Article Text

Abstract
Rationale: Wegener granulomatosis (WG) has previously been associated with increased nasal carriage of Staphylococcus aureus, but no studies have investigated the occurrence of pathogen growth in the lower airways.
Objectives: To culture bronchoalveolar lavage fluid (BALF) from patients with WG, patients with idiopathic pulmonary fibrosis (IPF) and normal controls.
Methods: 33 patients with WG, 22 with IPF and 8 normal controls underwent bronchoscopy and bronchoalveolar lavage. Quantitative culture established bacterial levels in the lower airways. Culture experiments were designed to investigate whether BALF is a supportive environment for S aureus growth. BALF cytokines were measured by ELISA.
Results: Pathogens were commonly grown from BALF of patients with WG and those with IPF. S aureus was particularly associated with patients with WG both in relapse and in remission. BALF levels of interleukin 1 receptor antagonist (IL1ra) were statistically significantly elevated in those patients who grew a pathogen from lavage fluid. BALF from patients with WG and IPF stimulated S aureus growth compared with normal lavage fluid.
Conclusions: Pathogens are more commonly isolated from BALF from patients with WG than from that of patients with IPF or normal controls, and with a different culture profile. IL1ra was associated with pathogen growth in WG and IPF. WG BALF is a trophic environment for S aureus growth. Pulmonologists treating patients with acute or relapsing WG should consider bronchoscopic microbiological sampling and consider antibiotics with antistaphylococcal activity.
Statistics from Altmetric.com
Wegener granulomatosis (WG) is a small vessel systemic vasculitis characterised by antineutrophil cytoplasmic antibodies (ANCAs) directed against proteinase-3 (PR-3). A role for infection in WG was first postulated by Frederick Wegener in 1936, but a more substantial argument was put forward in 1980, when a retrospective trial suggested that nearly 50% of relapses were provoked by infection.1 Nasal carriage of Staphylococcus aureus is increased in WG, and is associated with a higher relapse rate.2 How this relates to relapse and whether a similar process affects the lower respiratory tract is unknown.
It is unclear why patients with WG have increased nasal carriage of S aureus. A controlled cytokine response is essential for bacterial clearance and resolution of inflammation. However, experiments in acute respiratory distress syndrome have shown that elevated interleukin 6 (IL6), IL1 receptor antagonist (IL1ra) and IL1β levels in bronchoalveolar lavage fluid (BALF) are associated with a promotive growth environment for S aureus.3 4 These studies suggest that a proinflammatory environment may be permissive for S aureus growth, raising the possibility of a cause and effect relationship. Several reports have suggested the importance of cytokines in the inflammatory response seen in WG, but the clinical implications of these measurements have not been fully established.
Idiopathic pulmonary fibrosis (IPF) is a chronic interstitial lung disease associated with damage to the alveolar capillary barrier. A number of viruses have been implicated in IPF pathogenesis,5–7 but studies have not established whether bacteria in the lower airways are also present or play a proinflammatory role in patients with IPF. The current study was designed to establish the prevalence of lower airway pathogen growth in patients with WG or IPF and in normal controls, and then to determine any relationship with clinical or radiological findings. We went on to establish BALF levels of IL6, IL1ra and IL1β cytokines and lastly investigated whether WG BALF promotes S aureus growth in vitro.
METHODS
Patient recruitment
Thirty-three patients with WG meeting the classification criteria according to the Chapel Hill consensus statement were recruited.8 Patients were enrolled consecutively as they presented at University Hospital Birmingham from 2003 to 2008 with new or relapsing disease, and remission patients were consecutively recruited from clinic at routine appointment. Disease onset, relapse and remission definitions were defined according to European League against Rheumatism recommendations.9 Disease activity in WG was monitored using the Birmingham Vasculitis Activity Score (BVAS).10
Contraindications to enrolment for patients with WG were refractory hypoxia (arterial oxygen tension (PaO2)/fractional inspired oxyen (FiO2) ratio (P:F ratio) <300 on 40% oxygen), the need for ventilatory support (continuous positive airway pressure (CPAP), non-invase ventilation (NIV) or intermittent positive pressure ventilation (IPPV)) or continuous renal replacement therapy.
Idiopathic pulmonary fibrosis
We used IPF as a disease control which has not been associated with S aureus nasal carriage and as a comparator group who also receive immunosuppression in order to enable comment about the disease-specific nature of lower airway S aureus infection and for the influence of immunosuppression to be addressed. Twenty-two patients diagnosed with IPF according to current American Thoracic Society (ATS) criteria11 were recruited sequentially at first presentation to our interstitial lung disease clinic before immunosuppressive treatment.
No patients with IPF who had a history or clinical features to suggest active pulmonary infection within the last 4 weeks prior to bronchoscopy were included. Eight normal volunteers free from respiratory disease were recruited as controls. The study was conducted according to the Declaration of Helsinki. All patients gave informed consent and this study was approved by the local ethics committee (South Birmingham, UK, LREC ref 2003/166).
Imaging
Patients with WG and those with IPF underwent high resolution CT (HRCT) scanning. Scans were read blinded to conditions by a respiratory specialist (DRT) and a radiologist (PG), and assessed for features previously noted in a review of pulmonary findings in WG.12
Pulmonary function testing
Forced vital capacity (FVC) was measured using the Jaeger Compact system (Viasys Healthcare, Basingstoke, UK). Total lung diffusing capacity for carbon monoxide (TLCO) was measured by a single-breath technique (Jaeger Compact system; Viasys Healthcare). Results are expressed as the percentage of predicted values.
Bronchoalveolar lavage (BAL)
All patients underwent BAL according to national guidelines.13 To prevent nasal contamination, patients were intubated through the mouth. A nasal swab was performed for culture to look for matched nasal and lower airway bacteriology.
Repeat bronchoscopy
All patients with WG were invited to undergo a repeat bronchoscopy to establish whether there was evidence of persistent colonisation—7 patients with WG agreed to have repeat bronchoscopy entirely for research purposes after induction of remission; 4 others agreed to repeat BAL as they needed bronchoscopy for the assessment of disease relapse. Nine patients with IPF agreed to repeat bronchoscopy after at least 3 months treatment with prednisolone, azathioprine and latterly N-acetylcysteine.
Cytokine measurements
BALF cytokine levels were measured by ELISA (R&D Systems, Systems, UK) according to the manufacturer’s instructions.
Quantitative culture
Serial 10-fold dilutions (104–108) of the original BALF specimen were made in normal saline. An inoculum of each dilution was plated on chocolate and blood agar. Bacterial numbers at 24 and 48 h were estimated by two investigators, blinded to conditions, and expressed as colony-forming units (CFU)/ml BALF.
Culture experiments
To assess whether BALF is a permissive environment for S aureus growth, a laboratory S aureus (National Collection of Type Cultures, 6571, Oxford, UK) was incubated with BALF from 10 patients with WG, 10 patients with IPF and 6 normal controls. The S aureus was cultured in brain heart infusion (BHI). An inoculum of 10−5 bacteria per ml, determined using a haematocytometer, was added to 1 ml of BALF or 0.9% saline as a control in a 50:50 mix with 1 ml of BHI. Following an overnight incubation, 1:10 dilutions of the broth were made and dilutions of 10−4–10−7 were inoculated onto chocolate agar plates, in triplicate. The plates were read, after 24 h incubation at 37°C and 5% CO2, by two investigators blinded to the variable conditions. Preliminary experiments revealed that at the dilutions performed, the initial protein content did not effect S aureus growth (data not shown). BALF experiments were repeated following heat inactivation of the proteins in the BALF for 10 min at 80°C.
Statistics
Non-parametric data were assessed by Kolmogorov–Smirnoff test and are presented as median and interquartile range (IQR). Differences in pathogen growth patterns between cohorts and also between groups of patients with different WG activity were examined using Fisher exact test (FET). Cytokine analysis was performed using a Kruskal–Wallis test followed by a Dunn test to look at differences between cohorts and then look at differences within a disease group when a pathogen was present. Culture experiments had a Kruskal–Wallis test applied, and Dunn test was used to compare groups. A p value of ⩽0.05 was considered statistically significant. Statistics were performed using SPSS 15.
RESULTS
Demographics
At presentation, patients with WG were classified as acute (first ever presentation), relapse or remission based on their BVAS and clinical presentation. Clinical features of the individual activity groups, the 22 patients with IPF and 8 normal controls are described in table 1. Three of 11 (27%) acute patients underwent bronchoscopy before immunosuppression with steroids and cyclophosphamide, and 2/10 (20%) remission patients were on no medication (60% steroids, 30% azathioprine, 20% cyclophosphamide and 10% methotrexate). All relapse patients were on immunosuppressive medication at the time of bronchoscopy (83% steroids, 25% cyclophosphamide, 33% azathioprine, 16% each mycophenolate, rituximab and infliximab). Patients receiving cyclophosphamide had co-trimoxazole chemoprophylaxis. Pathogen growth was unrelated to individual immunosuppressive therapies in active or remission patients (data not shown). Of the 16 patients who were on co-trimoxazole chemoprophylaxis, 10 grew a pathogen of which 6 were S aureus. No patients with IPF had received treatment prior to the first bronchoscopy.
Microbiology of first bronchoscopy after enrolment
Pathogens were grown from 64% (21/33) of WG BALF compared with 36% (8/22) of IPF (FET, p = 0.058) and 0% (0/8) of normal controls (FET, p = 0.001). S aureus grew in the BALF of 40% (13/33) of all patients with WG compared with 0% (0/22) of patients with IPF (FET, p = 0.001). Other bacteria were identified equally in the two disease groups. No organisms were grown in the BALF from normal control subjects (table 2).
BALF pathogen growth in the different WG activity groups
Pathogens were more commonly grown in WG disease relapse (83% (10/12)) and remission (70% (7/10)) than at first acute presentation (36% (4/11)) although this did not reach statistical significance (FET, p = 0.076). S aureus was statistically more likely to be grown in the relapse (50% (6/12)) and remission group (60% (6/10)) than in the first acute presentation with WG (8.3% (1/12)) (FET, p = 0.031).
Five of 13 (38%) patients with WG who grew S aureus in the BALF had only mixed normal flora grown from their nasal swab. Two of 12 (17%) patients who grew S aureus from their nasal swab had a sterile BALF. The remaining samples were concordant, and all S aureus were methicillin sensitive.
Sequential BAL microbiology
There were no differences in the bacterial growth patterns from the first or second WG BALF. Three of 11 sequential patients with WG grew pathogens in both their BALF cultures, although the bacteria grown were different, giving no evidence of colonisation. Three patients grew a pathogen in the first culture but not in the second. Four patients grew a pathogen only in the second culture. A pathogen was more commonly grown on the second bronchoscopy although this was not statistically significant (FET, p = 0.076).
Five of nine patients with IPF who underwent sequential bronchoscopy had two sequential sterile cultures. Two patients grew pathogens only on the first occasion and two grew pathogens only on the repeat BAL. There was no increased likelihood of growing a pathogen on the second BAL culture (p = 0.376).
Pathogen growth related to clinical–radiological findings in WG
Most patients with WG (91%) had radiographic pulmonary abnormalities (table 1), with cavities more likely to occur in the disease relapse group (p = 0.031). The presence of a pathogen in WG BALF was not associated with bronchiectasis (FET, p = 0.761), cavities (p = 0.399), fibrosis (p = 0.724) or nodules (p = 0.555). There were no statistically significant differences in blood C-reactive protein (CRP) or white cell count in patients with WG and IPF who had evidence of bacterial infection (data not shown).
BALF cytokine levels and the relationship with pathogen growth
BALF levels of IL1α (Dunn test, p = 0.048), IL1β (p = 0.003), IL1ra (p<0.0001) and IL6 (p = 0.008) were elevated in patients with WG compared with normal controls. IL1ra (p<0.001) and IL6 (p = 0.009) levels were elevated in patients with IPF compared with controls. IL1α (p = 0.05) and IL1β (p = 0.001) levels were higher in patients with WG compared with IPF disease controls. Levels of IL1ra were elevated in patients with WG (p = 0.039) and IPF (p = 0.015) who grew a pathogen compared with those who did not. The other cytokine levels measured did not relate to the presence or absence of a pathogen (table 3).
Soluble factors within BALF promote S aureus growth
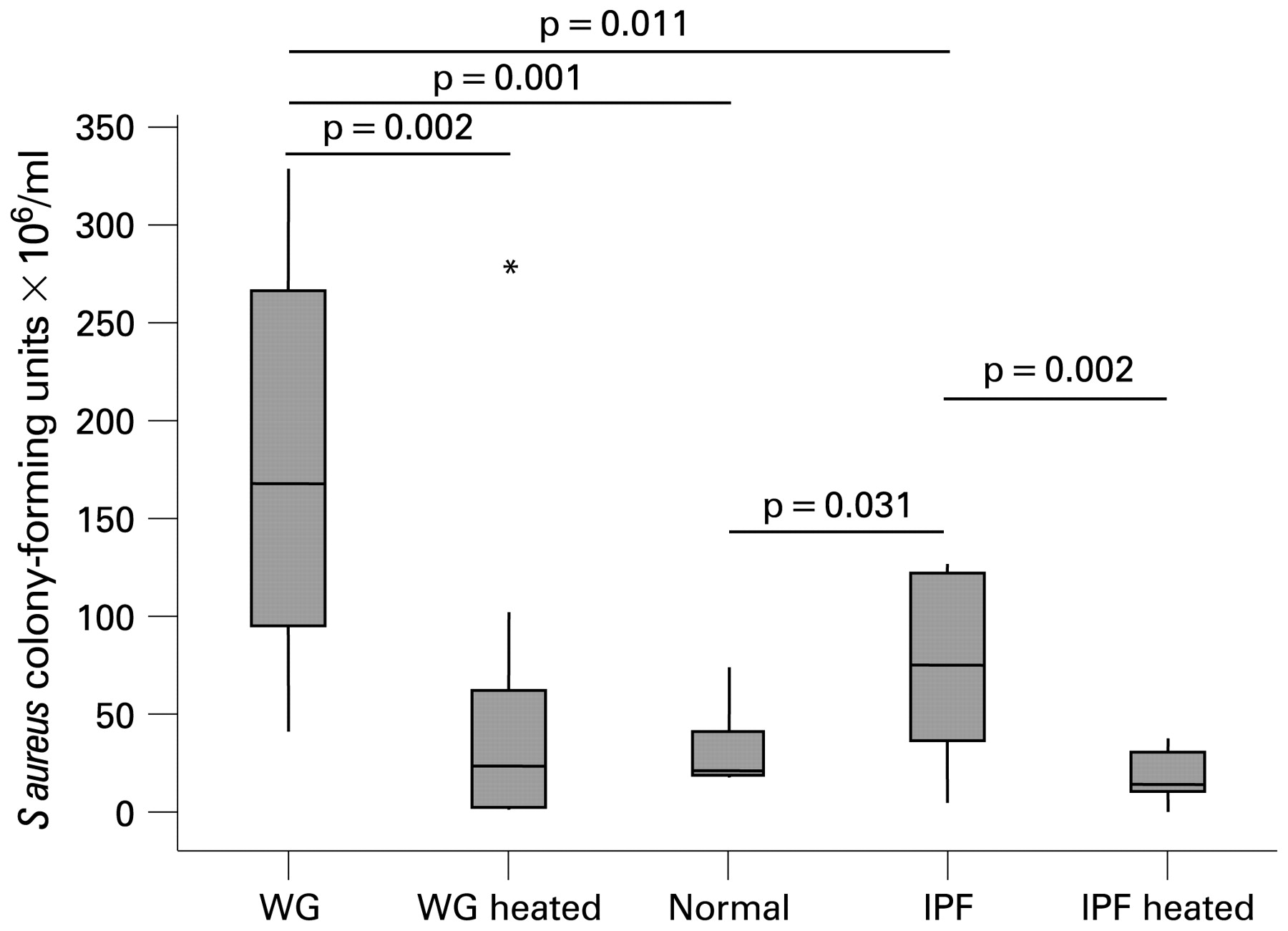
Incubations with BALF from patients with WG promoted statistically significantly more S aureus growth (Dunn test, 168.4 CFU/ml (IQR 95–268), p = 0.025) than BALF from patients with IPF [75.0 CFU/ml (IQR 37–122), p = 0.041) and normal controls (23 CFU/ml (IQR 19–42)). Heat inactivation resulted in a statistically significant reduction in S aureus growth with BALF from patients with WG (23.5 CFU/ml (IQR 3–63), (p = 0.0008) (fig 1).
{kind=link}
S aureus growth in culture with brochoalveolar lavage fluid (BALF). BALF or normal saline (50:50 mix) with brain heart infusion were incubated with an inoculum of 10−5 bacteria per ml. After 24 h of incubation, quantitative culture was performed to determine the number of S aureus colony-forming units. BALF experiments were repeated following heat inactivation of the proteins in the BALF for 10 min at 80°C. IPF, idiopathic pulmonary fibrosis; WG, Wegener granulomatosis.
DISCUSSION
This study has shown that pathogens were more commonly isolated from BALF of patients with WG and IPF than that from normal controls. S aureus was most frequently found in the WG remission and relapse groups rather than at disease presentation. Serial bronchoscopy suggests that pathogen presence in BALF was due to transient infection rather than persistent lower airway colonisation. There were no significant associations between pathogen growth and radiological findings, pulmonary function tests, immunosuppression or antibiotic treatment. Culture experiments revealed that WG BALF was a permissive environment for S aureus growth and that this effect was heat sensitive. Also, cytokines, previously reported to be promotive of S aureus growth in vitro, were elevated in WG.
Previous studies looking at nasal carriage of S aureus have suggested that persistent nasal S aureus carriage is associated with disease relapse in WG.2 We believe that ours is the first study to demonstrate that lower airway bacterial infection, especially with S aureus, is also common in patients with WG. Chronic lung damage is a recognised feature of the WG lung.14 and this may contribute to pathogen growth in conjunction with immunosuppressant therapy. Previous studies have shown that with progressive epithelial cell damage, adherence and internalisation of S aureus are increased.3 In WG this may be important since ANCA itself also induces IL1 and IL8 release from neutrophils,15 potentially amplifying local inflammatory tissue damage and thereby promoting S aureus growth.
The mechanisms by which S aureus may have a predilection for the lower airways of patients with WG especially in chronic disease are likely to be multifactorial—related to structural changes, functional immunodeficiency, defective host innate immunity or variability in the virulence of S aureus strains. There was a high incidence of bronchiectasis and cavities in the patients with WG relapse and remission, but this did not relate to the presence of a pathogen. Equally most but not all patients who had lower airway S aureus growth also had S aureus in the nose, suggesting a link with nasal carriage as part of the general respiratory tract response.
The lack of association with pulmonary features investigated in this study may reflect the relatively low numbers recruited in this trial, due to rarity of WG rather than a true lack of effect. However, if the lack of relationship is true it is likely that, in contrast to cavitating staphylococcal pneumonia,16 the underlying disease process rather than infection is driving the cavitation process, especially since several cases of cavitating disease had completely sterile BALF. There was also no clear effect of immunosuppression or chemoprophylaxis on bacterial growth, although the data were difficult to interpret because of the relatively small numbers in each group. Bacteria were isolated in active and remission patients despite the prophylactic co-trimoxazole prescribed, demonstrating that this dose was inadequate to control pathogen growth.
The microbiology pattern in WG was different between our three defined activity groups, with S. aureus more commonly isolated in disease relapse and remission patients rather than at acute presentation, suggesting that S aureus may have a role in disease relapse. The predilection of WG for S aureus infection appears to be disease related as these changes were not seen in patients with IPF who we used as a pulmonary disease control. Due to the intense inflammatory response associated with WG activity, we were unable to associate the presence of a pathogen with the intensity of the local cellular inflammatory response to confirm that this represented an infection rather than colonisation. However, BALF IL1Ra levels were increased in association with the presence of a pathogen in patients with both WG and IPF.
IL1Ra is an acute phase proteins and staphylococci are highly efficient in mediating the upregulation of IL1α, IL1β and IL1Ra.17 These data suggest that the presence of staphylococci may induce or relate to a local alveolar inflammation. In addition, since IL1Ra has previously been shown to be a trophic factor for S aureus,4 we performed relevant but simple BALF growth experiments in vitro. The observation that BALF from patients with WG stimulated growth of S aureus supports a role for a trophic interaction between the host inflammatory response and the bacteria within the lung. In this regard, WG BALF appears to have similar properties to that of acute respiratory distress syndrome.4
There are a number of potential mechanisms whereby S aureus infection might initiate relapse in WG; S aureus is able to stimulate directly the tumour necrosis factor α receptor,17 superantigen release,18 generation of immune complexes,19 expansion of memory effector T cells20 and may induce glucocorticoid resistance.21 Further recruitment, in a longitudinally studied cohort, will be required to assess the importance of our findings, and to address whether the prevalence of S aureus in the lower airway is associated with an increased risk of subsequent disease relapse, thus making intervention relevant.
This study has also demonstrated that a significant number of patients with IPF grow pathogenic bacteria from their BALF with a spectrum of pathogens different from WG. We specifically excluded any patient thought clinically to have had evidence of infection within the 4 weeks prior to bronchoscopy, and on their first bronchoscopy they were not immunosuppressed. To our knowledge, no study has previously looked at the issue of bacterial colonisation in IPF. Given the variable presence of cellular neutrophilic inflammation in patients with IPF, it is possible therefore that unrecognised airway colonisation is a determinant of this phenomenon. The clinical relevance of this observation warrants further evaluation especially in view of the recent publication of a pilot study demonstrating improved exercise tolerance and lung function with continuous co-trimoxazole usage in IPF patients.22
This study has limitations. First, during intubation, oral–pharyngeal contamination of the bronchoscope could have contributed to BALF pathogen growth. To counter this potential problem we used quantitative culture, a microbiological culture technique that has evolved as a sensitive and specific technique for the diagnosis of bacterial infection.23 Serial dilutions help to overcome contamination of the bronchoscope suction channel by oropharyngeal bacteria,24 and results were greater than would be expected from contamination alone. Secondly, we are unable to demonstrate in our BALF growth experiments that IL1Ra is directly responsible for the growth-promoting potential within the BALF as there is no effective inhibitor of IL1ra bioactivity. Finally, this was an observational study to ascertain the prevalence of pathogenic bacteria in the lungs of patients with WG, and our results need validation in another cohort of patients with WG.
In summary, this study has found a high incidence of pathogen carriage in the lower airways of patients with WG and IPF. The predilection for S aureus in WG is likely to be multifactorial but may relate to a dynamic relationship between alveolar inflammation and bacterial growth. Determining the role and mechanisms of lung S aureus carriage in disease and relapse may provide strategies for future treatments in WG. Physicians treating patients with acute or relapsing WG who wish to treat potential pulmonary infection should consider bronchoscopic microbiological sampling and prescribing antibiotics with antistaphylococcal activity.
Ethics approval: This study was approved by the local ethics committee (South Birmingham, UK, LREC ref 2003/166).
Acknowledgments
We would like to thank the staff and patients of the Birmingham vasculitis clinic and the University Hospital ILD clinic. We would like to thank Professor Caroline Savage and Dr Peter Guest (PG) for their help in this project, and Patti Bharadwa for her technical assistance.
REFERENCES
Supplementary materials
Web only appendix 64;8:692
Files in this Data Supplement:
Footnotes
Competing interests: None.
Funding: AR was supported by a Wellcome entry level fellowship. DRT is supported by a Wellcome Intermediate Fellowship.
▸ Additional methods are published online only at http://thorax.bmj.com/content/vol64/issue8