Article Text

Statistics from Altmetric.com
P70 ETHNIC DIFFERENCES IN VITAMIN D LEVELS AMONG PATIENTS WITH TUBERCULOSIS IN SOUTH-EAST LONDON
1J. K. Randhawa, 2V. Kahr, 3F. A. Post, 1R. D. Barker, 2H. J. Milburn. 1King’s College Hospital, London, UK, 2St Thomas’ Hospital, London, UK, 3Academic Department of HIV/GU Medicine, King’s College London, London, UK
Introduction and Objectives Vitamin D deficiency may be associated with tuberculosis (TB) disease; this relationship remains ill-defined. Somalis represent a significant proportion of our TB workload, hence we have an interest in this group. We carried out a retrospective analysis of vitamin D levels in patients with TB to determine any associations between age, gender, disease site or ethnicity.
Methods Patients with TB at two hospitals in south-east London from January 2004 to January 2009 were analysed. Vitamin D levels taken within 1 month of TB diagnosis were included. Patients were categorised by country of birth: Somalia, Africa (not Somalia), south Asia (India, Pakistan, Bangladesh, Sri Lanka) and the rest of the world. Data collected included age, gender, disease site and HIV status.
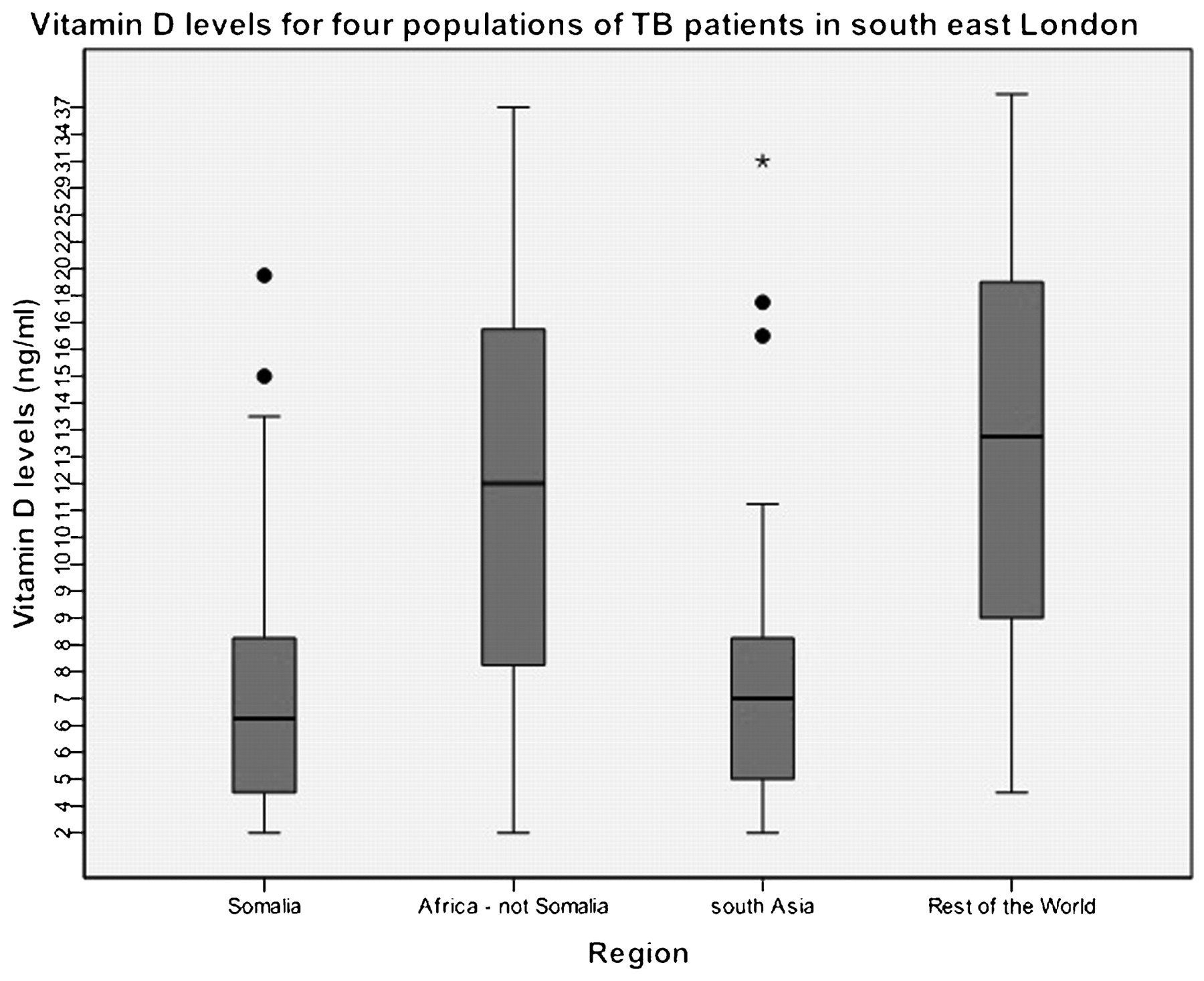
Results We identified 1190 patients, with complete data in 195 (16.4%). There were 36 (18.5%) patients from Somalia, 63 (32.3%) from Africa (not Somalia), 26 (13.3%) from south Asia and 70 (35.9%) from the rest of the world. All groups had deficient levels of vitamin D (<60 ng/ml); these were significantly lower in those from Somalia and south Asia compared with Africa (not Somalia) or the rest of the world (p<0.001, fig 1). Levels of vitamin D were similar between men and women. There was a suggestion of a U-shaped relationship between vitamin D levels and age (p = 0.21). There was no significant difference in vitamin D levels in patients with pulmonary TB (mean 12.9 ng/ml) compared with extrapulmonary TB (mean 11.3 ng/ml). There was no association between vitamin D level and HIV status.
{kind=link}
Vitamin D levels for four populations of TB patients in south-east London.
Conclusions Patients from Somalia and south Asia had lower levels of vitamin D than patients from other countries. This may not be related to skin tone alone, as patients from Africa (not Somalia) had levels comparable with the rest of the world. The reason for these differences is unclear, but could be related to genetic differences in vitamin D receptor polymorphisms, diet or culture. Vitamin D deficiency does not appear to be associated with extrapulmonary TB or HIV disease, although further sub-analyses in individual ethnic groups with larger numbers may be useful.
P71 “FIND&TREAT”: TOUGH TIMES IN THE TUBERCULOSIS CAPITAL OF EUROPE
1A. Story, 1S. Hemming, 2M. Lipman. 1Find&Treat, Department of Health TB Projects, London, UK, 2The Royal Free Hampstead NHS Trust, London, UK
Background “Find&Treat” (F&T) is a Department of Health-funded initiative to strengthen tuberculosis (TB) control among hard-to-reach populations. The team of TB nurse specialists, social and outreach workers work directly with TB and allied frontline providers across London to tackle TB and suspected TB among homeless people, problem drug and alcohol users and prisoners (hard-to-reach). F&T provides an active case finding service with the Mobile X-ray Unit (MXU), supports case management and Directly Observed Therapy (DOT), provides training and raises awareness and locates and re-engages patients who are lost to follow-up. Our holistic approach advocates for case management to ensure completion of diagnostic investigations and DOT from onset for all hard-to-reach patients. Between October 2007 and June 2009 we have given practical support and advice to TB services across London for 481 suspected and confirmed TB cases with complex and challenging needs. Here we provide an overview of our work so far and its impact on the management of socially complex TB cases in London.
A Complex and Challenging Caseload 263 (55%) referrals were from TB services, 137 (28%) through mobile screening, 46 from prisons and the remainder from allied agencies in the homeless, drugs and alcohol sector or directly from Health Protection Units. The main reasons for referrals were to ensure completion of diagnostic investigations (193), treatment (147) and to re-engage patients lost to follow-up (139). 77% of referrals were men and 32% were UK-born. Where known, 71% (289/405) have complex social problems including homelessness, drug (heroin, base/free-base cocaine) and alcohol dependency and recent imprisonment. Of the 275 active TB cases referred, 81% had pulmonary disease of which 60% were sputum smear-positive at diagnosis. More than one-third of culture confirmed cases (158) had drug-resistant TB (isoniazid mono-resistant, 22%; rifampicin mono-resistant, 3%; multidrug resistant (MDR), 9%). TB services are able to provide DOT for only half (58) of the 103 cases currently taking treatment. So far, 109 cases have been confirmed not TB.
Conclusion Tackling TB among hard-to-reach populations in the capital is a major public health challenge that requires a co-ordinated pan-London multi-disciplinary and multi-agency approach.
Funding source: Department of Health.
P72 “FIND&TREAT”: RETURNING THE LOST BACK TO LOCAL TUBERCULOSIS SERVICES
1A. Story, 1P. Windish, 1J. Hall, 2M. Lipman. 1Find&Treat, Department of Health TB Projects, London, UK, 2The Royal Free Hampstead NHS Trust, London, UK
Background A major element of the work of “Find&Treat” (F&T) is to find and return to services patients with tuberculosis (TB) who have become lost to follow-up (LFU). Prior to F&T there was no standardised response to LFU in London and, in most cases, patients were effectively “discharged” after unsuccessful appointment reminders and a home visit. There is no internationally agreed or standardised definition for LFU in TB prevention and control. This abstract describes the profile of these patients, presents the practical steps undertaken by F&T to return patients with active TB to treatment services and the outcomes of the return to service work to date.
Profile of LFU Cases Since October 2007 TB services have referred to us 133 hard-to-reach active cases who disengaged prior to treatment completion. 74% of LFU cases were men and 34% were UK-born. The majority (77%) had pulmonary TB of who 55% were sputum smear-positive at diagnosis. Two-thirds (88/133) of the cases were culture confirmed, of whom 20 had drug-resistant disease (4 multidrug-resistant (MDR)); 16 of them were smear positive. Despite a very high prevalence of complex social problems, only 38% of LFU cases received Directly Observed Therapy from treatment onset.
Practical Steps We developed a working definition and systematic approach to managing LFU and return to service which sought to identify diagnosed and suspected cases who could potentially harm either themselves or others by not completing prescribed treatment or relevant investigations. We search local and national shared databases used by the NHS, housing and criminal justice agencies, day centre and drugs agency networks and by outreaching alongside colleagues in allied agencies across London.
Outcome To date, two-thirds (89) of patients have been found and returned to treatment services, including 10 drug-resistant cases (4 MDR). Of those found, 29 are on treatment, 34 completed treatment, 5 died of TB and 6 were transferred out. In 15 cases, local clinicians decided to stop treatment as the case was considered too socially chaotic to treat. This work demonstrates that it is possible to find and return hard-to-reach patients to treatment services and highlights the potential public health impact of LFU.
P73 THE CHANGING EPIDEMIOLOGY OF TUBERCULOSIS IN CENTRAL MANCHESTER
S. Singhania, C. Bell, M. Woodhead. Manchester Royal Infirmary, Manchester, UK
Introduction We sought to describe the changing epidemiology of tuberculosis (TB) in Central Manchester over last 13 years.
Methods Tuberculosis data for last 13 years from the TB unit at Manchester Royal Infirmary were analysed and compared with the UK data reported by the Health Protection Agency (http://www.hpa.org.uk).
Results The annual number of cases of TB has grown from 43 in 1996 to 146 in 2008, a 344% rise. The age group 15–45 years constitutes 64% of the total cases. This proportion has remained constant over last 8 years (63% in 2001). The largest number of TB patients is from the Indian subcontinent (45–50%). Although the black African population is one-third of the Indian subcontinent population, there has been a constant rise in the number of black African cases which currently constitutes 30% of the total cases of TB compared with 16% in 2000. The proportion of Caucasian cases has halved (currently 15%) since 1996 but the absolute numbers has doubled (12 in 1996, 23 in 2008). The proportion of non-UK-born patients has also gone up from 62% to 75% currently. There is a high incidence of extrapulmonary cases (55%) compared with the national data (45%). The proportion of sputum positive cases was 23% in 1997 and has increased to 43% in 2008. Samples were taken in 75% of the cases and, among them, 70% of patients have positive cultures for TB. The incidence of isoniazid resistance (6%) is similar to the national figure (7%) and is increasing (2.3% in 1996), but multidrug-resistant TB and other mono drug resistance still remains less than 1%. HIV co-infection is currently seen in 6% of the cases and has become more common in the last 5 years (2.9% in 2003). The proportion of patients completing TB treatment has consistently remained constant (81% in 1996, 84% in 2007).
Conclusion The disproportionate rise in cases of TB in Manchester emphasises that TB is an inner city disease. The changing epidemiological pattern of TB poses new challenges to the TB unit in Central Manchester.
P74 CLINICAL EPIDEMIOLOGY OF TUBERCULOSIS IN SOMALIS IN SOUTH-EAST LONDON
1V. P. Kahr, 2J. K. Randhawa, 3F. A. Post, 4L. V. Baker, 5T. C. Stokes, 1H. J. Milburn, 2R. D. Barker. 1St Thomas’ Hospital, London, UK, 2King’s College Hospital, London, UK, 3Academic Department of HIV/GU Medicine, King’s College London, London, UK, 4University Hospital Lewisham, London, UK, 5Queen Elizabeth Hospital, South London Healthcare Trust, London, UK
Introduction and Objectives According to the last UK census (2001), 43 515 Somalis are living in the UK, 78% in London. This population contributes a high number of patients with tuberculosis (TB). Given the importance of Somalis to our TB burden, we decided to characterise their pattern of disease and compare it with other ethnic groups in south-east London.
Methods We obtained data from four hospitals using local databases and the London TB register. Patients diagnosed with TB disease from January 2004 to January 2009 were included. Patients were divided into four categories by country of birth: Somalia, Africa (not Somalia), south Asia (India, Pakistan, Bangladesh, Sri Lanka) and the rest of the world. Data collected included site of disease, HIV status and drug resistance. Data were extracted from an SQL server database and analysed using SPSS Version 17.
Results We identified 2267 patients; the data are summarised in table 1. Country of birth was not ascertained for 217 (9.6%) patients. Patients from Somalia were relatively young and more often women. They were rarely HIV positive and commonly had extrapulmonary disease. This was similar to patients from south Asia. Common extrapulmonary sites of TB for Somalis were cervical lymph nodes (n = 54, 21.8%), mediastinal lymph nodes (n = 26, 10.4%), gastrointestinal tract (n = 20, 8%) and spine (n = 20, 8.0%). Drug resistance was highest in Somalis, largely due to increased numbers of isoniazid (17.8%) and streptomycin (15.7%) resistance. There was little rifampicin resistance (<1%).
Conclusions Patients from Somalia have a high incidence of TB and a distinct pattern of disease. They have higher rates of extrapulmonary TB and a low rate of HIV, which is similar to patients from south Asia. Given the low rates of HIV in these patients, the aetiology of the high TB incidence in these groups remains obscure. Understanding the characteristics of TB disease in different ethnic groups could reduce diagnostic delay by increasing clinical suspicion. The high rate of isoniazid resistance among these patients may have contributed to the national increase in isoniazid resistance. The low rate of rifampicin resistance, and therefore multidrug resistance, is reassuring.
P75 SCREENING PRISONERS FOR TUBERCULOSIS: WHAT SHOULD THE UK DO?
1S. Yates, 2A. Story, 3A. C. Hayward. 1HMP Pentonville, London, UK, 2Find&Treat, Department of Health TB Projects, London, UK, 3UCL Centre for Infectious Disease Epidemiology, London, UK
Background NICE recommends that prisoners should be screened for tuberculosis (TB) by a health questionnaire on each prison entry followed by chest radiography for those with symptoms of active TB. This approach is at odds with other European countries where chest radiography on entry is recommended for all prisoners irrespective of symptoms. We sought to assess the potential impact on case detection of limiting chest radiography to only those prisoners who had symptoms of TB.
Method We collected data on symptoms compatible with active pulmonary TB (cough, night sweat, fever, weight loss and haemoptysis) from 5616 otherwise healthy prisoners and 30 prisoners diagnosed with active TB through the Mobile X-ray Unit (MXU). Of the cases, 80% were culture confirmed. From these data we were able to estimate the proportion of prisoners who would require chest radiography based on these symptoms alone or in combination and the proportion of active cases that would be missed were the screening to have been restricted to symptomatic prisoners.
Results Untargeted screening identified a prevalence of active pulmonary TB of 202 per 100 000 population giving a number needed to screen (NNS) to identify one case of 495. Restricting chest radiography to prisoners with cough (>2 weeks duration) would reduce the proportion of all prisoners screened to 22% (95% CI 21% to 23%) with an NNS of 182 but would miss 40% of all active pulmonary cases (95% CI 22% to 57%). Addition of extra symptoms further reduces the NNS but substantially increases the proportion of cases missed.
Conclusions Symptoms compatible with active pulmonary TB are common among prisoners in London. The current UK recommendation to restrict chest radiography to prisoners with symptoms of active TB is likely to lead to many missed opportunities to diagnose cases and prevent further transmission. Recently, and following early work by the MXU in prisons, the Department of Health has funded a project to install static X-ray screening units in eight key feeder prisons, with the local PCTs agreeing to undertake systematic screening in these prisons for all new entrants.
Funding source: Department of Health.
P76 TUBERCULOSIS IN LONDON AND OTHER ENGLISH CITIES: IS THE CAPITAL THE SPECIAL ONE?
1M. E. Kruijshaar, 1I. Abubakar, 1J. P. Crofts, 2M. Lipman. 1Health Protection Agency, Centre for Infections, London, UK, 2Royal Free Hospital, Respiratory Medicine, London, UK
Introduction Nearly half of all tuberculosis (TB) cases in England are from London, and the majority of the recent national increase is often attributed to rises in the capital. Although high rates of TB are also found in other urban areas, it is unclear whether London’s trends are reflected elsewhere.
Aim To compare the rate and characteristics of TB cases in London with that of other large urban English conurbations.
Method TB cases reported to the Enhanced Tuberculosis Surveillance (ETS) system between 1999 and 2006 were included if reported from London or from an urban area with a population of >400 000 in the 2001 census. Rates were calculated using mid-year estimates provided by the Office for National Statistics. Case characteristics were compared using the χ2 test and trends over time with the χ2 trend test.
Results The overall rate of TB in London was 45/100 000 in 2006 compared with 19/100 000 in the 12 other major conurbations. This varied from 6/100 000 in Brighton to 69/100 000 in the Leicester urban area. Between 1999 and 2006 the number of cases in London rose faster than in other areas (2308 to 3362 vs 1783 to 2450, p = 0.007), although the incidence rate increased at a similar pace (39% increase in London vs 35%). In London, cases were more often non-UK-born (73% vs 56%, p<0.001), of non-white ethnic group (86% vs 77%, p<0.002) and younger (65% aged 15–44 vs 54%, p<0.001). The proportion of non-UK-born cases in the other urban areas rose from 54% in 1999 to 70% in 2006, while in London this stabilised from 2000 at around 82%.
Discussion The burden of TB in the largest conurbations in England varied substantially, with London seeing the greatest number of cases and Leicester reporting the highest rates. Although cases in London are more often non-UK-born, younger and of non-white ethnicity, the increasing trend in the proportion of non-UK-born cases in other urban areas suggests a similar pattern is emerging in these areas. This argues for a specific urban TB control policy which can be implemented nationally.
P77 INCONSISTENT AND INCOHERENT METHODS OF SCREENING NEW ENTRANTS TO THE UK FOR TUBERCULOSIS
1M. Pareek, 2I. Abubakar, 3P. J. White, 1G. P. Garnett, 4A. Lalvani. 1Department of Infectious Disease Epidemiology, Imperial College London, London, UK, 2Tuberculosis Section, Health Protection Agency, London, UK, 3Modelling and Economics Unit, Health Protection Agency, London, UK, 4Tuberculosis Research Unit, Imperial College London, London, UK
Background Notifications for tuberculosis (TB) in the UK increased by 30% between 1992 and 2007, with overseas-born migrants accounting for 72% of UK cases of TB in 2007. This has refocused attention on TB screening for new entrants to the UK. Currently, new entrants are identified and screened with chest radiographs at the port of entry to determine whether they have active TB. Subsequent follow-up is determined by the initial screening results and devolved to local Primary Care Trusts (PCTs) who are responsible for completing the process. However, little is known about how PCTs follow up and screen new entrants referred from the port of entry.
Aims To investigate the processes and methods PCTs use in screening new entrants for TB, and whether this differs between low (incidence <20/100 000) and high (incidence ⩾20/100 000) TB burden PCTs.
Methods An anonymous 20-point questionnaire was administered to all 192 PCTs in the UK asking: which new entrants are followed up, who is screened for latent TB infection (LTBI) and how they are screened for LTBI. Descriptive analyses were undertaken. Categorical responses were compared using a χ2 test with a p value <0.05 considered significant.
Results 177/192 (92.2%) PCTs responded; 76.3% were low-burden PCTs. All 177 PCTs followed up abnormal chest radiographs. However, only 107/177 (60.4%) screened new entrants for LTBI; high-burden PCTs were significantly less likely than low-burden PCTs to screen new entrants for LTBI (OR 0.26, 95% CI 0.12 to 0.54, p<0.0001). Few new entrants had active TB diagnosed (median 0.0%, IQR 0.0–0.5%), but more had LTBI (median 7.85%, IQR 3.95–14.25%). PCTs which screened for LTBI varied in the new entrant subgroups they elected to screen (depending on TB incidence in the originating country), particularly in those aged 16–35 years where low-burden PCTs were significantly more likely to follow NICE guidance on who to screen (p = 0.047). Heterogeneity also existed in the protocols by which new entrants were screened for LTBI (table 1). More low-burden PCTs than high-burden PCTs used interferon-gamma release assays in diagnosing LTBI. Overall, 65.7% and 32.4% of PCTs followed NICE guidance on how to screen the <16 and 16–35 age groups, respectively.
Heterogeneity in the protocols and tools (including the uptake of interferon-gamma release assays) employed by different primary care trusts (PCTs) to screen for latent TB infection (LTBI)
Conclusions Considerable heterogeneity, inconsistency and lack of adherence to NICE guidance exist at all levels of the UK new entrant screening process. Current screening practices should therefore be re-evaluated in the context of the clinical and health economic evidence base to develop a nationally standardised cost-effective policy.
P78 SCREENING PATIENTS INITIATING ANTI-TNF AGENTS FOR MYCOBACTERIAL INFECTION USING INTERFERON-GAMMA RELEASE ASSAY: THE EXPERIENCE OF A LARGE INFLAMMATORY BOWEL DISEASE SERVICE
K. Greveson, C. Murray, C. Toumpanakis, L. Baptista, I. Cropley, M. Hamilton, M. Lipman. Royal Free Hospital, London, UK
Introduction Screening and treatment for latent tuberculosis infection (LTBI) is recommended by the BTS prior to initiation of treatment with anti-tumour necrosis factor (TNF) agents. Conventional screening involves assessment of risk factors, chest radiography and tuberculin skin testing (TST), which can be difficult to interpret in immunosuppressed subjects. Interferon-gamma release assay (IGRA) may detect Mycobacterium tuberculosis (Mtb) infection with greater specificity and possibly sensitivity compared with TST. Here we review our use of blood IGRA in patients with inflammatory bowel disease (IBD) initiating anti-TNF therapy.
Method A retrospective single-centre review was undertaken of patients with IBD either considered for or using anti-TNF agents assessed for evidence of Mtb infection with IGRA testing as part of their screening protocol. T SPOT-TB was the IGRA selected. Baseline assessment was undertaken by the IBD team, with onward referral to the TB service as needed.
Results Since 2008, 50 patients (24 anti-TNFα naïve, 26 established on anti-TNF) have been screened for LTBI using IGRA (table 1). Eight (16%) were born in TB endemic countries. All subjects had normal chest radiographs and a negative clinical assessment. Two patients (4%) had reactive Elispot results; one had a history of adequately treated pulmonary TB, was already using adalimumab and continued this after benefit/risk analysis; the other was treated for LTBI following the IGRA result. Two patients (4%) had an indeterminate Elispot result, both of which were non-reactive when repeated 2 weeks later. The remaining 46 patients had a non-reactive Elispot result. Nine patients (20%) were on no immunosuppression at the time of testing while 36 (80%) were taking azathioprine, prednisolone or mercaptopurine. Median follow-up to date is 5 months (range 1–8). No cases of active TB have occurred.
Conclusion The use of a simple screening protocol for LTBI incorporating IGRA in place of TST appears to work well in our specialist IBD service. Our detection rate for Mtb infection is consistent with other data, as is the proportion of indeterminate results. Longer term follow-up will indicate whether we have missed any LTBI using this assessment.