Article Text

Statistics from Altmetric.com
P94 USE AND UTILITY OF A 24-HOUR INFORMED TELEPHONE SUPPORT SERVICE FOR “HIGH-RISK” PATIENTS WITH COPD
J. R. Hurst, F. Fitzgerald-Khan, J. J. P. Goldring, J. K. Quint, J. P. Dilworth, C. Mikelsons, J. A. Wedzicha. Royal Free Hampstead NHS Trust, London, UK
Introduction The “epidemic” of chronic obstructive pulmonary disease (COPD) requires innovative service developments to improve outcomes. It is particularly important to prevent hospitalisations. Successful chronic care models in COPD have been described. We present the first evaluation of an Early Presentation and Intervention in COPD (EPIC) service focused on “informed” 24/7 telephone support for high-risk NHS COPD patients. The service was funded by a Clinical Innovations competition at Royal Free Hampstead NHS Trust.
Method 74 “high-risk” patients were recruited over 6 months (defined as GOLD stage IV or those with previous hospitalisation) from inpatient and outpatient settings, representing 32% of patients admitted over that period. After a recruitment interview to record key patient and COPD information, patients were contacted every 2 months by a nurse and reviewed in clinic 6-monthly. Patients were invited to use the telephone service “when you need any advice about your chest and particularly if you think you are having a flare-up”. We present the use and utility of the service over 1 year.
Results The 74 patients were high-risk (eg, mean (SD) age 70.3 (9.1) years, forced expiratory volume in 1 s 44.2 (16.5)%). 30% were on long-term oxygen therapy and 46% lived alone. 70% of patients completed 1 year, 23% died and 7% left. Follow-up was for a total of 22074 days. 76% of patients used the service or it was used on their behalf, generating 258 calls (mean duration 7.9 min) at a rate of 1 call/100 patients/day. 76% of calls were between 08.00 h and 17.00 h. The proportion of calls in response to possible exacerbation did not vary by day, but was higher overnight and at weekends. There were very few overnight calls, most of which required further assistance from emergency services. To avoid one hospital assessment overnight, the service would require 7359 patients. The 52 patients completing 1 year had a reduced number and duration of hospitalisations while on the service compared with the previous year (31 vs 56 admissions and 289 vs 461 days, both p = 0.002). The patients valued the service.
Conclusion A telephone advice line for high-risk COPD patients reduces hospitalisation and is valued by patients, but is unlikely to be cost-effective 24/7 at a local level given the low volume of overnight calls.
P95 EFFECT OF TELEPHONE WEATHER ALERT SYSTEM ON EMERGENCY COPD ADMISSIONS AND HEALTHCARE UTILISATION IN PATIENTS WITH MILD TO MODERATE AIRFLOW OBSTRUCTION
N. Diar Bakerly, A. Thompson, J. A. Roberts. Salford PCT, Salford, Lancashire, UK
Introduction Exacerbations are a major cause of morbidity and mortality in patients with chronic obstructive pulmonary disease (COPD). They have a great impact on patients’ health, as well as having a large impact on healthcare utilisation (HCU) including emergency hospital admissions. They are more frequent in the winter months, and it has been hypothesised that they are positively linked with a sudden drop in temperature.
Aims To evaluate the effectiveness of a telephonic alert system (the Met Office project) to warn patients with COPD of severe weather changes on hospital admissions and HCU.
Methods All patients with mild to moderate airflow obstruction from three primary care practices were invited to participate. The project ran between 1 November 2008 and 28 March 2009. Weather alerts were delivered to patients via automated message by the Met Office. The primary outcome was number of emergency COPD admissions. Secondary outcomes were hospital bed-days, general practice consultations (surgery visits and telephone advice), home visits, visits to A&E, visits by COPD early supported discharge (ESD) team and out-of-hours service were measured during the project and compared (for the same patients) with the same data between 1 November 2007 and 28 March 2008 (12 months earlier).
Results A total of 435 patients were invited to participate and 157 (34%) patients took part in the project. Mean (SD) age 71 (9.7) years, forced expiratory volume in 1 s (FEV1) 1.4 (0.5) l and 59.1 (16.5)% predicted. During the project five weather alerts were generated (first alert reached 150 patients; second reached 146; third reached 138 patients; fourth reached 137 patients; and the fifth reached 125 patients). Data on hospital admissions and HCU are shown in table 1. The cost of the project was £18 per patient enrolment. The total mean cost per patient has increased from £262 before initiation of the project to £400 after initiation.
Conclusions The weather alert project was associated with a significant drop in visits to general practice and visits by out-of-hours services. Home visits increased significantly. A non-significant increase in hospital admissions with exacerbations of COPD was noted. The overall cost per patient increased.
P96 EFFECT OF AN INNOVATIVE AUTOMATED INTERACTIVE HEALTH FORECAST ALERT SYSTEM ON RATE OF EXACERBATIONS OF COPD
1D. Halpin, 2T. Laing-Morton, 3M. Levy, 2P. Marno. 1Royal Devon & Exeter Hospital, Exeter, UK, 2Met Office, Exeter, UK, 3University of Edinburgh, Edinburgh, UK
Introductions and Objectives We have developed a proactive chronic obstructive pulmonary disease (COPD) health forecast service that alerts patients to an elevated risk of exacerbations. A rule-based forecasting model predicts periods of increased risk triggering a direct-to-patient alert via an interactive automated telephone call. The forecast is linked to an anticipatory care intervention package which includes an information pack containing practical advice on recognising early symptoms of an exacerbation, managing their home environment and keeping active. Over the winter of 2008–9 we have assessed the effectiveness of this service in a randomised controlled trial.
Methods 78 patients with COPD were recruited from three general practices. All were given the information pack in December 2008 and half were randomised to receive the forecast calls. Patients completed the EXACT daily symptom diary on a Blackberry PDA. Responses were reviewed on a daily basis and exacerbations confirmed by telephoning patients. Data were collected for 4 months from December to March. Heath status was assessed at the beginning and end and exacerbation rates compared using a negative binomial model.
Results The mean age of the patients was 69.3 years, mean forced expiratory volume in 1 s (FEV1) was 1.43 l, 74% were male. There was no significant difference in mean±SEM baseline SGRQ (52±3 vs 54±2) or EXACT (33±2 vs 32±2) scores. The mean maximum EXACT score was similar in both groups (54±2 vs 54±2). There was a non-significant trend for a lower rate of confirmed exacerbations over the winter in patients receiving the forecast (0.95 vs 1.17, 95% CI for difference −0.45 to 0.89).
Conclusions This was a complex trial involving innovative delivery and response mechanisms to capture patient experience. This type of methodology was viewed positively by patients and showed that a health forecasting service may reduce exacerbation rates.
P97 GEOGRAPHICAL INFLUENCE ON REPORTING COPD EXACERBATIONS
P. J. Rudd, G. C. Donaldson, J. K. Quint, J. P. Goldring, J. R. Hurst, J. A. Wedzicha. Academic Unit of Respiratory Medicine, University College London, Royal Free and University College Medical School, London, UK
Background Seeking prompt treatment for exacerbations of chronic obstructive pulmonary disease (COPD) hastens recovery and improves quality of life. We investigated whether the straight line distance between the patient’s home, their GP and our study clinic influenced whether patients reported their exacerbations.
Methods We investigated 266 COPD patients who had been monitored for at least 1 year and had experienced at least one exacerbation between October 1995 and September 2007. Exacerbations were recorded on daily diary cards and defined as two respiratory symptoms including at least one major symptom for two consecutive days. Patients were asked to telephone for a same day clinic appointment if an exacerbation occurred. Free taxi transport was provided. We investigated the relationship between the proportion of exacerbations reported and the distance from the patient’s home (centre of postcode district) to the clinic and to their GP surgery. Analysis was performed on data collected before May 2005 and after June 2005 when the clinic moved location from hospital A to hospital B.
Results The mean (SD) age was 67.5 (8.2) years, forced expiratory volume in 1 s (FEV1) 1.14 (0.5) l, FEV1% predicted 45.2 (18.0)%, smoking history 50.1 (34.9) pack years. The median distance from the patient’s home to hospital A was 2.4 km (IQR 1.3–5.5) and to hospital B was 8.6 km (IQR 4.3–11.0). For patients studied at hospital A (fig 1), the proportion of reported exacerbations fell as distance increased (rho = −0.18, p = 0.01, n = 194). Such a relationship was not observed with patients attending hospital B (rho = −0.10, p = 0.31, n = 102). 66 patients attended both hospitals and, for these patients in whom the travelling distance increased, the proportion of reported exacerbations fell from a median of 50% (IQR 33–71%) at hospital A to 20% (0–50%) at hospital B (p = 0.004). There was no relationship between the distance to the GP surgery and reporting rates at hospital A (rho = 0.01, p = 0.93) or hospital B (rho = 0.08, p = 0.43).

Proportion of chronic obstructive pulmonary disease (COPD) exacerbations reported by patients in relation to the straight line distance from their home to hospital A.
Conclusions Longer travelling distances decrease the likelihood that patients will report exacerbations for treatment in clinical studies. This is an important issue for organisation and delivery of clinical service and trials.
P98 RETROSPECTIVE ANALYSIS OF PREDICTORS OF MORTALITY AND READMISSION AFTER AN EXACERBATION OF COPD
A. Fahim, W. Lee, S. Faruqi, J. A. Kastelik. Castlehill Hospital, Cottingham, East Yorkshire, UK
Introduction and Objectives Patients who survive an acute exacerbation of COPD (AECOPD) are at increased risk of death and rehospitalisation. The aim of this study was to identify predictors of mortality and readmission in patients admitted with an AECOPD.
Methods We retrospectively reviewed 402 episodes in 205 patients admitted to our hospital with an AECOPD from April 2005 to June 2009. Forced expiratory volume in 1 s (FEV1)%, number of admissions in the last 12 months, current medications, MRC dyspnoea scale, performance status (PS), co-morbidities, social circumstances, total white cell count (WCC), C-reactive protein (CRP), smoking status and demographic parameters were obtained and analysed.
Results One hundred and six men of median age 69 years (range 47–93) with 225 episodes and 99 women of median age 72 years (range 49–91) with 178 episodes comprised the study population. Overall, 42% had two or more admissions in the previous 12 months. 67% had an FEV1 <50% of predicted and 63% had an MRC dyspnoea scale ⩾3; 46% had a PS ⩾3 and 31% had two or more co-morbidities; 62% of patients were on a combination of inhaled steroids and long-acting β2 agonist and 43% were on an anticholinergic agent; 24% lived alone and 43% continued to smoke. Cumulative mortality was 6.8%. Of those patients, 55% had ⩾2 admissions in 12 months, 69% had an MRC dyspnoea scale ⩾3, 59% continued to smoke, 62% had a PS ⩾3 and 62% had two or more co-morbidities. We found social isolation to be the only significant predictor of mortality. The factors associated with increased risk of readmission included lower FEV1% and continuing to smoke.
Conclusion Our study suggests that mortality and readmissions in patients admitted with an AECOPD are multifactorial. Social isolation appears to be associated with an increased risk of death. These findings need to be confirmed in a larger prospective study.
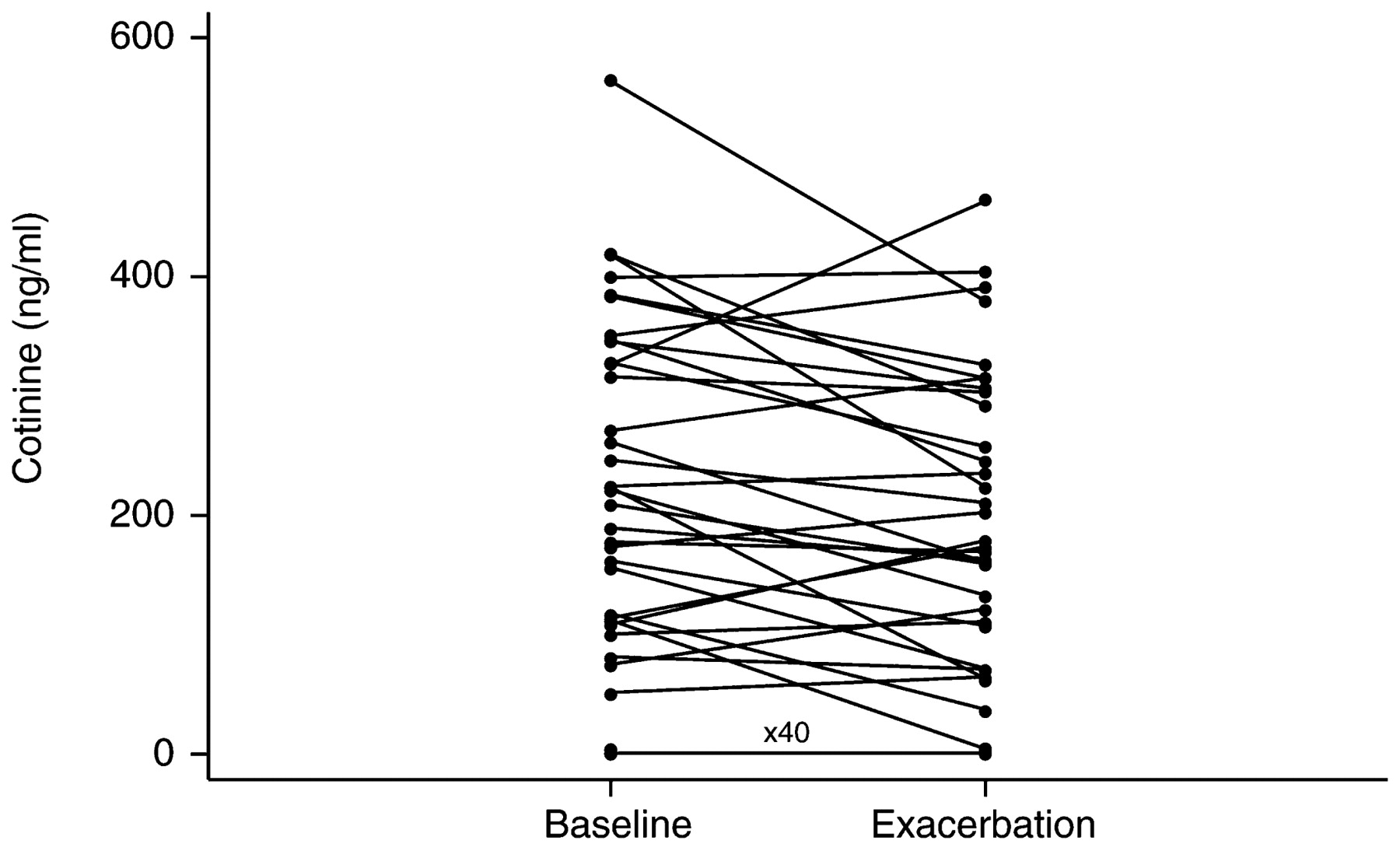
P99 CHANGES IN PLASMA COTININE AT EXACERBATION AND FASTER EXACERBATION RECOVERY IN NON-SMOKERS IN COPD
1G. C. Donaldson, 1J. K. Quint, 2D. Powrie, 1R. West, 1J. A. Wedzicha. 1University College London, London, UK, 2Southend University Hospital, Southend, UK
Introduction The benefits of not smoking on survival, lung function and risk of hospital admission are well established in chronic obstructive pulmonary disease (COPD). Patient self-reporting of tobacco use can be unreliable due to its social unacceptability. We investigated whether acute exacerbations of COPD differed between smoking and non-smoking patients.
Methods Seventy-two patients had plasma collected at baseline and exacerbation in which cotinine was measured by capillary column gas-liquid chromatography. Exacerbations were defined as two consecutive days of two or more respiratory symptoms, of which one was increased dyspnoea, sputum purulence or sputum volume; a few were identified by questioning the patients about treatment by their general practitioner or hospital doctor. Blood samples were taken 3.7 days (SD 2.5) after onset. Exacerbation recovery was determined as the number of days after onset that symptoms persisted and was followed by two consecutive days clear of symptoms. A smoker was defined as having a baseline cotinine concentration >15 ng/ml.
Results The 72 patients had a mean (SD) age of 69.5 (8.9) years, forced expiratory volume in 1 s (FEV1) 52.4 (17.0)% predicted and a median 2.79 (IQR 1.1–3.6) exacerbations per year. Plasma cotinine fell significantly in 72 patients (Wilcoxon; p = 0.022) and in smokers in particular from 223 ng/ml (IQR 136–345) to 190.0 ng/ml (IQR 115–304); p = 0.014, fig 1). Recovery times from exacerbation were available for 65 exacerbations; data were missing because the exacerbation took longer than 50 days to recovery or no symptoms were recorded post onset. Smokers took a median 14.5 days (IQR 8.5–25, n = 32) to recover which was significantly longer than in non-smokers who took 10 days (IQR 6–16; n = 33; p = 0.041). There was no difference between smokers whose cotinine fell at exacerbation (median 15 days (IQR 10–27); n = 21) and those in whom cotinine increased (median 14 days (IQR 6–18); n = 11; p = 0.393).
{kind=link}
{kind=link}
Conclusion Patients with COPD reduce their smoking during exacerbation which can provide a window of opportunity to target smoking cessation advice. Exacerbations of COPD may be shorter if the patient does not currently smoke.
P100 SPUTUM BACTERIOLOGY IN ACUTE EXACERBATION OF COPD: UTILITY OF SPUTUM APPEARANCE AND PREVIOUS CULTURE RESULTS IN DETERMINING ANTIBIOTIC THERAPY
W. Shafiq, G. Antunes, S. Murphy. James Cook University Hospital, Middlesbrough, UK
Background Acute exacerbations of COPD (AECOPD) are predominantly non-infective or viral in origin and most patients are probably treated with antibiotics unnecessarily. It is recommended that sputum appearance is used as a guide to determine the need for antibiotic therapy.
Aim The purpose of this study was to describe the bacteriology of AECOPD and to determine the utility of sputum inspection and previous sputum bacteriology history in predicting the need for and choice of antibiotics in AECOPD.
Methods Patients admitted to James Cook University Hospital (JCUH) with AECOPD (June–Dec 2007) were identified and the hospital microbiology database reviewed. Sputum microbiology results for the index episode and previous episodes of AECOPD were included. The relationship between sputum appearance and culture result and the impact of positive sputum culture on subsequent episodes were assessed.
Results There were 226 AECOPD episodes in 81 patients. Sputum samples were obtained in 82.7% and were described as mucoid (MU) 9.1%, mucopurulent (MP) 63.6% and purulent (PU) 27.2%. Pathogens were isolated in 29.5% and frequency varied according to sputum appearance: MU 8%, MP 29.4%, PU 54.9% (odds ratio (OR) PU:MU 13.4 (1.56–298), p<0.005; PU:MP 2.92 (1.4–6.1), p<0.005). For 32 patients with ⩾2 AECOPD, previous sputum culture results were predictive of subsequent culture results (pathogen isolated if previous sputum positive 60.6% vs previous sputum negative 21.9%; OR 5.48 (2–14.8), p<0.005). 73 pathogenic organisms were isolated (H influenzae 38.2%, Pseudomonas 24.6%, S pneumoniae 22%, E. coli 11%, other 4%). The same organism was isolated in successive episodes in 57.5% (19/33) of which antibiotic sensitivities were identical in 84.2% (16/19).
Conclusions Bacterial infection in AECOPD may be predicted by inspection of sputum and previous sputum bacteriology. Antibiotics should be prescribed for AECOPD only if purulent sputum is obtained or if pathogenic bacteria were isolated from sputum in previous episode. The commonest pathogen isolated in AECOPD is H influenzae followed by Pseudomonas and S pneumonia. Antibiotic therapy in AECOPD should be guided by previous sputum bacteriology if available.
P101 VITAMIN D LEVELS AND SUSCEPTIBILITY TO HUMAN RHINOVIRUS EXACERBATIONS OF COPD
1J. K. Quint, 1G. C. Donaldson, 1J. J. P. Goldring, 1A. Patel, 1S. Karmali, 2N. Wassef, 2M. Thomas, 1J. A. Wedzicha. 1University College London, London, UK, 2Royal Free NHS Trust, London, UK
Background Human rhinovirus (HRV) is the commonest virus associated with exacerbations of chronic obstructive pulmonary disease (COPD). It has been postulated that vitamin D deficiency increases infection susceptibility. We investigated whether vitamin D deficiency was associated with increased susceptibility to HRV exacerbations in COPD and whether vitamin D levels change from baseline to exacerbation.
Methods We studied 56 COPD patients (32 men) of mean (SD) age 71.1 (9.2) years, forced expiratory volume in 1 s (FEV1) 50.9 (20.5)% predicted, smoking history 51.3 (31.8) pack-years. All patients were sampled in the winter and summer at baseline. Serum samples were assayed for vitamin D (25-OH) by chemiluminescence-based immunoassay. At exacerbation, 46 patients had sputum or nasopharyngeal swab (NPS) samples tested by real-time PCR for quantification of viral load for HRV and all patients had blood taken for vitamin D measurement. Exacerbations were identified using diary cards according to our usual definition; two symptoms (major and/or minor) for two consecutive days.
Results 50 patients not on vitamin D supplementation (Calcichew) had lower vitamin D levels in winter than in summer (median 25.9 nmol/l (16.4–36.0) and 36.2 nmol/l (22.4–59.4); p<0.001). Six patients on Calcichew did not show significant seasonal variation in their vitamin D levels (winter median 51.7 nmol/l (33.9–68.6), summer 50.6 nmol/l (33.0–69.6); p = 0.35). For those not on calcium, adjusting for seasonality there was no difference in vitamin D levels between baseline and exacerbation (p = 0.43). HRV-positive exacerbations (n = 12, viral load >175 pfu/ml) were not associated with lower vitamin D levels at exacerbation (median 30.0 nmol/l (20.4–57.8) and 30.6 nmol/l (19.4–48.7); p = 0.88). HRV load in sputum or NPS at exacerbation did not correlate with exacerbation vitamin D levels (rho = −0.29; p = 0.23 and rho = −0.09; p = 0.79, respectively).
Conclusions Patients with lower vitamin D levels are not more likely to be HRV positive at exacerbation and exacerbation levels of vitamin D do not correlate with HRV load. Vitamin D levels do not decrease at exacerbation in COPD.
Funded by NIH RO1 HL082578.
P102 CONCURRENT COPD/PNEUMONIA: INCIDENCE AND CLINICAL OUTCOMES AMONG PATIENTS ADMITTED WITH EXACERBATION
1N. Ahmad, 1S. George, 1E. Davis, 2K. S. Srinivasan, 2H. Moudgil. 1Princess Royal Hospital, Telford, UK, 2Princess Royal Hospital and University of Keele Medical School, Telford, UK
Background Although infection is frequently implicated in exacerbations of chronic obstructive pulmonary disease (COPD), the actual reporting of concurrent pneumonia is more variable and anecdotally can be subjective. Despite similar clinical outcomes, the 2008 RCP/BTS National Audit identified a disproportionately higher than expected reporting of concurrent pneumonia among patients admitted with COPD at this hospital.
Objectives More robustly correlating with radiology reported data on COPD admissions, objectives were (1) to report the actual incidence of concurrent COPD/pneumonia among admissions coded as exacerbation and (2) to determine in which way this then influences clinical outcomes.
Methods Retrospective data including formal radiology reporting of admissions over 12 months to end December 2008 were analysed ranking non-parametric data (Mann-Whitney U) or ratios by χ2 reporting statistical significance where p⩽0.05. Pneumonia scoring and formal microbiology were not assessed.
Results Of 784 admissions, 570 (72.7%) were primarily respiratory related and, of these, 199 (35%) had radiological evidence for pneumonia. The group with pneumonia (n = 199) tended to have longer length of stay (median 7 (interquartile range 3–14) vs 6 (3–10) days, p = 0.005), to be older (77 (69–82) vs 71 (63–79) years, p = 0.001), featured more men (54% vs 44%, p = 0.021) and were less likely to have supported early discharge (17% vs 26%, p = 0.044) than those without pneumonia (n = 371). Importantly, despite no difference in the mean number of admissions during this period, the group with pneumonia also reported more inpatient mortality (22/199 vs 15/371, p = 0.001).
Conclusions The data identified that about one-third of patients admitted with COPD at this hospital have radiology-reported evidence of concurrent pneumonia and an at risk of older men who then also share worse clinical outcomes including longer length of stay and inpatient mortality.
P103 BIOLOGICAL, PHYSIOLOGICAL AND SUBJECTIVE BIOMARKERS IN COPD SUBJECTS AT STABLE STATE AND EXACERBATION: AN OBSERVATION
1M. Bafadhel, 1S. Terry, 1S. McKenna, 1V. Mistry, 1C. Reid, 2M. McCormick, 2P. Rugman, 2P. Dodson, 2M. Saunders, 1I. D. Pavord, 1C. E. Brightling. 1Institute of Lung Health, University of Leicester, Leicester, UK, 2AstraZeneca, Charnwood, Loughborough, UK
Introduction Pulmonary and systemic inflammation is present in patients with chronic obstructive pulmonary disease (COPD) during periods of stability, with increased inflammation, worsened lung function and health status during exacerbations. Current management of exacerbations includes oral corticosteroids and antibiotics if there is an associated increase in sputum purulence. The effect of different aetiologies during an exacerbation may give rise to different inflammatory responses, and thus may provide a biomarker platform for aetiological diagnosis, targeted therapy and/or inflammatory modulation in a heterogeneous disease.
Aims To assess biological, physiological and subjective biomarkers in subjects with COPD during stable state and exacerbations.
Methods 145 subjects with COPD (GOLD I–IV) entered a 12-month longitudinal study looking at biomarkers at stable state (3-monthly visits) and exacerbations (table 1). Health status was measured using the chronic respiratory health questionnaire (CRQ) and the visual analogue score (VAS). Spirometry was undertaken pre and post salbutamol bronchodilation, while spontaneous/induced sputum and blood were processed and analysed for cellular differential and free supernatants using the meso-scale platform (MSD, Maryland, USA) which included 26 cytokines and chemokines (inflammatory panel), growth factors and acute phase reactants (vascular/hypoxia panel). Neopterin (serum and sputum) was measured using ELISA and PCT (serum) was measured using the Kryptor platform (BRAHMS, Germany).
Baseline demographic data of subjects
Results 145 baseline visits and 182 exacerbations were captured. The mortality rate was 9% during the study. Comparing stable state and exacerbations in all subjects, there was a significant worsening in mean (SEM) forced expiratory volume in 1 s (l), CRQ and VAS (mm) (1.34 (0.05) vs 1.10 (0.04), p<0.0001; 16.4 (0.4) vs 12.2 (0.3), p<0.0001; 142 (7) vs 243 (6), p<0.0001). There was a significant increase (p<0.01) in total blood leucocytes, blood neutrophils, C-reactive protein and airway inflammation. We observed significant increases in serum interleukin (IL)-6, serum amyloid A (sAA1) and in sputum IL1β, IL6, IL6r, tumour necrosis factor α (TNFα), TNFR1, TNFR2, CCL3 (MIP-1), CCL13 (MCP4), CCL17 (TARC), CCL5 (RANTES), CXCL10 (IP-10) and sputum neopterin.
Conclusions In subjects with COPD there is a measurable increase in systemic and pulmonary inflammation during an exacerbation and an associated decline in health status and lung function. Whether these biomarkers increase differentially in response to different aetiologies needs further investigation.
P104 SERUM PROCALCITONIN AND C-REACTIVE PROTEIN IN PATIENTS HOSPITALISED WITH PNEUMONIA, ASTHMA OR COPD
1T. Clark, 2M. Bafadhel, 2C. Reid, 3M. Medina, 3M. Barer, 1K. Nicholson, 1C. E. Brightling. 1Department Infectious Diseases, University Hospitals of Leicester, Leicester, UK, 2Institute of Lung Health, University of Leicester, Leicester, UK, 3Department of Medical Microbiology, University of Leicester, Leicester, UK
Background Pneumonia and acute exacerbations of asthma or chronic obstructive pulmonary disease (COPD) comprise a large proportion of hospital admissions and are a major cause of morbidity and mortality. Antibiotics are not recommended for acute asthma and are only recommended in COPD exacerbations if severe or if clinical features suggest a bacterial cause. Despite these recommendations, overuse of antibiotic therapy in airways disease continues. A simple biomarker to guide the use of antibiotic therapy is required. Serum C-reactive protein (CRP) and procalcitonin are elevated in bacterial infection and have been used to guide treatment in lower respiratory tract infection. For procalcitonin a cut-off value of 0.25 ng/ml has been proposed to guide antibiotic usage.
Aims To compare serum procalcitonin and CRP concentrations in hospitalised patients with pneumonia and exacerbations of asthma or COPD.
Methods Serum samples were available from hospitalised subjects during the winter months of 2006–8 with a diagnosis of pneumonia, exacerbation of asthma or COPD (as defined by ICD-10 diagnosis and chest radiographic changes). Serum procalcitonin was measured in duplicate using TRACE kryptor technology (BRAHMS, Germany) with a lower limit of detection of 0.02 ng/ml.
Results Procalcitonin and CRP were significantly higher in subjects hospitalised with pneumonia compared with those with exacerbations of COPD and asthma (p<0.001, table 1). Using a cut-off value for procalcitonin of 0.25 ng/ml, 5%, 35% and 73% of subjects with asthma, COPD exacerbation or pneumonia, respectively, would have received antibiotics. Using a receiver-operator curve for procalcitonin for pneumonia (antibiotics required) versus asthma (no antibiotics required), the area under the curve (AUC) was 0.91 and a cut-off of 0.07 ng/ml had a sensitivity of 85% and specificity of 85%. For CRP the AUC was 0.96 and a cut-off of 37 mg/l had a sensitivity of 90% and specificity of 90%. There was a significant correlation between procalcitonin and CRP (rs = 0.56, p<0.001).
Clinical characteristics at admission
Conclusion Serum procalcitonin and CRP are elevated in hospitalised patients with pneumonia compared with those with exacerbations of asthma or COPD. Both biomarkers can be used to reduce antibiotic therapy in these groups, but procalcitonin does not offer any benefit over CRP.