Article Text

Statistics from Altmetric.com
P124 REPRODUCIBILITY OF THE MULTIPLE BREATH NITROGEN WASHOUT TEST IN HEALTHY VOLUNTEERS AND SUBJECTS WITH MILD TO MODERATE ASTHMA
1M. F. Biddiscombe, 2S. Verbanck, 3S. Meah, 3P. J. Barnes, 3O. S. Usmani. 1Nuclear Medicine, Royal Brompton Hospital and National Heart and Lung Institute, Imperial College London, London, UK, 2Respiratory Division, Academic Hospital, Vrije Universiteit, Brussels, Belgium, 3Airways Disease Section, Royal Brompton Hospital and National Heart and Lung Institute, Imperial College London, London, UK
Introduction The multiple breath nitrogen washout (MBNW) test is a non-invasive physiological tool that can be used to assess differences in ventilation heterogeneity arising in the proximal (conducting) from that in the distal (acinar) airway compartments. Abnormalities in the MBNW acinar (Sacin) and conductive (Scond) airway indices have been observed and indicate significant ventilation heterogeneity in patients with asthma and chronic obstructive pulmonary disease (COPD).
Objectives To assess the same-day and day-to-day reproducibility of MBNW parameters (Sacin, Scond) in 24 healthy volunteers (HV, mean forced expiratory volume in 1 s (FEV1) 104%pred; age 22–59 years; males 12) and 12 patients with mild to moderate asthma (A, mean FEV1 92%pred; age 21–54 years; males 8).
Methods Each subject performed two MBNW runs (1 run = 3 MBNW tests) each day, on three separate days. Each MBNW test consisted of consecutive 1-litre oxygen inhalations until expired nitrogen was <2%.
Results Higher Sacin and Scond (greater heterogeneity) values were detected in A vs HV subjects. Functional residual capacity (FRC) calculated from MBNW correlated with that measured using body plethysmography (r = 0.65; p<0.01). No correlation was observed between Sacin and Scond and subject’s FEV1, FVC or FEF25–75 (p>0.10) for both groups. Day-to-day variability of Sacin and Scond were greater than spirometric measures (table 1).
Conclusion Sacin and Scond were significantly higher for asthmatic subjects compared with healthy volunteers, indicating greater ventilation heterogeneity. In both populations, the MBNW test showed acceptable same-day and day-to-day reproducibility in Sacin and Scond. In asthmatics, day-to-day variability was consistently greater than intra-day variability on all variables, which is probably a characteristic of variable airways obstruction. This information on variability is important to estimate sample size in therapeutic trials to assess the regional airway responses of the MBNW test to inhaled drug therapy.
P125 IS UPPER AIRWAY WHEEZE (“VOCAL CORD DYSFUNCTION”) THE MISSING LINK IN THE ASSOCIATION BETWEEN GASTRO-OESOPHAGEAL REFLUX DISEASE AND ASTHMA?
C. E. Bucknall, G. A. Miller, P. Vaughn. Stobhill Hospital, Glasgow, UK
We have recently reported our experience diagnosing and treating gastro-oesophageal reflux disease (GORD) objectively with pH studies to document normalisation of oesophageal acid exposure and, in an uncontrolled study, have shown that this strategy allowed significant reductions in asthma therapy.1 We now report the findings of a 3-month survey of co-morbidities affecting all patients attending a problem asthma clinic which may shed some light on the underlying mechanisms of this association. Case note review for demographics, co-morbidities and therapy requirements was undertaken. Relationships between categorical variables were examined using χ2 tests.
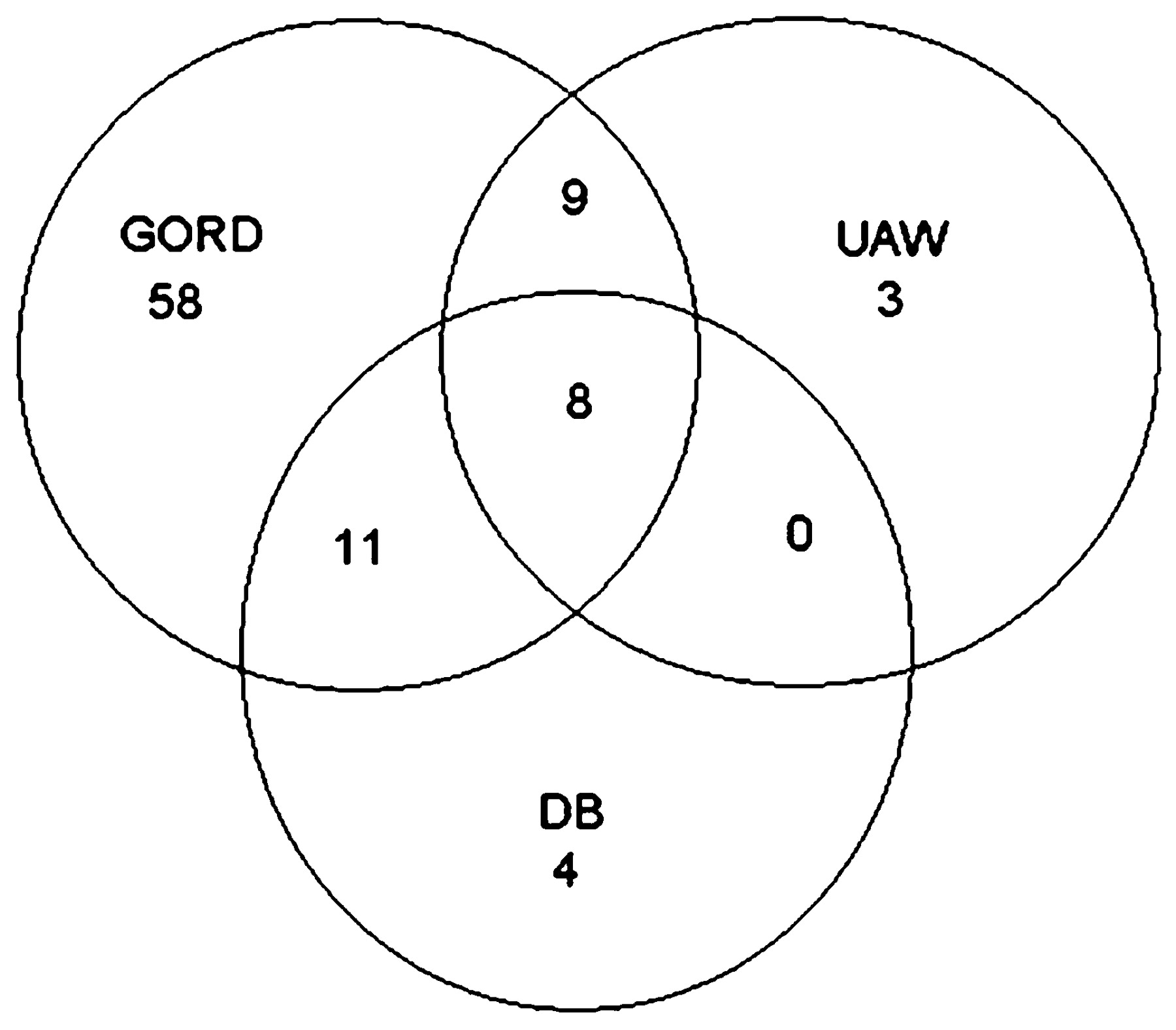
The relationships between the occurrences of GORD, upper airway wheeze (UAW) (often incorrectly attributed to vocal cord dysfunction) and dysfunctional breathing (DB) are shown in fig 1. Of the 86 patients with GORD, 50% have this diagnosis based on objective measurements, with the remainder reporting typical oesophageal symptoms (patients with exclusively extra-oesophageal symptoms generally undergoing pH study). UAW diagnosis is based on the observation of upper airway wheeze, since other tests in our hands have not proved useful.2 DB diagnosis is based on detailed assessment by a specialist respiratory physiotherapist, since previous study in our clinic has failed to prove the benefit of using Nijmegen scores or CPET.3

Venn diagram showing relationship of gastro-oesophageal reflux disease (GORD), upper airway wheeze (UAW) and dysfunctional breathing (DB).
The relationships between UAW and GORD and between UAW and DB are significant (p = 0.037 and 0.004, respectively), although no significant association is seen between DB and GORD (p = 0.13).
We postulate that GORD causes UAW and dysfunctional breathing—symptoms which mimic asthma—causing asthma treatment to be escalated inappropriately, and that effective therapy of GORD together with breathing control and education reduces symptoms due to UAW and DB and allows asthma therapy to be reduced. This hypothesis would explain the Cochrane findings that GORD intervention studies which use asthma symptoms and therapy requirements as outcomes often show positive benefit, whereas those which target physiological outcomes are usually negative.
P126 OBESITY AND THEOPHYLLINE USE ARE ASSOCIATED WITH GASTRO-OESOPHAGEAL REFLUX DISEASE IN A PROBLEM ASTHMA COHORT
G. A. Miller, C. E. Bucknall. Stobhill Hospital, Glasgow, UK
Data were collected on all 126 patients attending a problem asthma clinic over a 3-month period in order to construct a profile of clinic attendees and explore the inter-relationships between co-morbidities. Baseline demographics, asthma diagnosis and therapy and details of significant co-morbidities were collated. This abstract describes the relationships of gastro-oesophageal reflux disease (GORD), obesity and asthma therapy.
28 patients (22.2%) had a body mass index (BMI) <25, 34 (27%) had a BMI 25–30 and 46 (36.5%) had a BMI > 30. 86 patients (68%) had a diagnosis of GORD, this being a clinical diagnosis in 42 patients (48.8%) based on an abnormal pH study in 43 patients (50%) with 1 patient having abnormal barium swallow/endoscopy. 26 patients (31.3%) were taking more than 40 mg proton pump inhibitors (PPI) daily, higher doses being prescribed where a pH study on empirical 40 mg/day continued to show abnormal oesophageal acid exposure (>4% of time).
GORD and obesity were strongly associated (p = 0.0046). Using Pearson χ2 tests, we assessed the individual relationships of GORD and obesity (categorised as BMI ⩽30 and >30) with use of theophyllines and leukotriene receptor antagonists, low and high dose inhaled corticosteroids (800< or >800 μg beclomethasone dipropionate equivalent), oral corticosteroids, subcutaneous bricanyl infusion, omalizumab or other immune modulating drugs.
GORD was associated with high dose inhaled corticosteroids (p = 0.005) and theophylline (p = 0.0008) use. Obesity was also associated with theophylline (p = 0.04) use. Neither GORD nor obesity was associated with the other treatments described above. Regression analysis to take account of the interrelationship of obesity and GORD showed that theophylline use and obesity were independent predictors of the presence of GORD (p = 0.038 and p = 0.018, respectively).
This analysis shows that obesity and GORD were common co-morbidities in this population with a third of patients requiring higher than standard doses of PPI therapy. Theophylline usage and obesity were significant predictors for GORD, in keeping with the current knowledge base and raising the possibility that theophyllines should be used more cautiously in this context.
P127 IMPORTANCE OF CO-MORBID CONDITIONS IN PATIENTS ATTENDING A PROBLEM ASTHMA CLINIC
G. A. Miller, C. E. Bucknall. Stobhill Hospital, Glasgow, UK
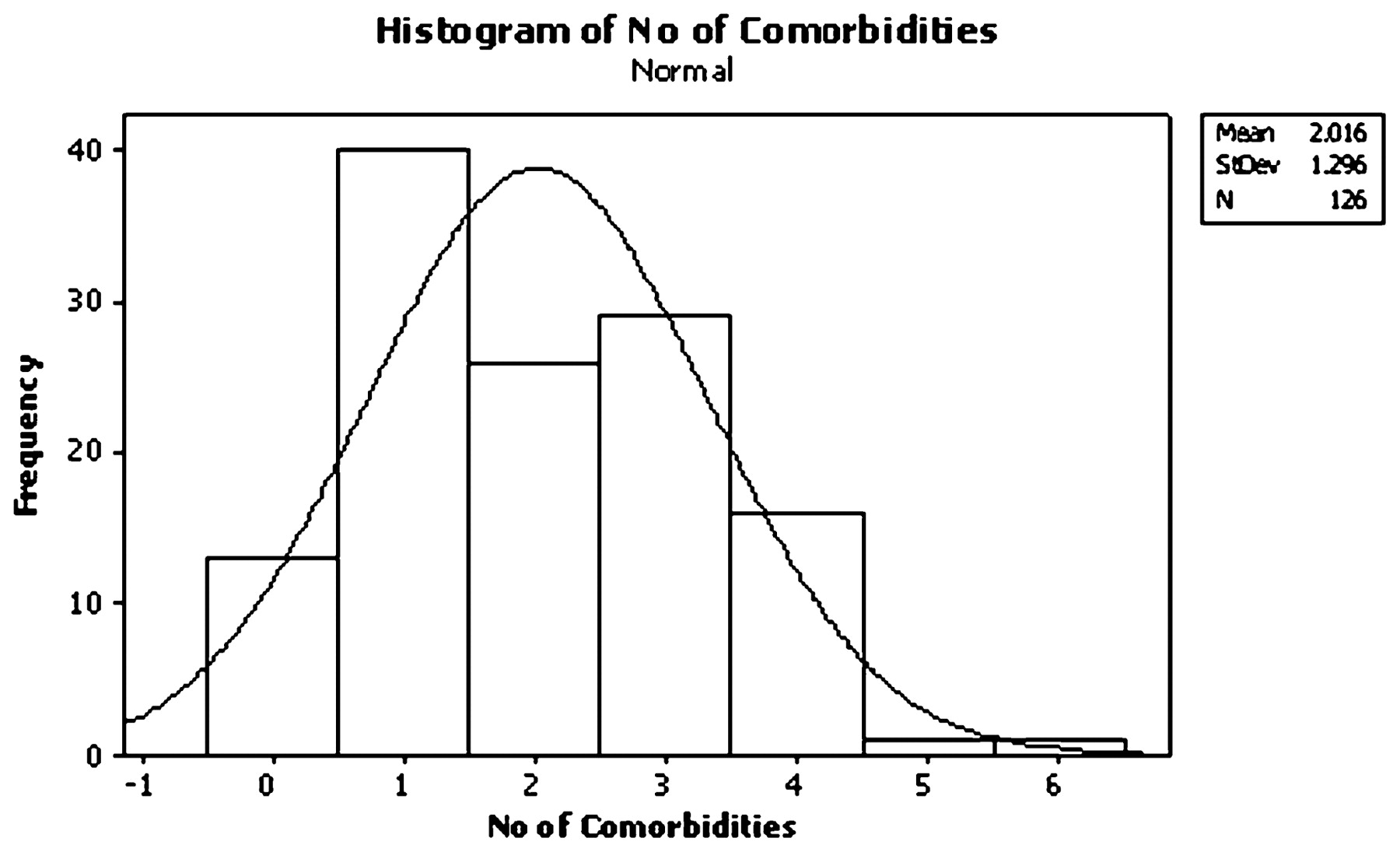
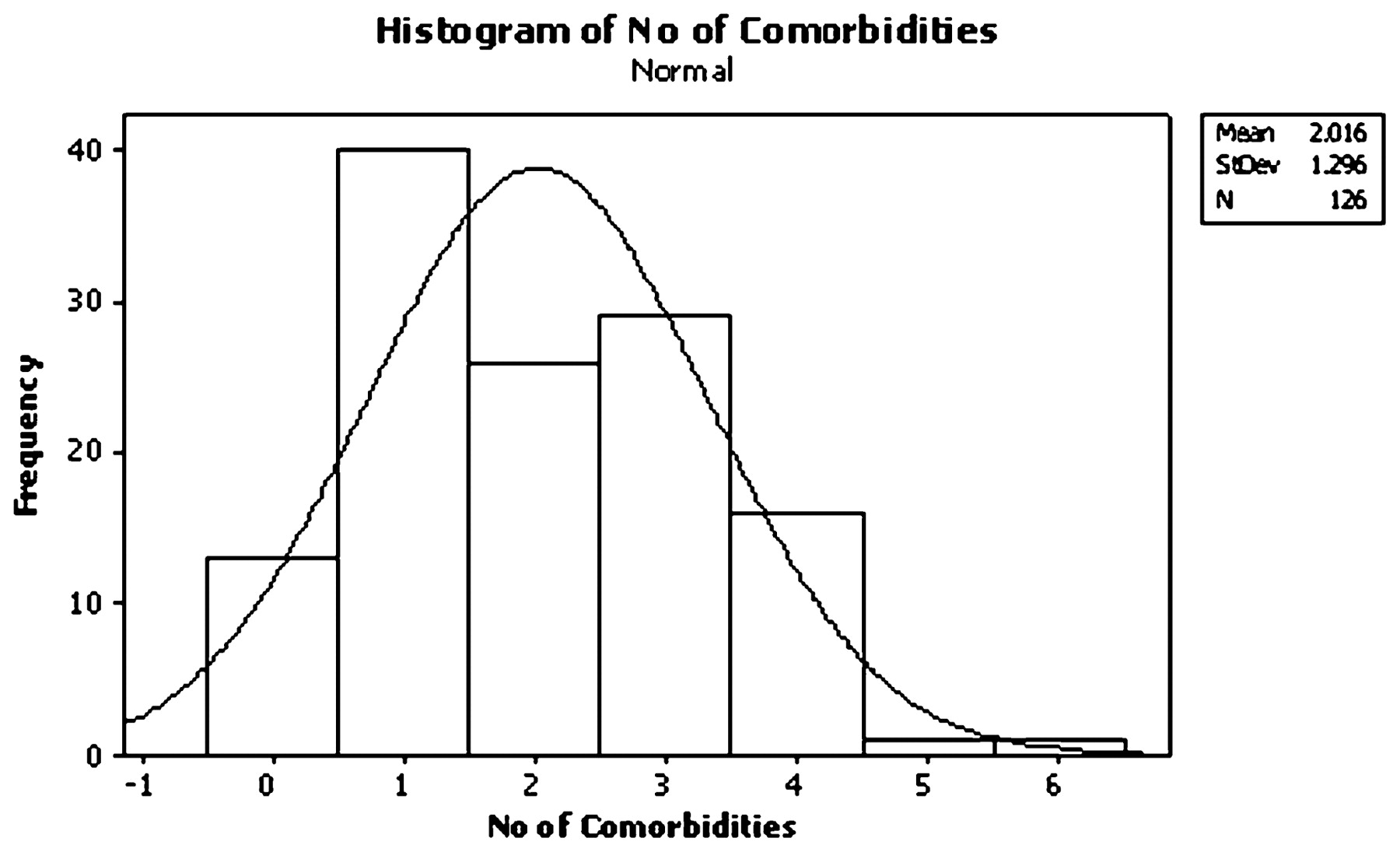
Data on all 126 patients attending a problem asthma clinic (PAC) over a 3-month period were collated in order to provide information on population demographics and co-morbidities. Only patients with confirmed and difficult-to-treat asthma attend the PAC, so this cohort does not include any patients with other conditions masquerading as asthma.
There were 89 women and 37 men (ratio 2.4:1). Mean age was 49.3 years (range 15–80). 72 were never smokers (57%) and only 10 (8%) were current smokers. Asthma diagnosis was based on ⩾12% bronchodilator reversibility in 67%, peak expiratory flow (PEF) variability in 21%, PC20 <2 mg/ml with compatible history in 4%, raised exhaled nitric oxide/compatible history/response to asthma treatment trial in 4%, leaving 5 patients (4%) with no current objective evidence of asthma but usually with previous documentation of this. Median body mass index (BMI) was 28.95 (range 17–61). Most patients were on BTS treatment steps 4 (42.9%) and 5 (39.7%). Median dose of inhaled corticosteroids for all cases was 1600 μg (range 200–8000), median dose for those on long-term oral corticosteroids was 10 mg (range 2.5–20). Other therapies used included theophyllines in 44%, leukotriene receptor antagonists in 33%, both of these in 17%, subcutaneous terbutaline in 6%, omalizumab in 9% and other steroid-sparing agents in 3%. 66 patients (53%) had documented action plans.
Co-morbid conditions were identified as contributing to symptomatology in all but 13 cases: dysfunctional breathing 18%, upper airway wheeze 16%, psychological or psychiatric problems 34%, rhinitis/sinusitis 15%, nasal polyposis 9%, bronchiectasis 8% (selective scanning policy), mucous hypersecretion without bronchiectasis 13%, ABPA 6% and severe asthma with fungal sensitisation (SAFS) in a further 11%.
Conclusion Co-morbid factors are more common in this cohort than in other published series.1 2 It is likely that problem/difficult asthma clinics have different characteristics due to regional referral practices. This analysis emphasises the importance of careful phenotyping of all difficult asthma patients in order to target therapy appropriately.
{kind=link}
{kind=link}
Histogram of number of co-morbidities.
P128 CORRELATIONS IDENTIFIED BETWEEN SPUTUM EOSINOPHILS AND PULMONARY FUNCTION IN PATIENTS WITH SEVERE REFRACTORY ASTHMA
A. Lu, G. Tavernier, J. A. Sloan, C. Prys-Picard, R. M. Niven. North West Lung Research Centre, Manchester, UK
Introduction Asthma phenotyping has become a major part of clinical evaluation for patients with severe refractory asthma at the Manchester Severe Asthma Service. This includes sputum cell analysis as well as routine pulmonary function assessments.
Objective To identify whether a clinical correlation exists between presence of sputum inflammatory cells and pulmonary function of patients attending the Manchester Severe Asthma Service.
Method Data were retrospectively collected from 156 patients within the service. Successful sputum sample cell analysis was compared with the nearest dated pulmonary function test results. Eight parameters (FEV1, FEV1/FVC ratio, reversibility, FEF50, TLC, volume of trapped gas, Tlco and Kco) were correlated with a ⩾2.5% presence of sputum eosinophils (eosinophilic sputum) and a ⩾50% presence of neutrophils (neutrophilic sputum).
Results Correlations between patients with eosinophilic sputum (38%) and increased volumes of trapped gas (p = 0.022), lower levels of FEF50 (p = 0.043) and higher levels of Kco (p = 0.043) were identified. Borderline trends were also identified between eosinophilic sputum and FEV1 (p = 0.077) and FEV1/FVC ratio (p = 0.053). No significant associations were identified between neutrophilic sputum and pulmonary function parameters apart from a weak trend between neutrophilic sputum and FEF50 (p = 0.094). Unsurprisingly, smoking status was significantly correlated with FEV1/FVC ratio (p = 0.031), FEF50 (p = 0.038), and Kco (p = 0.002). There was also a trend for a relationship between smoking status and FEV1 (p = 0.079).
Conclusion This study has shown a correlation between eosinophilic sputum and markers of asthma severity (FEF50, trapped gas), indicating that these patients may have more severe small airways obstruction. The study population had a high prevalence (>60%) of patients with non-eosinophlic sputum, although this population is on a large and varied array of anti-inflammatory treatments. Of this non-eosinophilic sputum group, 63% were shown to have high sputum neutrophils.
P129 OMALIZUMAB REDUCES MAINTENANCE ORAL CORTICOSTEROID USE IN PATIENTS WITH SEVERE PERSISTENT ALLERGIC ASTHMA
1R. Niven, 2M. Molimard, 3R. Buhl, 4V. Le Gros, 5A. Thielen, 6J. Thirlwell, 7R. Maykut. 1University Hospital of South Manchester and the University of Manchester, Manchester, UK, 2CHU Pellegrin-Carriere, Bordeaux, France, 3Mainz University Hospital, Mainz, Germany, 4Novartis Pharma SAS, Rueil-Malmaison, France, 5Novartis Pharma GmbH, Nuremberg, Germany, 6Novartis Horsham Research Centre, Horsham, UK, 7Novartis Pharma AG, Basel, Switzerland
Background Side effects associated with oral corticosteroids (OCS) place a significant burden on patients and healthcare resources. Treatments that limit OCS use can help to reduce the burden associated with long-term steroid therapy.
Methods Data on maintenance OCS use in patients (⩾12 years) with severe persistent allergic asthma who had received omalizumab for >16 weeks were gathered from physicians in France, UK and Germany. Data were pooled to assess the OCS-sparing potential of omalizumab. OCS doses (as prednisolone equivalent) were recorded at baseline (start of omalizumab treatment) and at a non-specific time point after at least 16 weeks of omalizumab therapy.
Results Data were available for 411 omalizumab-treated patients (France, n = 108; UK, n = 65; Germany, n = 238); 199 (48.4%) were taking maintenance OCS at baseline (UK, n = 33; France, n = 64; Germany, n = 102). In total, 110 (55.3%) OCS patients stopped or reduced their OCS dose at the time of data collection (42 (21.1%) stopped; 68 (34.2%) reduced). OCS dose was increased or remained unchanged in 88 (44.2%) patients. Post-baseline data were missing for one patient. In patients receiving maintenance OCS at baseline, mean (SD) baseline dose was 19.6 mg (16.22) and the mean (SD) absolute and percentage reduction in OCS dose was 7.7 mg (12.23) and 32.8% (67.36), respectively. In patients who stopped or reduced maintenance OCS, mean (SD) baseline dose was 23.0 mg (17.30) and the mean (SD) absolute and percentage reduction in OCS dose was 15.0 mg (11.12) and 71.3% (29.09), respectively.
Conclusion Real-life experience demonstrates the OCS-sparing potential of omalizumab in some patients with severe persistent allergic asthma.
P130 RISK FACTORS FOR FREQUENT EXACERBATIONS AND AIRFLOW OBSTRUCTION IN SEVERE ASTHMA
S. Shah, S. Gupta, M. Bafadhel, A. Singapuri, P. Haldar, W. Monteiro, I. D. Pavord, A. J. Wardlaw, C. E. Brightling. Glenfield Hospital, Institute for Lung Health, Leicester, UK
Background Severe asthma is a heterogeneous disease that affects 10% of all adult patients with asthma. Attempts have been made to define this phenotypic heterogeneity, but there remains a need to understand the features associated with the increased exacerbation frequency and persistent airflow obstruction that characterise the disease.
Methods Patients attending the difficult asthma clinic between January 2007 and December 2008 were assessed with the recording of demographics, medical history, lung function, atopy and sputum. Baseline data was used to determine factors associated with (a) frequent exacerbations (⩾3 severe exacerbations (courses of oral prednisolone) in previous year) and (b) fixed airflow obstruction (FAO, post-bronchodilator (BD) FEV1/FVC ratio <70% and FEV1% predicted <80%). Further analysis of longitudinal data and multiplex analysis for cytokines and chemokines in the sputum supernatant is ongoing.
Results We recruited 203 subjects; mean (SEM) age 49 (1) years, M:F ratio 79:124, atopy 42% and smoking history 4 (1) pack-years. Other characteristics were: post-BD FEV1/FVC ratio 71 (1)%, post-BD FEV1% predicted 78 (2)%, sputum neutrophils 61 (2)%, sputum eosinophils geometric mean 2.6 (95% CI 2.0% to 3.4%), severe exacerbations in past year 3.5 (0.3). Univariate analysis revealed: (1) eosinophilic airway inflammation (sputum eosinophils >3%) was associated with poorer FEV1% predicted and higher serum IgE levels; (2) male asthmatics were older and had worse post-BD FEV1% predicted and FEV1/FVC ratio. Multivariate analysis using logistic and standard multiple regression revealed: (1) none of the clinical characteristics predicted frequent severe exacerbation; (2) male gender emerged as an important predictor of FAO (p = 0.003, odds ratio (OR) 3.4); (3) neutrophilic airway inflammation best predicted FAO among males (p = 0.02, OR = 1.04); (4) post-BD FEV1/FVC ratio was predicted by neutrophilic and eosinophilic airway inflammation (R2 = 0.13, p = 0.003) and post-BD FEV1% predicted was best predicted by eosinophilic airway inflammation (R2 = 0.12, p = 0.006); (5) eosinophilic airway inflammation was associated with poorer lung function in females (R2 = 0.16, p = 0.003) but not males.
Conclusions In our cohort we identified that airflow obstruction was associated with male gender and best predicted by eosinophilic and to a lesser extent neutrophilic inflammation. We were unable to identify predictors for frequent exacerbators.