Statistics from Altmetric.com
S56 EVIDENCE FOR ASSOCIATION BETWEEN SARCOIDOSIS AND PULMONARY EMBOLISM FROM 30-YEAR RECORD LINKAGE STUDY
1A. P. Nataraja, 2C. J. Wotton, 2M. J. Goldacre, 1L-P. Ho. 1Oxford Sarcoidosis Clinic, Oxford Centre for Respiratory Medicine, Oxford, UK; Radcliffe Hospitals NHS Trust and MRC Human Immunology Unit, Weatherall Institute of Molecular Medicine, Oxford, UK, 2Unit of Health-Care Epidemiology, Department of Public Health, University of Oxford, Oxford, UK
Introduction Sarcoidosis is a multisystem disorder of unknown aetiology, characterised by the formation of non-caseating granuloma. A higher than expected incidence of pulmonary embolism (PE) was observed anecdotally in our Sarcoidosis Clinic over a 3-year period, raising the question of disease association.
Methods We carried out a retrospective cohort analysis using data from a well-established record linkage data set in Oxford (“ORLS”; years 1963–1998), and a more recent record linkage data set covering England (“England”; 1999–2005), to compare rate ratios (RRs) for pulmonary embolism and deep vein thrombosis (DVT) between people admitted to hospital for sarcoidosis and a reference cohort for all ages and those below 65 years. RRs of myocardial infarction, subarachnoid haemorrhage, abdominal aortic anerusym and cardiac failure were also analysed as controls. The reference cohorts comprised individuals with various minor medical and surgical conditions as main diagnoses (eg, squint, otitis media and nasal polyps). They were standardised by age, gender, year of first admission and district of residence. Rates of PE and control conditions were calculated based on person-years at risk, relative to that in the reference cohort. The confidence interval for the rate ratio and χ2 statistics for its significance were calculated.
Results We found a significantly increased RR for PE in patients with sarcoidosis, for patients both above and below 65 years of age, and in both data sets (RR 1.87, 95% CI 0.96–3.27 (ORLS); RR 2.72; 95% CI 1.52 to 4.50 (England) for all age patients). The RR of cardiac failure in sarcoidosis (RR 1.78, 95% CI 1.09 to 2.75 (ORLS); RR 3.23; 95% CI 2.02 to 4.89 (England) for all age patients), but not of other control diseases, was also increased.
Conclusions There appears to be an increase in susceptibility to PE, but not of control acute vascular incidents such as myocardial infarction and subarachnoid haemorrhage in patients with sarcoidosis. This supports anecdotal clinical observations, and suggests a link between coagulopathy and sarcoidosis, with clinical implications for management of these patients.
S57 INCREASING PREVALENCE OF SPIROMETRY-DEFINED COPD IN MIDDLE AGED MEN AND WOMEN IN SCOTLAND, 1995–2003
M. Gillies, J. Lewsey, H. Starkie, A. Briggs, M. Shepherd, K. MacIntyre. University of Glasgow, Glasgow, UK
Background Chronic obstructive pulmonary disease (COPD) is a growing public health problem. We examined the prevalence of spirometry-defined COPD over time in a nationally representative sample of the Scottish population.
Methods 13 142 individuals aged 35–64 years participated in the Scottish Health Surveys (1995, 1998 and 2003). Sociodemographic, lifestyle and health-related information was collected for each participant. Respiratory symptoms were assessed using the Medical Research Council (MRC) respiratory questionnaire and spirometry measured according to a standardised protocol. Complete data were available on 61.0% of participants; missing data were multiply imputed. The prevalence of spirometry-defined COPD (Global Initiative for Chronic Obstructive Lung Disease (GOLD) criteria) was calculated. Baseline characteristics of participants with spirometry-defined COPD were described. Logistic regression was used to model temporal changes in the prevalence of spirometry-defined COPD.
Results The overall prevalence of spirometry-defined COPD was 17.0% (95% CI 16.2% to 17.7%), 15.7% (14.5% to 16.9%), 15.5% (14.4% to 16.7%) and 20.0% (18.5% to 21.5%) in the 1995, 1998 and 2003 surveys, respectively. Of those with spirometry-defined COPD, 43.3.1% (40.7% to 45.9%) had mild disease, 41.2% (38.8% to 43.5%) moderate disease and 15.5% (13.9% to 17.2%) severe or very severe disease. Participants with spirometry-defined COPD were older (p<0.001), more likely to be male (p = 0.036), more socioeconomically deprived (p<0.001), more likely to be a current smoker (p<0.001) and more likely to report symptoms of breathlessness (p<0.001), phlegm (p<0.001) or wheeze (p<0.001) than other participants. The prevalence of spirometry-defined COPD increased over time (2003 vs 1995 odds ratio (OR) 1.46 (1.27 to 1.69)) independent of age, sex, socioeconomic deprivation, smoking status and respiratory symptoms. Only 15.4% (13.4% to 17.5%) of participants with spirometry-defined COPD reported having a long-standing respiratory condition; 3.9% (3.0% to 4.8%) specifically mentioned COPD. Two-thirds (64.6% (62.1% to 67.1%)) of the participants with spirometry-defined COPD that did not report a long-standing respiratory illness were current smokers. Among participants with spirometry-defined COPD there has been no change over time in the proportion that reported a respiratory diagnosis (2003 vs 1995 OR 1.08 (0.76 to 1.55)).
Conclusion The prevalence of COPD in Scotland is high, and rising. A significant proportion of individuals with spirometry-defined COPD do not report a long-standing respiratory illness; many continue to smoke. Despite increasing awareness among the public and healthcare professionals COPD remains underdiagnosed.
S58 IMPLICATIONS OF SCREENING FOR COPD: RESULTS FROM THE BURDEN OF OBSTRUCTIVE LUNG DISEASE (BOLD) STUDY FROM 14 COUNTRIES
1A. Jithoo, 2P. Enright, 3W. M. Vollmer, 3S. Gillespie, 1P. G. J. Burney. 1Imperial College, London, UK, 2University of Arizona, Tucson, USA, 3Center for Health Research, Kaiser Permanente, Portland, USA
Background A diagnosis of chronic obstructive pulmonary disease (COPD) requires the administration of prebronchial and postbronchodilator spirometry. However, it is not always feasible to perform spirometry in short office visits and particularly in countries with limited healthcare resources.
Aim To investigate the use of questionnaire predictors and peak expiratory flow (PEF) to identify those most likely to have COPD.
Methods Random samples of adults aged ⩾40 years from 14 sites (n = 9390) completed questionnaires about respiratory symptoms, COPD risk factors and health status, and performed prebronchial and postbronchodilator spirometry, including PEF, according to the standardised Burden of Obstructive Lung Disease (BOLD) study methodology. We used general classification and regression tree modelling (CART) to develop prediction models for COPD using questionnaire items and PEF. We conducted model building using a test sample (70%) and validated the results using a validation sample (30%).
Results CART modelling identified a high risk subgroup comprising 54.3% of the sample and consisting of individuals who had been told they have COPD/emphysema or who were long-term smokers (>20 years) or reported any dyspnoea. This subgroup had a 13% risk for having confirmed COPD and identified 87.2% of all cases. A reciprocal low risk group comprising 45.7% of the sample had only a 2.3% probability of having COPD (table 1). Adding prebronchodilator PEF data into the CART analysis resulted in a high risk group based only on the PEF data. This PEF model identified a high risk subgroup comprising a much smaller proportion of the population (21.6%) and yet capturing 83.8% of the true COPD cases.
Conclusion The use of PEF reduces the number of individuals who need confirmatory spirometry by more than half compared with questionnaire data, but retains high sensitivity. Using questionnaires and/or PEF screening for COPD can be useful especially in resource-limited settings.
General CART modelling for detecting moderate-severe COPD*
S59 IS ADULT HEIGHT RELATED TO THE RISK OF HAVING CHRONIC OBSTRUCTIVE PULMONARY DISEASE?
K. Ward, R. Hubbard. University of Nottingham, Nottingham, UK
Background A number of historical studies have suggested that shorter people are more likely to die from chronic obstructive pulmonary disease (COPD). The postulated mechanism for this association is that early life deprivation is associated with decreased growth and shorter adult stature and is also associated with an increased risk of developing COPD in adult life. Whether this association remains true today now that living conditions have improved in general is not known. The aim of this study is to quantify the current association between adult height and COPD, and to determine how this varies by age and adult socioeconomic status.
Methods Data on 1 204 110 people (>35 years old) were obtained from The Health Improvement Network—a longitudinal computerised general practice database. Height was compared between people with and without a diagnosis of COPD using linear regression. The potential confounders in this study were age, sex and adult socioeconomic score (measured as quintiles of postcode-linked Townsend score).
Results In our data set we had information on adult height for 1 025 662 (85%) people, and of these 2.7% had a diagnosis of COPD. The mean height for men was 175.8 cm and for women was 161.7 cm. Adult height and COPD showed a strong inverse relationship, with people diagnosed with COPD being 1.12 cm shorter on average than the general population after adjusting for sex, current social class and age. This difference was most marked in people aged 35–50 years (1.76 cm (95% CI 1.37 to 2.15) and decreased progressively with age, and was only 0.51 cm (95% CI 1.09 to −0.06 cm) in people over the age of 90 years. There was no clear trend between current adult socioeconomic status and the difference in height between people with and without COPD.
Conclusions Adult height is strongly associated with the risk of having COPD. This association was strongest in the youngest age category, suggesting that early life experience will remain an important risk factor for COPD for some time to come and possibly that COPD related to early life deprivation is more severe and tends to present at a younger age.
S60 RELATIONSHIP BETWEEN SERUM IGE LEVELS, SMOKING AND SMOKING CESSATION IN AN AGEING POPULATION IN THE UK (THE ELSA COHORT)
1J. Fingleton, 2S. Webster, 3N. Rice, 3D. Melzer, 2B. Patel. 1Royal Cornwall Hospital NHS Trust, Truro, UK, 2Royal Devon and Exeter NHS Foundation Trust, Exeter, UK, 3Epidemiology and Public Health, Peninsula Medical School, Exeter, UK
Introduction Cigarette smokers have higher immunoglobulin E (IgE) levels than non-smokers, but little is known about the effect of smoking cessation on IgE levels.
Aims The purpose of this study was to investigate the association between smoking and smoking cessation on serum IgE levels.
Methods We assessed the association between self-reported IgE levels and smoking history in 2365 individuals from the English Longitudinal Study of Ageing (ELSA) cohort.
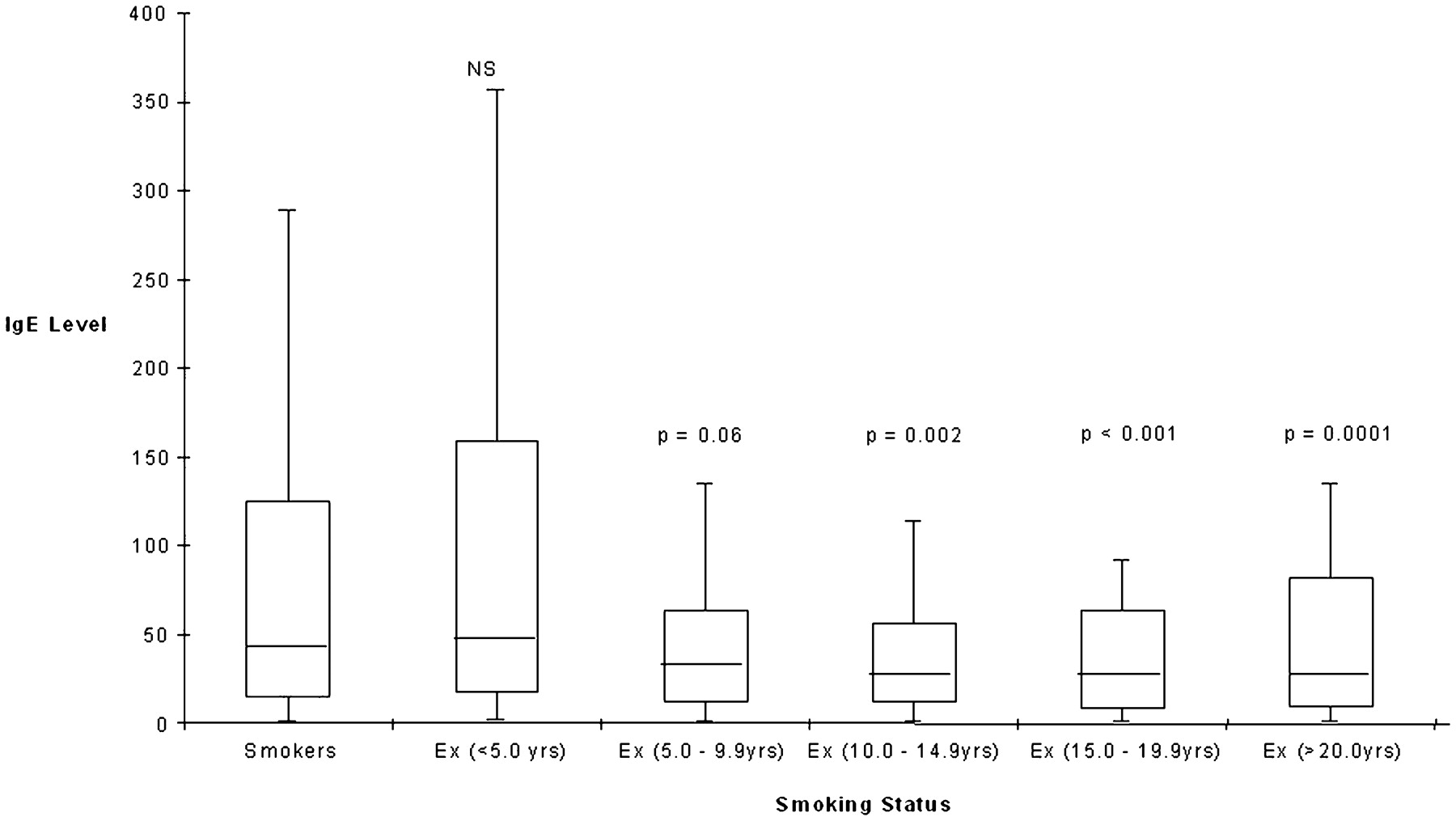
Results The 424 current smokers had higher IgE levels (median 42 kU/l (interquartile range 110)) than the 1052 ex-smokers (28 kU/l (70), p⩽0.0001). Ex-smokers had significantly higher IgE levels than the 889 non-smokers (22 kU/l (53), p⩽0.001). Ex-smokers were then further categorised according to time since smoking cessation. Ex-smokers of <5 years had IgE levels that were not significantly different from those of current smokers (46 kU/l (141)) (see fig 1). Ex-smokers of 5–9.9 years had lower levels than current smokers (32 kU/l (52)) but this failed to reach statistical significance (p = 0.06). Ex-smokers of >10 years had IgE levels that were similar to those of non-smokers and significantly lower than those of current smokers (p<0.001).
Conclusions The mechanism underlying elevated IgE levels in smokers is unknown. Our data suggest that this may be a direct effect of cigarette exposure that is reversible on cessation. However, the temporal decline appears to take place over a period of years.
{kind=link}
Immunoglobulin E (IgE) levels decline with time since smoking cessation. p Values are given relative to smokers.
S61 EXPLAINING ETHNIC GROUP DIFFERENCES IN LUNG FUNCTION: A CROSS-SECTIONAL STUDY
R. Hooper, M. K. Tumilty, J. F. Potts, P. G. J. Burney. Imperial College London, London, UK
Introduction and Objectives Different normal ranges for lung function are often assumed for different ethnic groups, though these are usually estimated from non-smoking, asymptomatic individuals, without adjustment for other risk factors. Assigning lower norms to a racial group that has experienced deprivation or other occupational/early life exposures may be discriminatory. Using data from the UK Burden of Lung Disease (BOLD) study, we estimated differences in lung function between ethnic groups adjusted for confounding variables.
Methods Participants aged ⩾40 years were randomly selected from practice lists at three general practices in London. The practitioner made initial contact, and those interested arranged an appointment with the study team for assessment. Forced expiratory volume in 1 s (FEV1) and forced vital capacity (FVC) were measured by spirometry, prebronchodilator and postbronchodilator. Quality of spirometry was reviewed centrally, and all technicians were trained and certified. Ethnic group, respiratory symptoms, health status and other risk factors were obtained from face-to-face interviews. Multivariable regression was used to estimate differences between ethnic groups in FEV1, FVC and the FEV1/FVC ratio, adjusting for confounders.
Results 4467 individuals were selected for recruitment, and investigators spoke to 1927. 677 provided complete questionnaire data and good quality spirometry. We present results in three ethnic groups: white (n = 550), black (n = 65, including mixed black/white) and Asian/other (n = 62, including mixed white/Asian, and other ethnic groups). In an unadjusted analysis, there was a significant difference in FEV1/FVC between blacks and whites (see table 1), which disappeared after adjusting for possible confounders. In contrast, there was no evidence for ethnic group differences in an unadjusted analysis of FEV1, but after adjusting for confounders there was a lower FEV1 in the black and Asian/other groups than in whites. Similarly, ethnic group differences in FVC became larger after adjusting for confounders.
Conclusions We found differences between ethnic groups in FEV1 and FVC which were not explained by age, height or other risk factors for respiratory disease. The FEV1/FVC ratio was more stable across ethnic groups. Several other studies have shown poorer lung function in blacks than whites. It remains unclear whether this indicates pathology or is a natural adaptation.