Article Text

Abstract
There is a need to re-evaluate the concept of asthma and chronic obstructive pulmonary disease (COPD) as separate conditions, and to consider situations when they may coexist, or when one condition may evolve into the other. Epidemiological studies show that in older people with obstructive airway disease, as many as half or more may have overlapping diagnoses of asthma and COPD (overlap syndrome). These people are typically excluded from current therapy trials, which limit the generalisability of these trials, and this presents a problem for evidence-based guidelines for obstructive airway diseases. Studying overlap syndrome may shed light on the mechanisms of COPD development. Overlap syndrome is recognised by the coexistence of increased variability of airflow in a patient with incompletely reversible airway obstruction. Patients typically have inflammatory features that resemble COPD, with increased airway neutrophilia, as well as features of airway wall remodelling. Overlap syndrome can develop when there is accelerated decline in lung function, or incomplete lung growth, or both. The risk factors for these events are shared, such that increasing age, bronchial hyper-responsiveness, tobacco smoke exposure, asthma and lower respiratory infections/exacerbations are significant risk factors for both incomplete lung growth and accelerated loss of lung function. Studying these events may offer new insights into the mechanisms and treatment of obstructive airway diseases.
Statistics from Altmetric.com
Asthma and chronic obstructive pulmonary disease (COPD) are the most common obstructive airway diseases in our community. Asthma is recognised as an allergic disease that develops in childhood, characterised physiologically by reversible airflow obstruction, and has an episodic course with a generally favourable prognosis, responding well to anti-inflammatory treatment. In contrast, COPD is typically caused by tobacco smoking, develops in mid to later life and is characterised by incompletely reversible airflow limitation that results in a progressive decline in lung function leading to premature death. While these are useful descriptions, they are limited because they do not fully depict the spectrum of obstructive airway disease that is seen in clinical practice. In particular, now that accelerated decline in lung function is recognised to occur in asthma, especially in those with asthma who smoke,1 and COPD is increasingly considered to be a treatment-responsive disease, there is a need to re-evaluate the concept of asthma and COPD as separate conditions, and to consider situations when they may coexist, or when one condition may evolve into the other. These are circumstances where asthma and COPD can overlap, and this review will examine these issues.
DEFINITIONS
The accepted definitions for the distinct obstructive airway diseases and their component syndromes are described in table 1. When a patient exhibits features of more than one condition, then they have an overlap syndrome. This review will address the overlap between asthma and COPD.
The current descriptions of asthma and COPD have been simplified into patterns of abnormal airway physiology (fig 1) which, in conjunction with symptoms, can be used to facilitate clinical recognition. There is a need to broaden these descriptions to accommodate the common clinical reality of people who fit the criteria for more than one condition.2 The American Thoracic Society 1995 COPD guidelines (fig 2)3 defined asthma, chronic bronchitis, emphysema, COPD and airflow obstruction, and identified 11 distinct syndromes. Overlap between two or more conditions made up 6 of these 11 syndromes. Further guideline development in COPD has placed more emphasis on recognising COPD as a disease where incomplete reversibility of airflow obstruction is the defining characteristic. This is useful since it allows easier recognition of obstructive airway diseases in general, and COPD in particular. However, the potential for overlap of the individual obstructive airway disease syndromes has received less attention.

Physiological patterns of airflow obstruction, expressed as forced expiratory volume in 1 s (FEV1), percentage predicted. Reversible AO, reversible airflow obstruction with improvement in FEV1 after bronchodilator; irreversible AO, incompletely reversible airflow obstruction, postbronchodilator FEV1 is <80%; irreversible AO+BDR, incompletely reversible airflow obstruction with significant bronchodilator responsiveness (BDR); irreversible AO+BHR, incompletely reversible airflow obstruction with significant bronchial hyper-responsiveness with fall in FEV1 after bronchoconstrictor. The label ‘asthma’ can be applied to reversible AO, irreversible AO+BDR and irreversible AO+BHR. Chronic obstructive pulmonary disease (COPD) can be applied to each of the conditions with irreversible AO+BHR. Overlap syndrome is present in irreversible AO+BDR and irreversible AO+BHR.
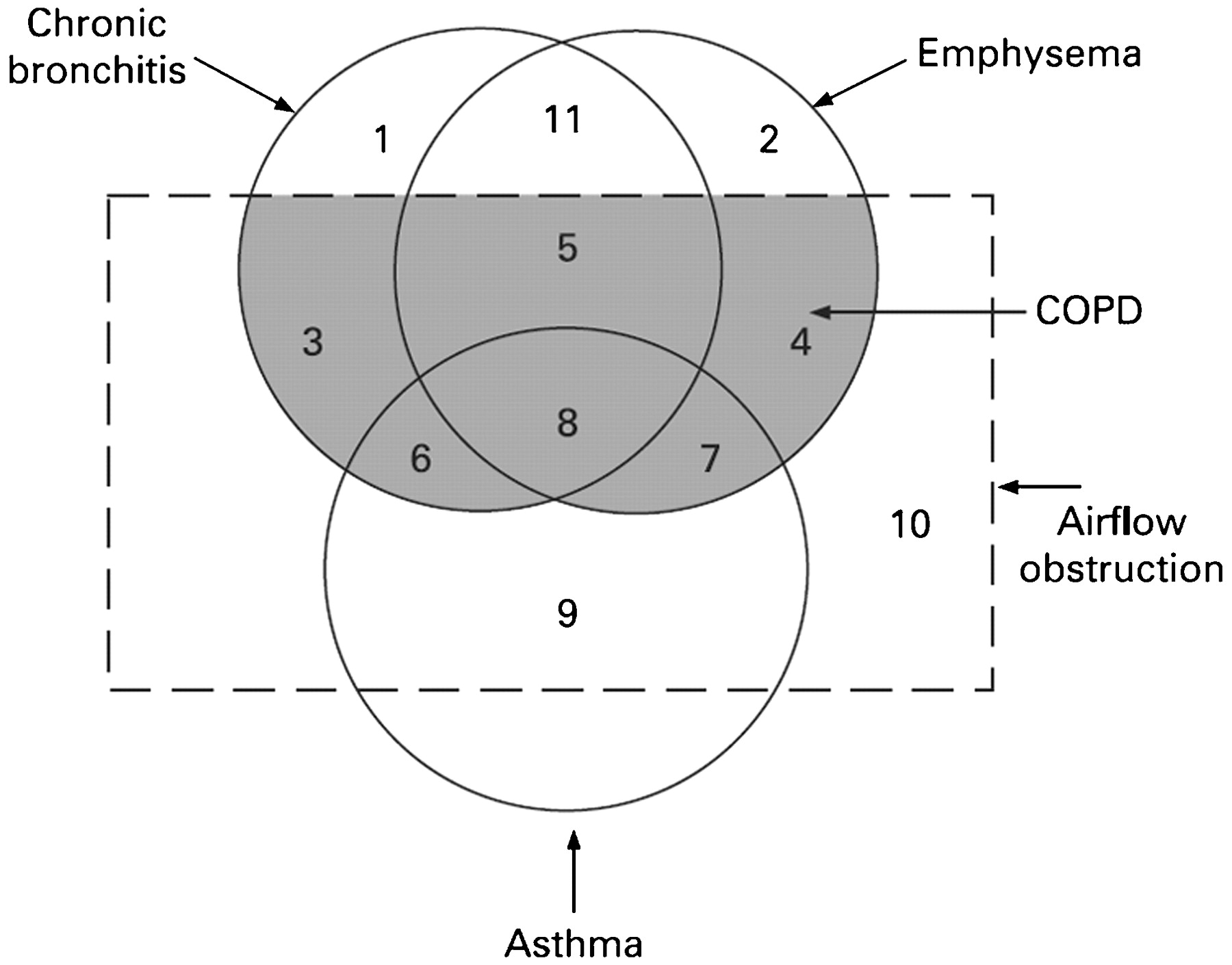
Non-proportional Venn diagram showing the number of overlapping conditions in patients with asthma, emphysema and chronic bronchitis (reproduced with permission from the American Journal of Respiratory and Critical Care Medicine). COPD, chronic obstructive pulmonary disease.
A recent study of the overlap in obstructive airway diseases using data from large population studies4 found that 17% and 19%, respectively, of patients had more than one condition present. With increasing age, there was a greater increase in the proportion of patients with obstructive lung disease who had overlapping diagnoses (fig 3). In older patients, a combined syndrome of asthma and COPD was the most common situation, as now confirmed using objective testing.5 Fewer than 20% of older patients have the classical phenotypes of emphysema alone or chronic bronchitis alone.

Percentage of adults (by gender) with airflow obstruction who have an overlap syndrome with increasing age. Males are shown in the black bars and females in the white bars. Data from Soriano et al.4
WHY IS IT IMPORTANT?
There are several reasons why the overlap syndrome is important. First, patients with overlapping asthma and COPD are excluded from clinical trials of treatment. This means that for an increasing proportion of older patients with obstructive lung disease, the data on efficacy of treatment may not be relevant. The clearest example of this comes from the studies on the efficacy of inhaled corticosteroids in asthma. These studies typically exclude smokers with asthma because of the difficulty in separating asthma from COPD in smokers with obstructive lung disease. However, up to 30% of people with asthma are smokers, and this means a substantial proportion of the population are excluded from randomised controlled trials. Extrapolation of the efficacy results for corticosteroids in non-smokers to smokers with asthma is flawed. Smokers with asthma have a relative corticosteroid resistance such that corticosteroids are much less efficacious in smokers with asthma than in non-smokers with asthma.6 This emphasises the need to study drug efficacy in relevant clinical populations, and the necessity to include overlap syndrome in drug evaluation programmes.
Secondly, clinicians are confused as to how and if they should differentiate asthma from COPD. In a study of the use of diagnostic labels for obstructive airway, many clinicians felt the need to extend the diagnostic label beyond asthma to indicate the presence of other clinical features, using additional terms such as asthma with chronic bronchitis, chronic obstructive bronchitis, asthma with permanent obstruction and COPD with a reversible component. The authors observed variation in the use of diagnostic labels for obstructive airway diseases, non-systematic use of current terms and uncertainty surrounding a short label such as asthma and whether it provided a sufficient case description.7
Thirdly, and perhaps more importantly, is that studying overlap syndrome may identify mechanistic pathways leading to the development of COPD. It is well known that patients with COPD typically present for care relatively late in the course of their disease, and that there is underdiagnosis of COPD in the community. By identifying common risk factors it may be possible to understand and modify the accelerated loss of lung function that leads to COPD. Several potentially important shared risk factors for overlapping asthma and COPD are increasing age, smoking, bronchial hyper-responsiveness (BHR) and exacerbations.
CLINICAL RECOGNITION AND INFLAMMATORY FEATURES OF THE OVERLAP SYNDROME: WHAT IS IT?
The clinical recognition of both asthma and COPD requires assessment of symptoms and physiological abnormalities (table 2). Symptoms can indicate the presence of a disease process; however, their sensitivity and specificity for asthma or COPD may be limited. At a physiological level, patients with overlap syndrome have evidence of incompletely reversible airflow obstruction (COPD) that can be detected by a reduced postbronchodilator FEV1 (fig 1). In addition, they have increased variability of airflow, which can be determined by increased bronchodilator responsiveness or BHR. The presence of airflow obstruction can confound the assessment of BHR in COPD. For recognition of the overlap syndrome, it may be preferable to use an indirect acting stimulus to assess BHR. Such agents do not directly cause airway smooth muscle contraction, and include hypertonic saline, adenosine and mannitol.
Informative data can be obtained from studies of discrete patient groups who have features of asthma and COPD. These groups include patients with asthma who smoke, those with asthma who develop incompletely reversible airflow obstruction and non-smokers who develop COPD. Smokers with asthma have features resembling COPD, since they are less responsive to corticosteroids and are less likely to have eosinophilic inflammation8 and more likely to have increased airway neutrophilia.9
The development of incompletely reversible airflow obstruction (COPD) is recognised to occur in some patients with long-standing asthma.10 11 These patients tend to be older, male, with a longer duration of disease, and have an increased risk of death from airway disease.12 13 A longitudinal study found that 16% of patients with asthma had developed incomplete airflow reversibility after 21–33 years of follow-up.14 The pattern of inflammation associated with asthma and incomplete reversibility of airflow obstruction is heterogeneous. Studies that exclude smokers find evidence of eosinophilic inflammation from increased exhaled nitric oxide (NO), increased blood eosinophils12 and increased airway eosinophils.15 This design naturally excludes an important portion of the asthma population and permits a selection bias.
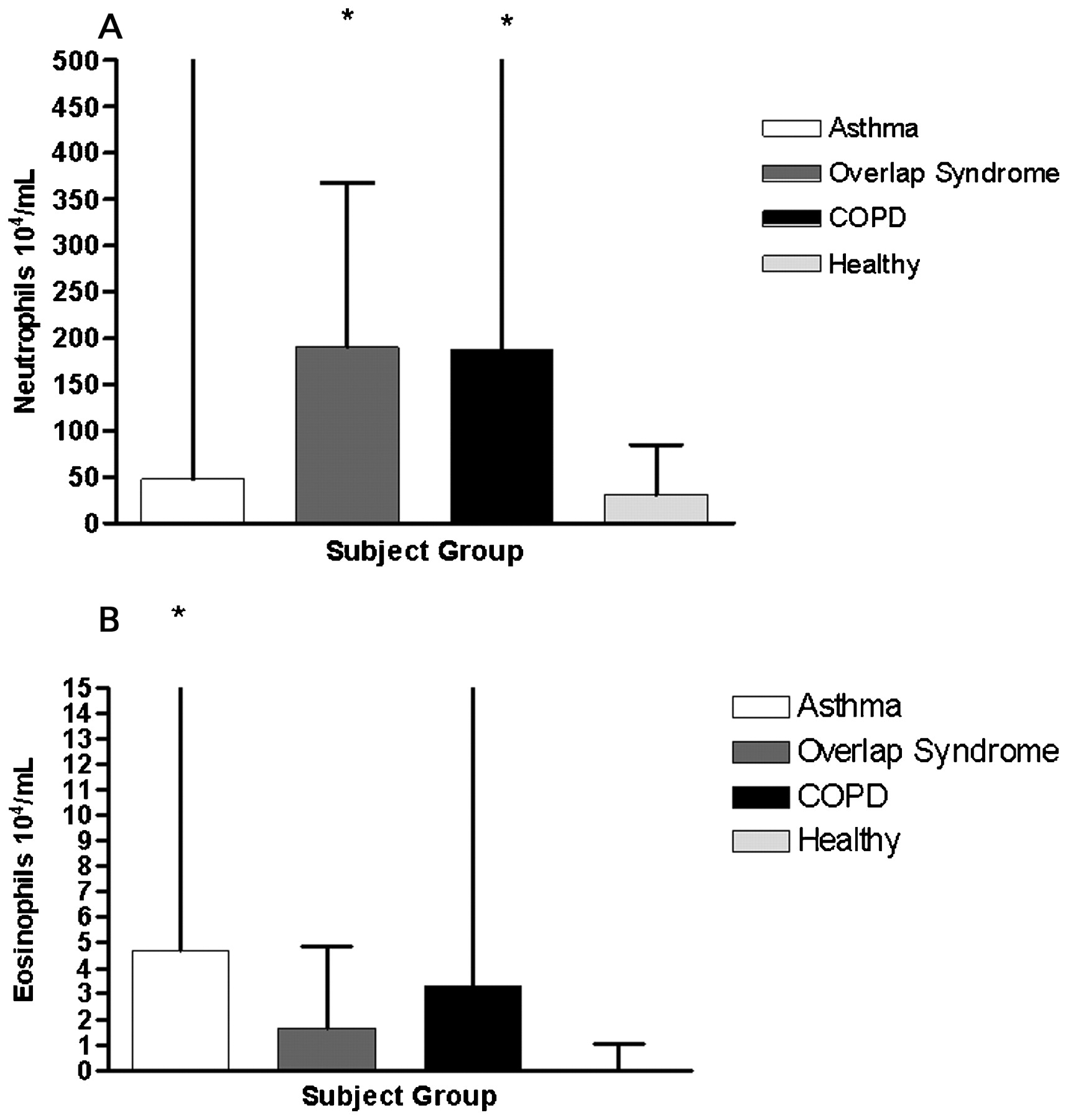
When unselected subjects with asthma and incomplete reversibility are studied, then there are increased airway neutrophils, with the intensity of neutrophilia correlated with the decline in FEV1.16–18 We studied 44 older (>55 years) adults with stable obstructive airway disease (asthma and/or COPD) to characterise the frequency of overlap syndrome, the pattern of airway complications and the pattern of airway inflammation. Sixty-five percent exhibited an overlap syndrome of asthma with COPD and only 16% and 21%, respectively, could be definitively categorised as asthma and COPD using the criteria in table 2. The participants with overlap syndrome and COPD were predominantly ex-smokers. Atopy was highest in asthma (100%) whereas in overlap syndrome the rate of atopy was intermediate (64%) between that of asthma and COPD alone (25%). Airway complications in the overlap syndrome, such as the need for oral corticosteroids, and presence of chronic bronchitis and bacterial colonisation, resembled COPD rather than asthma (fig 4). Sputum neutrophils and total cells were highest in those with overlap syndrome, where absolute numbers of neutrophils were up to five times higher than those with asthma alone and older healthy controls (fig 5A). Eosinophil numbers were significantly increased in those with asthma compared with healthy controls but not different between the groups with airway disease (fig 5B). Together these data confirm that the overlap syndrome of asthma and COPD is common in older people, has intermediate risk factor prevalence, but resembles COPD in terms of airway complications and the pattern of airway inflammation with increased airway neutrophils.

Airway complications and the overlap syndrome: percentage of patients with asthma (white bars), chronic obstructive pulmonary disease (COPD) (black bars) and overlap syndrome (grey bars) requiring oral corticosteroids for an exacerbation in the past year, with chronic bronchitis and with airway colonisation with bacteria.
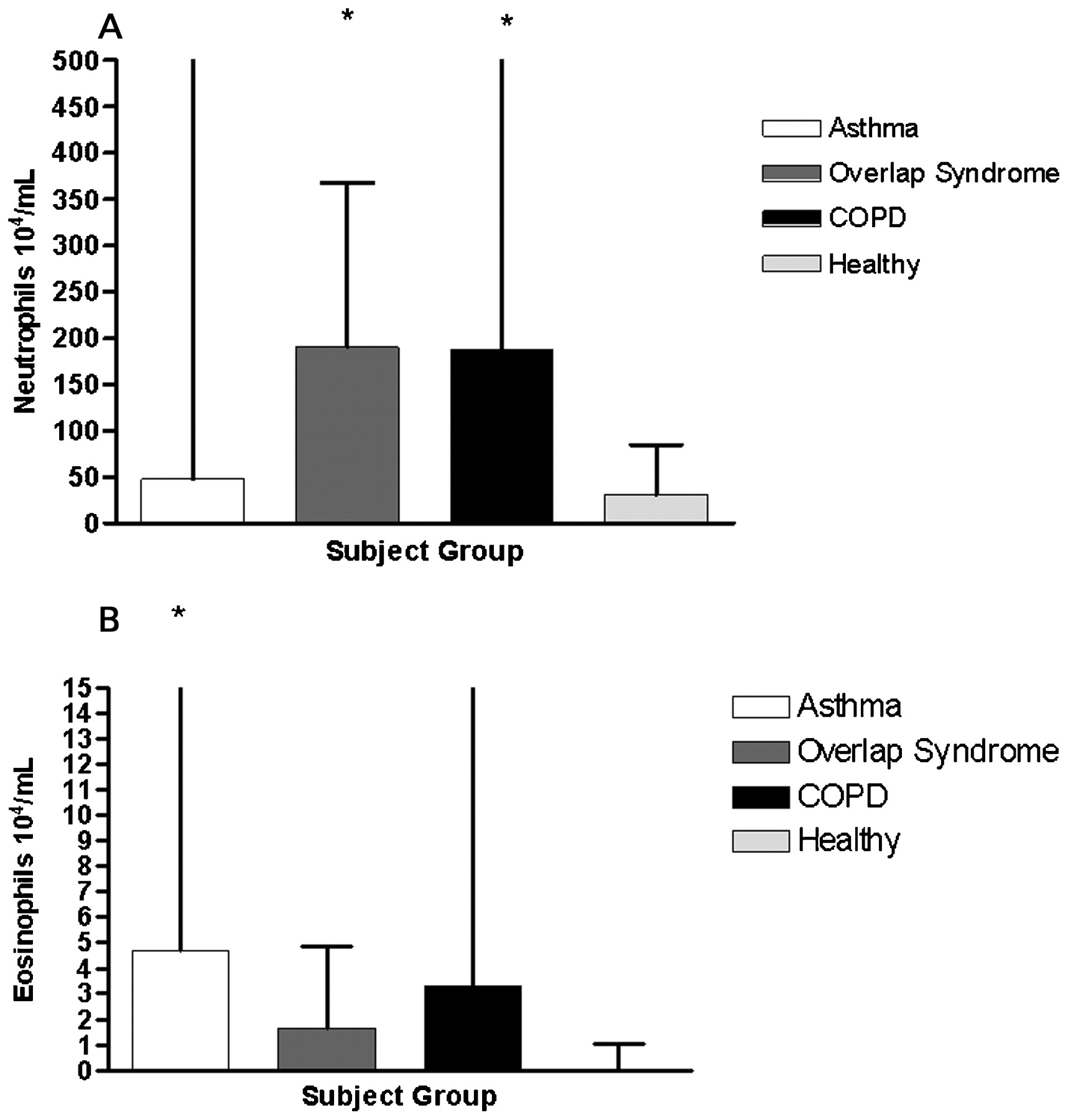
(A) Number (×104/ml) of sputum neutrophils in the airways of adults with asthma (white bars), chronic obstructive pulmonary disease (COPD) (black bars), overlap syndrome (dark grey bars) and healthy controls (light grey bars). * p<0.004 vs healthy controls. (B) Number (×104/ml) of sputum eosinophils in the airways of participants with asthma (white bars), COPD (black bars), overlap syndrome (dark grey bars) and healthy controls (light grey bars). *p<0.004 vs healthy controls.
Airway remodelling and the overlap syndrome
There is also increased airway wall remodelling in the overlap syndrome, with increased bronchial wall thickening on high resolution CT (HRCT).12 Increased thickness of the airway wall is an important feature leading to airway obstruction in most airway diseases.19 20 In asthma, this is due to inflammation, subepithelial fibrosis and increased thickness of the smooth muscle.21 There is also increased thickness of the airway wall in COPD, which is not as prominent as in asthma,22 but involves the same structures of the epithelium, reticular basement membrane, airway smooth muscle and mucous glands. There is also evidence of remodelling, fibrosis and inflammation in these structures.23 24 The increased smooth muscle reported in COPD is seen in some25 but not all studies. Increased thickness of the airway epithelium and goblet cell hyperplasia are features of the remodelled airway in both asthma and COPD. Similarly, increased airway wall fibrosis is reported in both asthma and COPD.23 24 26 Thus when considering the pathological changes within the airways that are associated with asthma and COPD, there is similarity in terms of structures that are remodelled, but differences in the degree of changes in specific structures.12
WHY IS THERE OVERLAP? WHY DOES IT OCCUR?
Overlapping asthma and COPD could occur for several reasons. Asthma and COPD are two common conditions, and by chance alone there will be overlap. The two conditions may also share common risk factors or origins, which means that one may evolve into the other. One expression of this possibility, the “Dutch hypothesis”, was proposed by Orie who suggested that BHR may be a risk factor for asthma and COPD.2 Another expression of the common risk hypothesis for overlap syndrome comes from the study of childhood diseases. Epidemiological studies have identified an association between childhood respiratory illness and impaired adult lung function.27 Airway growth starts in utero and continues throughout childhood into early adult years. Any diseases or exposures that lead to incomplete airway growth may also contribute to impaired adult lung function. In this way, fetal or childhood exposures may contribute to adult asthma and COPD.28
Adult COPD may therefore result from accelerated decline in lung function, failure to attain maximal airway growth or a combination of the two (box 1). An examination of lung growth through life shows evidence for both of these circumstances (fig 6). Identification of risk factors for these events will aid understanding of COPD and suggest ways to prevent the onset of COPD. Remodelling of airway structural elements is a key factor in airway growth, and is now recognised to be an important part of the pathological processes involved in asthma and COPD.21 This suggests that there will be overlap or commonality in the risk factors for impaired lung growth and accelerated decline in airway function. Epidemiological studies have shown this to be the case. Unexpectedly, there also appears to be risk factor potentiation, where each of the more common risk factors interacts with one or more other risk factors to potentiate the development of COPD. For example, smoking and asthma are independent risk factors for COPD, and smoking itself is a risk factor for asthma. Predictably, when the risks of combined asthma and smoking are examined, then the effects accumulate, and decline in adult lung function in smokers with asthma is greater than in asthma or smokers alone.1 29
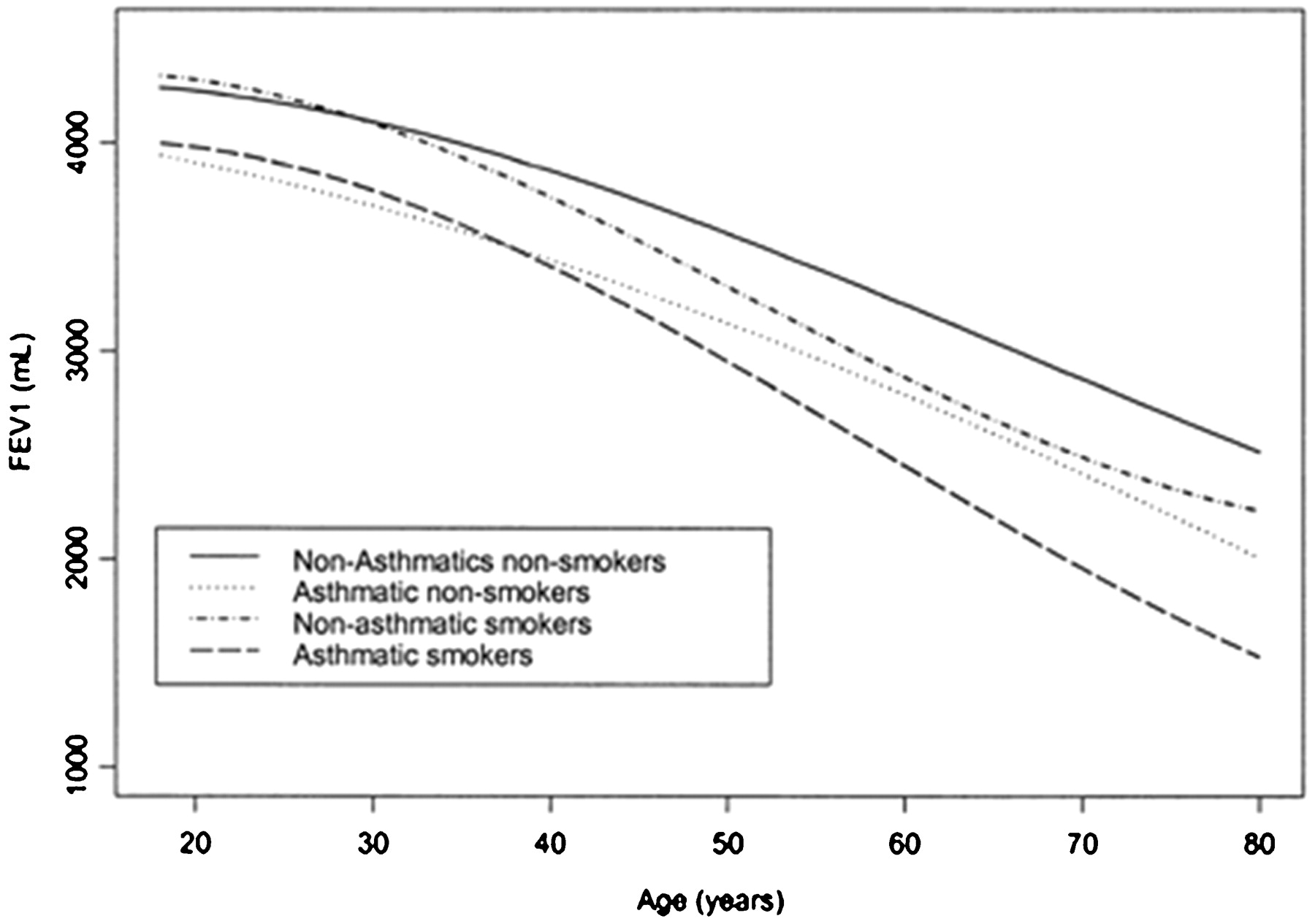
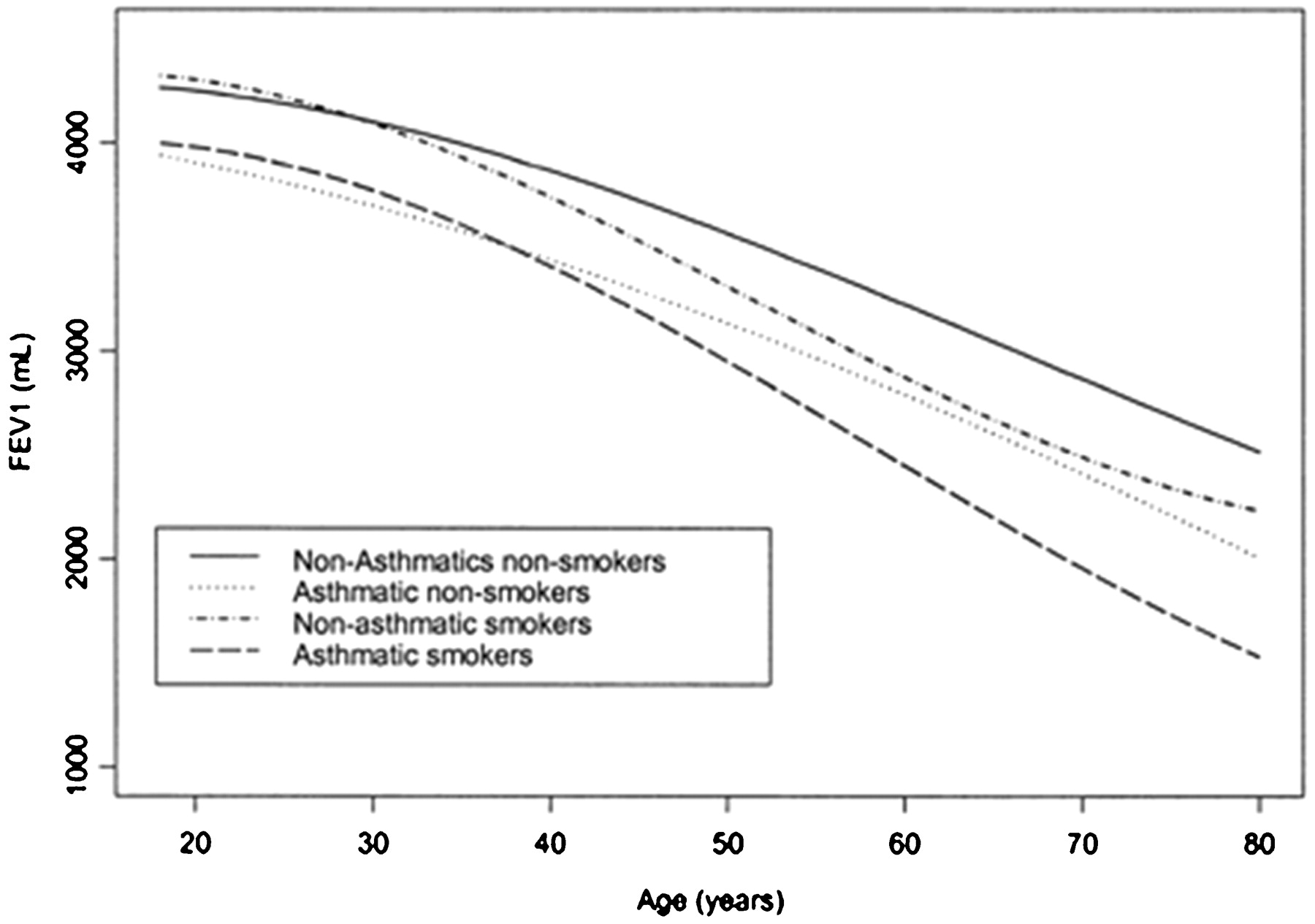
Forced expiratory volume in 1 s (FEV1) ml (corrected for height, weight and age at first survey) for males: non-smoking males without asthma (continuous line), non-smoking with asthma (dotted line), smoking without asthma (dashed and dotted line) and smoking with asthma (dashed line). (Reproduced with permission from the American Journal of Respiratory and Critical Care Medicine).
Pathways to chronic obstructive pulmonary disease (COPD)
Pathways to COPD
Accelerated decline in adult lung function
Incomplete lung growth during childhood
Common risk factors
Smoking
Bronchial hyper-responsiveness
Asthma
Exacerbation/infection
Risk factor potentiation
Asthma
Bronchial hyper-responsiveness
Smoking
Exacerbations
Other relevant risk factors
Gender
Body weight
Susceptibility genes
Accelerated decline in lung function
Since COPD represents incomplete reversibility of airflow obstruction, then any risk factor that leads to accelerated loss of lung function will contribute to the development of COPD. Several risk factors for accelerated decline in include age, smoking, BHR, asthma and exacerbations or lower respiratory infections. Increasing age is associated with decline in lung function, both in asthma and in those without asthma.1 29
Smoking
Loss of lung function is accelerated by smoking by up to 50 ml per year,29 30 and there is an established dose–response relationship.29 31 32 The loss of lung function with smoking may even be greater in those with asthma, such that smokers with asthma can develop COPD. Importantly, quitting smoking slows the decline in lung function. In the Lung Health Study, the annual decline in FEV1 in people who quit smoking at the beginning of the 11 year study was 30 ml/year for men and 22 ml/year for women. Continued smoking led to a decline in FEV1 of 66 ml/year in men and 52 ml/year in women.30
Bronchial hyper-responsiveness
BHR is present in between 10% and 20% of the population, and is frequently asymptomatic.2 33 The role of asymptomatic BHR in the development of asthma and COPD was investigated in the SAPALDIA (Study on Air Pollution and Lung Diseases in Adults) study. At baseline, 17% of the population had BHR to methacholine, and 50% of these were asymptomatic, giving a prevalence of asymptomatic BHR of 9%. Asymptomatic BHR was associated with an increased risk of developing newly diagnosed asthma, new symptoms of wheeze, chronic cough and a diagnosis of COPD after a 11 year follow-up period (table 3).34 Smoking led to an increased risk of developing BHR.35 36 This is an example of risk factor potentiation, where one risk for COPD positively interacts with another to potentiate the COPD risk.
BHR was also associated with an accelerated decline in lung function, and there was a significant interaction with smoking. There was a mean additional decline in FEV1 of 12 ml/year in current smokers and 11 ml/year in former smokers with BHR. Never-smokers with BHR also had an accelerated decline of 4 ml/year compared with asymptomatic participants without BHR. Thus active smokers with BHR were particularly at risk for the development of COPD. The mechanism is not known but may involve airway inflammation since induced sputum inflammatory markers were found to be increased in smokers with BHR.37
Asthma
Several epidemiological studies have identified that there is accelerated decline in lung function as a result of asthma and this positively interacts with smoking. The factors associated with accelerated lung function decline in asthma include more severe BHR,38 adult-onset asthma,39 frequent severe exacerbations,40 persistent symptoms,41 baseline airflow obstruction38 and persistent elevation of exhaled NO in difficult to treat asthma.42 There is clear evidence of risk factor potentiation, as many of the risks for accelerated lung function decline in asthma are also risk factors for lung function decline themselves—that is, smoking, BHR and severe exacerbations. Interestingly, baseline airflow obstruction, which is a risk for accelerated lung function decline, may result from incomplete lung growth as a result of childhood asthma or other childhood exposures, and is an example where the pathways to COPD (box 1) potentiate each other.
The deficits in lung function in asthma seem to arise early in the course of the disease,43 44 and may be an effect of incomplete lung growth.43 In one study, abnormal lung function at age 26 in patients with asthma was related to male sex, BHR at age 9 years, early onset of asthma and reduced lung function by age 9 years.41
Exacerbations
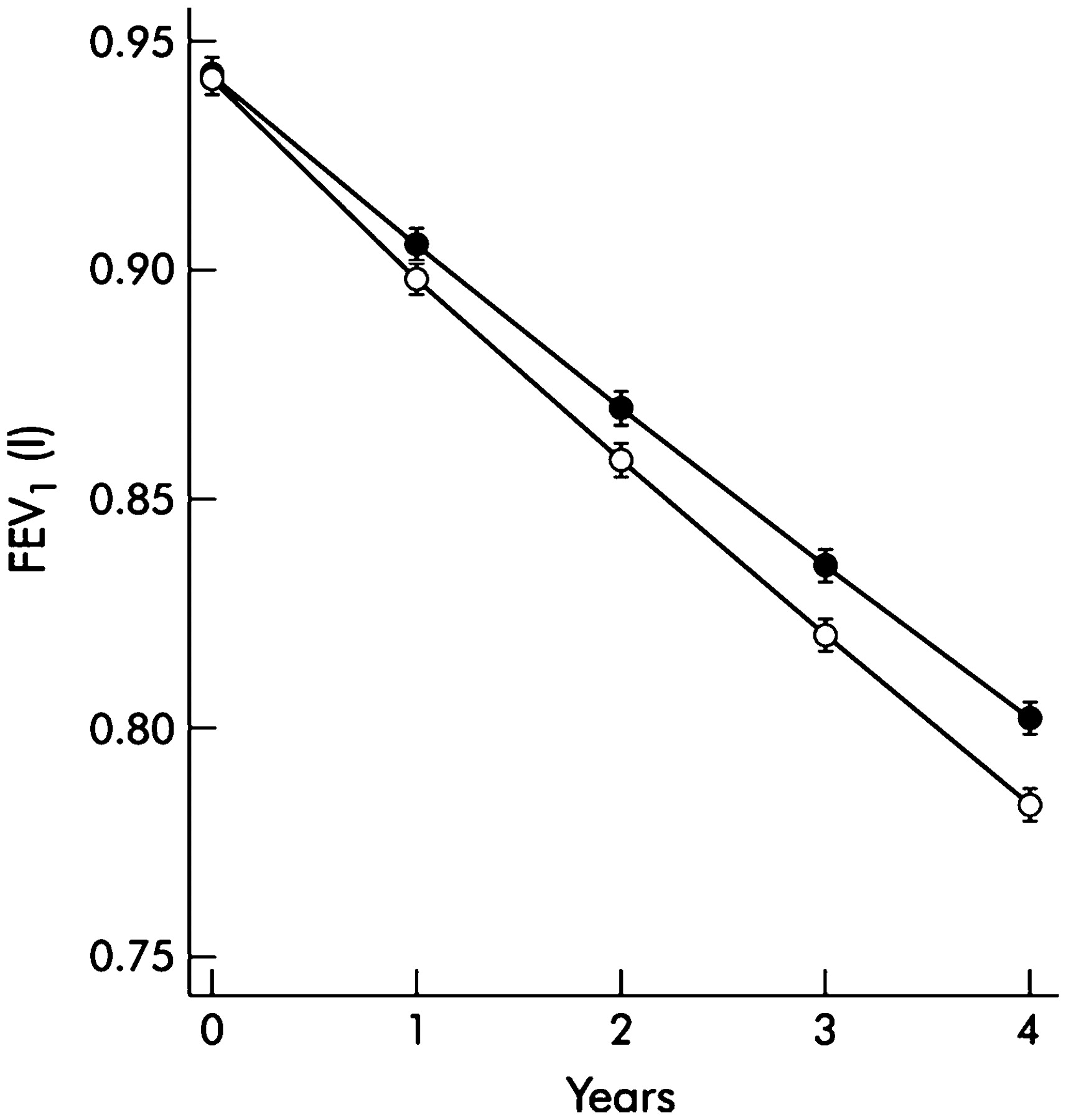
Both patients with asthma and those with COPD experience exacerbations of their disease. These are clinically significant events, frequently triggered by viral respiratory tract infection, and associated with quality of life impairment, loss of functional ability and increased healthcare utilisation. Recent data now show that disease exacerbations in both asthma and COPD45 46 (fig 7) can lead to accelerated loss of lung function. In asthma a longitudinal cohort study of patients with persistent asthma14 found a greater decline in FEV1 in those patients with frequent severe exacerbations. In a regression analysis, one severe exacerbation was associated with a 30 ml greater annual decline in FEV1. These results show that a severe asthma exacerbation is associated with accelerated FEV1 decline, to a similar degree as that seen with smoking and COPD. Another important observation was that the decline in FEV1 seen in infrequent exacerbators was not different from the population without asthma. This raises the possibility that modifying the exacerbation rate may prevent the onset of fixed airflow obstruction in asthma.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Annual change in forced expiratory volume in 1 s (FEV1) for patients with frequent (filled circles) and infrequent (open circles) exacerbations of chronic obstructive pulmonary disease (COPD). (Reproduced with permission from Thorax).
Childhood: risk factors for incomplete lung growth
Lung function in early adult life is a strong risk factor for the development of COPD. There is now evidence that poor lung function in infancy and childhood persists into adulthood, and that in utero events can modify airway function in early postnatal life. Stern et al studied lung function in infants soon after birth and found that poor airway function at that time was a risk factor for impaired adult lung function,45 suggesting that airway function throughout adult life may be determined during fetal development and the first few months of postnatal life.45 Maternal smoking adversely influences lung growth.46 In infancy there is an ∼15–20% reduction in airflow in children born to mothers who smoked during pregnancy.47 In addition, maternal smoking is associated with impaired fetal growth, and intrauterine growth retardation is itself associated with impaired airway function in infancy and later life.
Many of the risk factors for incomplete lung growth in childhood are similar to the risk factors for accelerated loss of lung function in adults, namely tobacco smoke exposure, asthma, BHR48 and exacerbations or respiratory infections. Additional risk factors include low birth weight, gender (lower in boys), nutrition and ethnicity.
Asthma
Several longitudinal studies show that at the commencement of adulthood, lung function is lower in people with asthma than in those without (fig 6).29 41 43 Impaired lung function has been observed in up to 25% of children in the Childhood Asthma Management Program49 and in children with eosinophilic asthma.52 This suggests that there may be incomplete lung growth with asthma, and this can be another pathway to the development of impaired lung function in adulthood.
There is an established relationship between smoking and asthma, with smoking potentiating the effects of asthma on respiratory ill-health. Surprisingly, there appears to be bi-directionality in the relationship between smoking and asthma. Studies have shown unexpectedly higher smoking rates in some groups with asthma, such as adolescents and pregnant women. Longitudinal studies among adolescents have identified that asthma is a risk factor for starting smoking and becoming a regular smoker.50
Early life infections
There is emerging evidence of a role for early life infections leading to impaired lung function and modification of asthma risk. For example, Barker studied lung function in adult men and found an association between respiratory infection during infancy and reduced adult lung function.51 Other studies show that respiratory viral infection modifies BHR, which is a risk for impaired lung function. Of equal importance is the now well-established observation that impaired lung function often precedes a viral-induced wheezing illness in childhood and leads to an increased likelihood of wheezing when a child subsequently develops a respiratory infection.52 This suggests a complex relationship between childhood respiratory infection and subsequent lung growth, and the need for more detailed mechanistic studies.
These events can be studied successfully in dynamic model systems. Chlamydia infection has been associated with asthma and may both cause acute infection and then enter a state of persistent infection with episodic reactivation.53 Chlamydia infection is also prevalent, and exposure can occur not only via respiratory infection, but during birth infants could be exposed to maternal Chlamydia, leading to the potential for early life Chlamydia exposure. When the effects of neonatal Chlamydia infection are examined in models of allergic sensitisation, then profound changes are seen. Neonatal Chlamydia infection leads to impaired lung growth with abnormal airspace enlargement. When combined with allergic sensitisation, then adult BHR is enhanced by neonatal Chlamydia infection, and there is enhanced airway remodelling with increased airway goblet cells, and abnormal airspace enlargement.53
CONCLUSION
Older people with symptomatic obstructive airways disease frequently have overlapping features of variable airflow obstruction (asthma) and incompletely reversible airflow limitation (COPD). They may have a prominent neutrophilic bronchitis and experience mucus hypersecretion. The overlap syndrome can occur due to accelerated decline in lung function and incomplete lung growth in children. These pathways share common risk factors of tobacco smoke exposure, BHR, asthma and respiratory infections. These risk factors may in turn co-occur and potentiate each other. In studying the pathogenesis of overlap syndrome, it will be fruitful to look for mediators that drive both airway inflammation and airway remodelling. Since patients with overlap syndrome are usually excluded from randomised treatment trials, the recommendations for management are necessarily extrapolated from trials of asthma alone or COPD alone. There is a need to extend drug efficacy studies to include patients with overlapping asthma and COPD, and address the many research opportunities to investigate the mechanisms and treatment of overlapping asthma and COPD in older people.
REFERENCES
Footnotes
Competing interests: None.
Funding: PGG holds an NHMRC Practitioner Fellowship and JLS holds am NHMRC Centre of Respiratory Research Excellence Fellowship.
Linked Articles
- Airwaves