Article Text

Abstract
Background: Traffic-related pollution is associated with the onset of asthma in children. Its effect on adult-onset asthma is poorly investigated. The SAPALDIA cohort study was used to investigate associations between the 11-year change (1991–2002) in home outdoor traffic-related particulate matter up to 10 μm in diameter (TPM10) and the incidence of asthma.
Methods: Never-smokers without asthma at baseline aged 18–60 years in 1991 were eligible for inclusion in the study. Subjects reporting doctor-diagnosed asthma at follow-up were considered incident cases. TPM10 at baseline and follow-up was predicted and interpolated to subjects’ place of residence by dispersion models using emission and meteorological data. Cox proportional hazard models for time to asthma onset were adjusted (age, gender, baseline atopy, body mass index, bronchial reactivity, maternal allergies).
Results: Of 2725 never-smokers, 41 reported asthma onset in 2002. Home outdoor TPM10 concentrations improved during the interval (mean −0.6; range −9 to +7.2; IQR 0.6 μg/m3). The incidence of asthma was associated with a change in TPM10. The hazard ratio (1.30; 95% CI 1.05 to 1.61) per 1 μg/m3 change in TPM10 (IQR) was not sensitive to further adjustments (education, workplace exposure, passive smoking, parental asthma or allergies, random area effects, lung function or co-pollutants such as regional, secondary, total PM10 or proximity to busy roads).
Conclusion: The data suggest a role for traffic-related pollution in adult-onset asthma. Space, time and source-specific individual assignment of exposure to traffic-related pollution is a key strength of SAPALDIA. It may explain why findings were statistically significant despite the limited number of new cases. As traffic-related pollution prevails, the finding may be of substantial public health relevance.
Statistics from Altmetric.com
Currently prevailing levels of ambient air pollutants exacerbate asthma. Thus, asthma-related symptoms, emergency room visits and hospital admissions all increase—together with the need for asthma treatments—during periods with higher outdoor air pollution.1 2 A controversial question, though, is whether chronic exposure to ambient air pollution causes new onset of asthma. Earlier studies comparing the prevalence of asthma across communities with different levels of pollution did not support this notion.3 However, cross-community comparisons fail to characterise contrasts in exposure occurring within communities. The main reason for such small-scale contrasts is traffic. Related pollutants reach far higher concentrations on and along busy roads compared with locations 50–200 m away from traffic arteries.4 A recent review showed that living near traffic sources is associated with both onset and exacerbation of childhood asthma.2
The aetiology of asthma may well depend on the age of onset of the disease.5 However, adult-onset asthma has received less attention, and discussions centre mostly around smoking and occupational causes.6 7 Cohort studies indicate that onset of asthma among adults is not uncommon; for example, the Nurses Health Study reported approximately one new case of asthma per 1000 adults occurring every year.8 In the younger European Community Respiratory Health Survey (ECRHS), the incidence was 2.3 new cases per 1000 person-years.9 The first study suggesting an association between home outdoor nitrogen dioxide concentrations (NO2), used as marker for traffic-related pollution, and adult-onset asthma has only recently been published.10 The results did not reach statistical significance. Most recently, ECRHS and its Nordic companion study RHINE observed very similar associations between the incidence of asthma and modelled NO2 concentrations.11 12 ECHRS was based on a model with a rather limited spatial resolution (1×1 km) available for the follow-up only,13 14 while RHINE was based on air quality at baseline with no information about interval pollution.
We now use the Swiss Cohort Study on Air Pollution and Lung Diseases in Adults (SAPALDIA), a population-based cohort study initiated in 1991 and followed up 11 years later. Source-specific levels of pollution were spatially assigned to each participant and to the entire follow-up period. Recently, using this cohort, it was shown that an improvement in air quality is associated with an attenuated decline in lung function.15 The objective of this new analysis was to investigate whether individual-level change in exposure to local traffic-related pollutants correlated with adult-onset asthma. We focus the analysis on never-smokers. Tobacco smoke and ambient air pollution have hundreds of constituents in common, but concentrations in cigarette smoke are much higher so that, among smokers, exposure to these constituents is dominated by smoking, a well accepted cause of asthma.
METHODS
Study design and population
Selection of the study participants and methods of the cross-sectional study (SAPALDIA 1) and the follow-up study (SAPALDIA 2) have been described elsewhere.16 17 Random samples of adults (18–60 years) were recruited in 1990 using population registries in eight Swiss areas. Health examinations were conducted in 9651 adults (mean age 40.6 years; 51% women) in 1991 (SAPALDIA 1), with 8047 participants reassessed in 2002 (SAPALDIA 2). There were 5734 participants (71.3%) without asthma or spirometry-defined chronic obstructive pulmonary disease (COPD) at baseline, and with annual home outdoor concentrations of particulate matter up to 10 μm in diameter (PM10) available for both surveys (table 1 and fig 1). The 2725 never-smokers (47.6%) are the sample used in this analysis. Ethical approval was obtained from the Swiss Academy of Medical Sciences and the regional ethics committees and via written informed consent from all participants.

Distribution of the change in traffic-related individually assigned concentrations of particulate matter up to 10 μm in diameter (TPM10) by study area and for the total sample. The eight areas are ordered by the annual mean TPM10 at baseline. Negative changes indicate improvements in air quality. The reduction in TPM10 was on average larger in the most polluted areas (Basel and Geneva). Boxes show the median and quartiles (25th and 75th percentile) of the distribution.
Air pollution exposure assessment
The concentration of PM10 was used as a marker of air pollution. Details of the individual assignment of exposure are given in the online supplement. In brief, the 1990 and 2000 PolluMap dispersion model was used.18 Inputs were hourly meteorological and emission inventory data (industrial and commercial construction, household heating, agricultural and forestry activities, traffic emissions).18–20 Annual mean concentrations were derived from the hourly predictions for each 200×200 m grid cell and each source. All residential addresses were linked to the models. Values between 1990 and 2000 were interpolated using the historical trends of central site measurements.18 Differences in the annual traffic-related home outdoor PM10 concentrations between the two SAPALDIA studies were used to estimate the change in exposure (with a negative change indicating improvements in air quality). Henceforth, we use the term dTPM10 for the difference in traffic-related PM10 and TPM10 for traffic-related PM10. The use of the interval exposure, defined as the cumulated mean concentration of home outdoor levels of TPM10 across the follow-up period, will be discussed. While our hypothesis is based on TPM10, we discuss the use of changes in regional, secondary and total PM10 as part of the sensitivity analyses. Analyses using proximity buffers (20, 50, 75, 100, 150 m) as markers of exposure are discussed in the online supplement.
Definition of asthma and covariates
Asthma was defined as positive answers to both questions that are standard in many studies, namely “Have you ever had asthma?” and “Was this confirmed by a doctor?”.16 21 To define onset of doctor-diagnosed asthma, henceforth referred to as “asthma”, those with asthma or COPD (forced expiratory volume in 1 s/forced vital capacity (FEV1/FVC) <0.7) at baseline were excluded. Moreover, we excluded subjects without asthma at baseline who reported asthma at follow-up but indicated the year of onset to be prior to baseline. In sensitivity analyses we also ignored the latter restriction and, alternatively, made further restrictions at baseline, mainly requiring no asthma, no COPD and no bronchial hyperreactivity (BHR) based on the standard methacholine inhalation test.16 22
Detailed information about current, past and passive smoking, occupational exposure to dust and fumes and other risk factors was gathered through interview-administered questionnaires.21 Participants were classified as atopic if they developed a weal to one or more of the eight common inhalant allergens tested in the baseline skin prick test.16 21
Statistical analysis
Details are given in the online supplement. In brief, our main goal was to determine whether changes in traffic-related air quality were associated with new onset of asthma. We focus on the associations between the incidence of adult-onset asthma and dTPM10. Models using the highly correlated TPM10 at SAPALDIA 1 and SAPALDIA 2 as well as interval exposures are discussed in the online supplement.
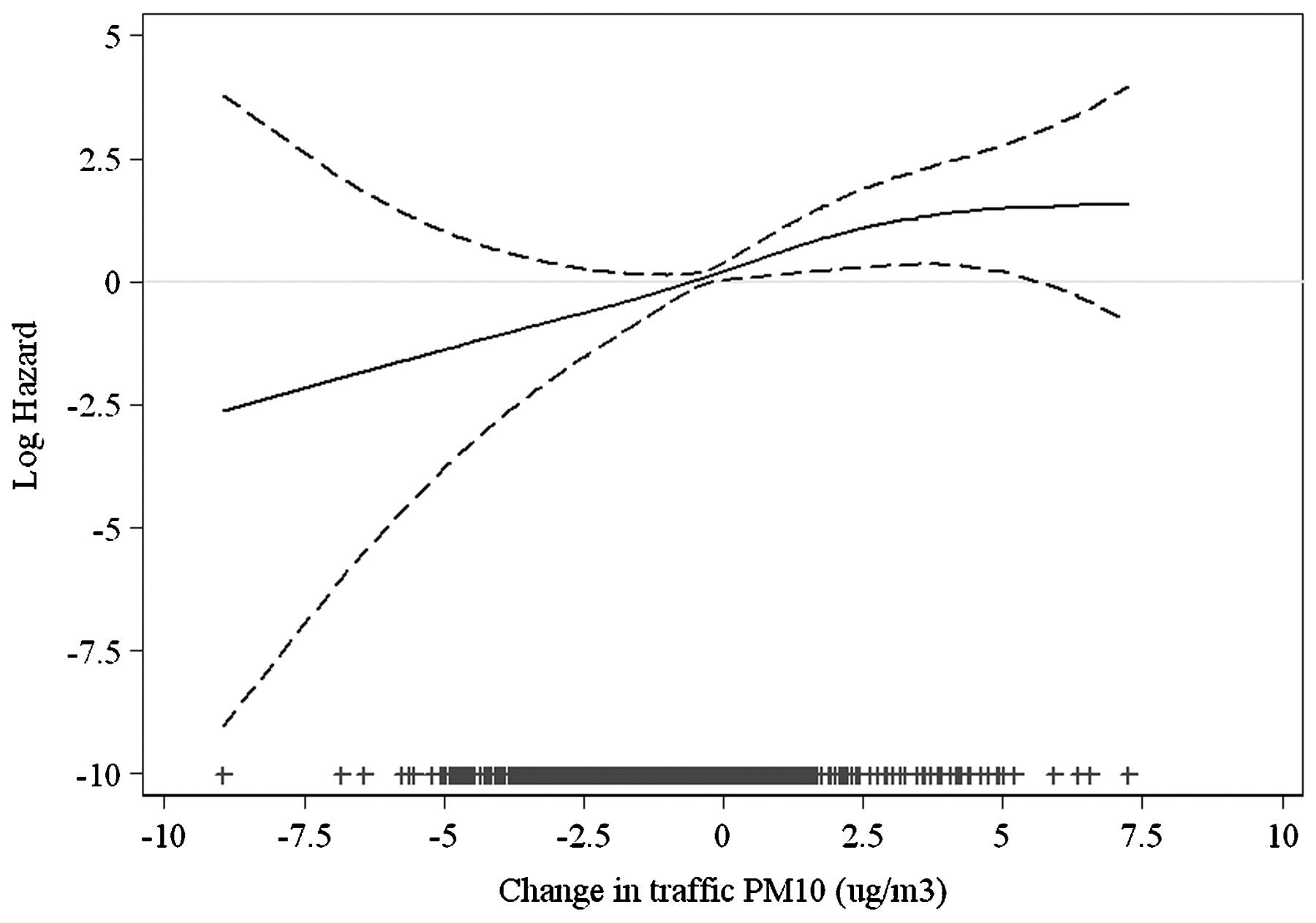
Analyses of incidence were based on Cox proportional hazard regression models. Time to onset of asthma was measured in years from SAPALDIA 1 to the reported age of first attack, or to SAPALDIA 2 among those without incident asthma (in which case outcomes were treated as censored). Covariates preselected on prior knowledge were considered as potential confounders if associated with incident asthma at a p value ⩽0.2. These variables were retained in the multivariate model if p values were <0.1 or if the coefficient of dTPM10 was modified by 10% or more upon their removal. For time-varying variables (body mass index (BMI), BHR, FEV1), we also considered the change between SAPALDIA 1 and 2 as potential confounders. Figure 2 was based on a non-parametric regression using Generalised Additive Models (GAM).

Association between change in traffic-related concentrations of particulate matter up to 10 μm in diameter (PM10) and adult-onset asthma (log hazard with 95% confidence interval) among SAPALDIA never-smokers. Generalised additive model adjusted for age, sex, atopy at baseline, body mass index at baseline, bronchial hyperreactivity at baseline, maternal allergies. The symbols (+) on the x-axis indicate observations.
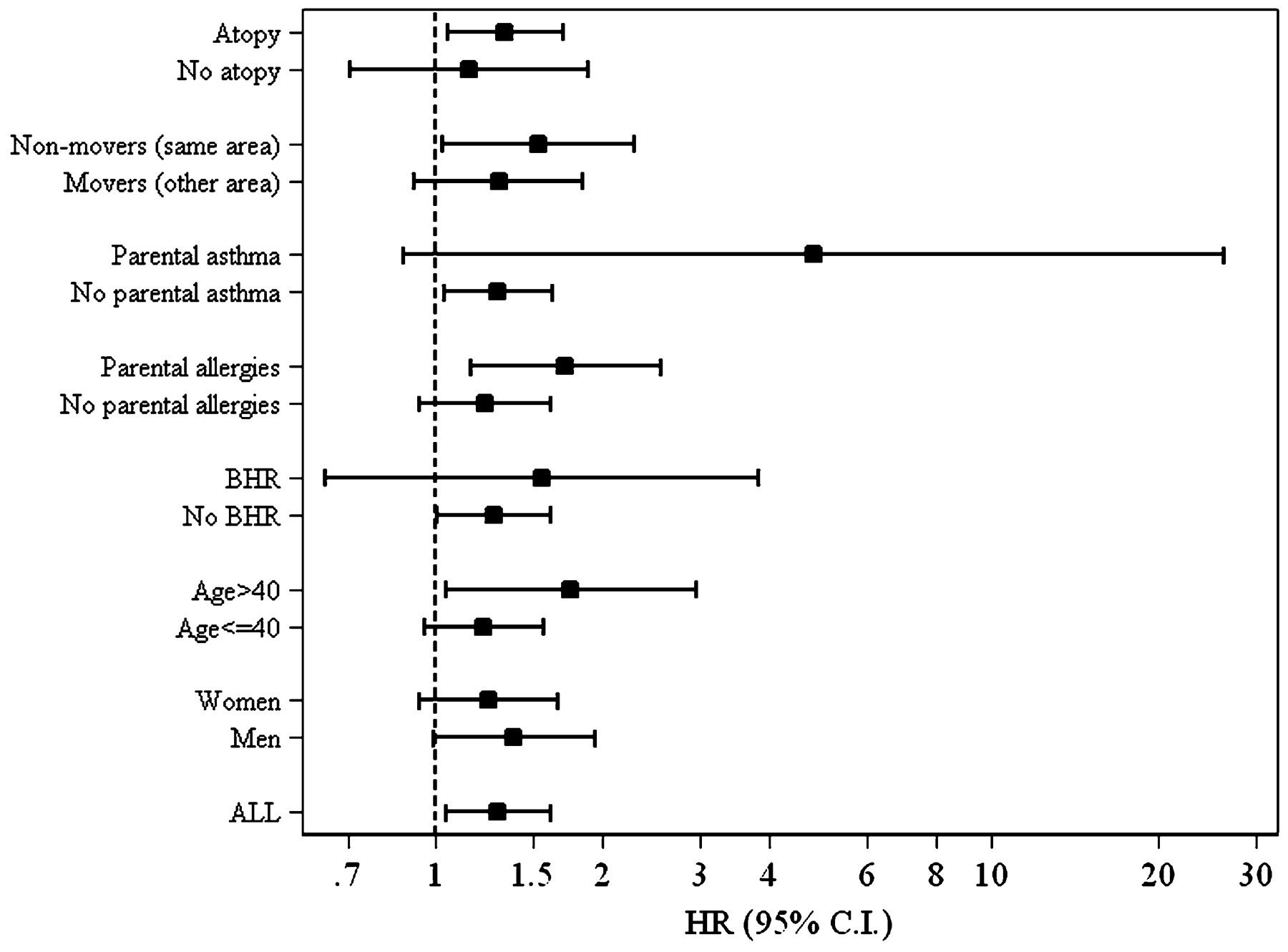
Sensitivity analyses consisted of both less and more parsimonious models, and analyses were also restricted to participants who always lived in the original SAPALDIA area. We also tested random effects of area lived in at baseline. The exploratory assessment of heterogeneity across predetermined subgroups (fig 3) has limited statistical power but may be of interest in comparison with future studies.
{kind=link}
{kind=link}
{kind=link}
Association between incidence of asthma and change in traffic-related concentrations of particulate matter up to 10 μm in diameter (PM10) among subgroups of never-smokers (models adjusted for age, sex, atopy at baseline, body mass index at baseline, bronchial hyperreactivity (BHR) at baseline, maternal allergies). Hazard ratios (HR) are presented per 1 μg/m3 difference in traffic-related PM10 with 95% confidence intervals (CI); p value for interaction for parental allergies = 0.088; all other interactions p>0.1.
Analyses were conducted with the statistical software Stata/SE 10.0. p Values of <0.05 were considered statistically significant. Proportional hazard assumptions were tested but never violated for the air pollution exposure terms.
RESULTS
Table 1 describes the main covariates of the 2725 never-smokers without asthma or COPD at baseline, stratified by incident asthma status at follow-up. A total of 41 subjects (1.5%) developed asthma during the 11 years of follow-up, corresponding to an incidence rate of 1.39 (95% CI 1.02 to 1.88) cases per 1000 person-years. New cases were on average younger and more likely to be atopic at baseline than non-asthmatic subjects. Baseline BHR was also more prevalent among incident cases. Non-participants are described in table S1 in the online supplement.
Traffic emissions were reduced by an average of 25% across all areas between 1990 and 2000.18 The area mean of the TPM10 ranged between 0.9 and 5.4 μg/m3 and between 0.8 and 3.1 μg/m3 in SAPALDIA 1 and 2, respectively, accounting for 6–16% of the total PM10 concentrations across the study areas. TPM10 was highly variable within areas. The within-area coefficient of variation (CV) ranged from 15% to 36% while the spatial variation of total PM10 within each area was small (range of CV 2–10%).
The distribution of area-specific dTPM10 is presented in fig 1. Table S4 in the online supplement provides the related data for movers and non-movers. Study areas are ordered by the area mean level of TPM10 at baseline. Changes were largest in the more polluted areas. The overall mean dTPM10 was −0.59 μg/m3, with a range from −8.95 to 7.24 and an interquartile range from −0.80 to −0.21 (table 1).
Table 2 shows the asthma incidence hazard ratios for a 1 μg/m3 change (approximately IQR) in TPM10 from several models. The hazard ratios were not sensitive to modelling assumptions. We observed a tendency toward stronger associations in multivariate models compared with the unadjusted model or the age- and sex-adjusted basic model (table 2).
Adjustment for area or the number of years lived at the baseline address did not affect the point estimates either. A stricter definition of “no asthma”, excluding subjects with hyperreactive airways at baseline, reduced the population to 1846 subjects. However, associations with dTPM10 remained similar (HR = 1.27; 95% CI 1.01 to 1.61 per μg/m3 dTPM10). As shown in table 3, adjustment for change in regional, secondary or total PM10 did not affect the point estimates for dTPM10 but inflated the confidence intervals yielding non-significant estimates. Hazard ratios of the 11-year change in these co-pollutants were instead very sensitive to adjustment by dTPM10. The null findings among smokers are shown in table S2 in the online supplement.
Residential proximity to busy roads was not associated with asthma. These results are discussed in the online supplement (including table S3).
Figure 2 shows the association between dTPM10 and the log of the hazard ratio based on the main model of table 2.
Area-specific estimates of dTPM10 reached statistical significance in only two communities (Wald and Payerne), with no indication of heterogeneity of associations across areas (p = 0.3). Hazard ratios among the subgroups explored for interaction are presented in fig 3. None of the apparent differences reached statistical significance for effect modification. Associations of dTPM10 with asthma onset appeared larger among those with parental allergies (p for heterogeneity = 0.088). In general, estimates were larger among non-movers with the main model HR reaching 1.53 (95% CI 1.02 to 2.28).
DISCUSSION
This study suggests that traffic-related air pollution has a role in the development of adult-onset asthma among never-smokers. These results are in line with numerous studies conducted in children. According to a recent review by Salam et al,2 evidence for a causal role of traffic-related air pollution on childhood asthma onset is strong and more recent studies further support the conclusions of Salam et al.23 The available individually assigned long-term characterisation of home outdoor pollution offered the unique opportunity to investigate how the change in traffic-related air quality affected adult-onset asthma. SAPALDIA has previously shown that improvement in air quality is associated with an attenuation in the decline of pulmonary function.15 Our novel results suggest that a decrease in air pollution is also paralleled by a reduced risk of developing asthma as an adult, or an increase in pollution correlates with a larger number of cases of adult-onset asthma.
The results need to be put in the context of several strengths and limitations. We first address challenges related to air pollution exposure assessment and then discuss the interpretation of the health outcome.
We believe that our ability of space, time and source-specific assignments of individual exposure is not only a strength but most likely a condition for successfully investigating the asthma-onset hypothesis. Our primary exposure term was the change in TPM10. Air quality improved during follow-up, but more so in the more polluted areas, leading to a negative correlation between baseline TPM10 and its change (dTPM10) (r = −0.76). Interval exposure correlated negatively with the change in TPM10 as well (r = −0.59). Thus, neither baseline exposure nor air quality at follow-up or interval exposure would capture the dynamic of a subject’s exposure history. The only adequate alternative approach to our analysis would be the use of the interval exposure with adjustment for baseline TPM10, which corresponds conceptually and mathematically to our use of the change in TPM10. While this strategy gave similar point estimates (table 3), the collinearity between baseline TPM10 and interval TPM10 greatly reduces precision in the estimation, underscoring the advantage of temporally resolved individual assignment of change in exposures.
The needs for accurate spatial and source-specific assignment of exposure are interrelated challenges for a successful investigation of the asthma hypothesis. Contrasts in subjects’ exposure to air pollutants originate to a large extent from spatial heterogeneity in air quality within cities. These contrasts are primarily driven by traffic-originated pollutants, which can easily increase 5–10 times in concentration along the traffic arteries while decreasing to “urban background” concentrations within 200 m of such roads.4 24 Thus, it is important to identify the exact residential location and to model traffic-specific markers of air pollution that reflect local spatial patterns. Our outdoor exposure model used source-specific emission inventories and estimated concentrations with a spatial resolution of 200×200 m.18 Models of some tail-pipe constituents may be improved with higher resolution. In this case, our estimates are likely to be biased to the null. Like other studies, we also ignored time at work or commuting. This misclassification may attenuate estimates, but we expect little bias as home outdoor remains the most important determinant of personal exposure to pollutants of outdoor origin.25
TPM10 ought to be considered a proxy for traffic-related primary pollutants rather than the culprit pollutant per se. Spatial distributions of other biologically relevant traffic-related toxicants (such as PM2.5, ultrafine particles, polycyclic aromatic hydrocarbons or redox active metals contained on fine PM) were not modelled separately and their correlation with TPM10 is not known. It may, however, be that what we label as “TPM10” captures in part also the spatial distribution in the exposure to ultrafine particles or other traffic-related constituents. Other markers of local traffic-related pollutants or PM compositions may result in different effect scales.
In contrast to several studies conducted in children, residential proximity to busy roads was not associated with asthma onset in our study. The limitation of such markers in a longitudinal study is discussed in the online supplement.
Point estimates were higher among subjects with better exposure assessment, namely those who never moved. Associations of asthma onset with PM10 from other sources were not only smaller but substantially decreased with adjustment for dTPM10 (eg, PM10 at baseline in table 3; other data not shown). In line with the findings in children, this observation further underscores the relevance of traffic-related versus urban background pollution in the development of asthma.
As emphasised by Eder et al, asthma is a syndrome rather than one disease, and various phenotypes of “asthma” may have different risk patterns.1 Our abilities to specify asthma phenotypes were limited as we relied on reported doctor-diagnosed asthma, as used in many epidemiological studies. This precludes a more detailed assessment of phenotypes and the clinical distinction between asthma and COPD. The latter were excluded from our baseline population and the analyses are restricted to non-smokers, so the impact of misclassified diagnoses may be rather marginal in this analysis.
However, a major related problem is the definition of “onset of asthma”. The distribution of time to onset varied substantially (see online table S5), and many reported onset of asthma prior to SAPALDIA 1 but did not report asthma at baseline. If we include those “loosely defined” new cases of asthma, associations remained positive but no longer statistically significant (see online table S6). Given the uncertainties related to the time of onset, the change in TPM10 was derived as the difference between SAPALDIA 1 and 2. The theoretically more appealing definition of the exposure window until asthma onset is discussed in the online supplement. These attenuated and non-significant findings must be interpreted with caution.
The identification of susceptible subgroups is of both public health and biological relevance. Given the limited number of new cases, we can only speculate about the meaning of the patterns shown in fig 3. Taken at face value, the results would indicate that those with an inherently higher baseline risk for asthma due to atopy, BHR or parental asthma are more strongly affected by traffic-originated pollution. However, none of the interactions was statistically significant, which may reflect random variation. Modig et al reported higher risks among atopic subjects.10
The onset of asthma among smokers—another group with an inherently higher incidence of asthma—was not associated with TPM10 (see table S2 in the online supplement). If similar combustion-related constituents and immunological mechanisms were involved in asthma onset due to both smoking and traffic-related pollution, the contribution of the latter exposure may be marginal among smokers, resulting in null findings for TPM10.
The study by Modig et al was the first to use a marker of local traffic-related pollution (namely NO2) to investigate the asthma-onset hypothesis in adults. While their findings are in line with our results, the correlations were not statistically significant in the Swedish case-control study (N = 2×203).10 It is also of note that traffic-related PM10 at SAPALDIA 2 was not associated with asthma onset. Since the Swedish study was based on cases and controls recruited from only one city (77 000 inhabitants), the subjects may all have experienced the same (unknown) temporal trends in exposure. One may therefore expect that “current exposure” adequately ranked people’s current, past as well as cumulative exposure. This assumption does not hold for SAPALDIA, which may explain the discrepancy between our results and those from the first Swedish study. In ECRHS the incidence of asthma also correlated significantly with home outdoor NO2 concentrations at follow-up, derived from an emission-based model.11 As in the first Swedish study, assignment of traffic-related exposure was done only for the address at follow-up as baseline air quality data were not available,13 so the positive results contrast with the null findings seen in our study if exposure at SAPALDIA 2 was used. It is not known whether air quality changes followed similar patterns for all participants across the 21 ECRHS centres, but follow-up in ECRHS was on average a few years shorter. The most recent Swedish study (2009) reported strikingly similar results to ECRHS, but was based on an NO2 dispersion model of high resolution (50×50 m).12 Our use of TPM10 precludes a quantitative comparison of risk estimates. Again, in contrast to our study, the Swedish study defines baseline exposure only. Spatial contrasts and changes may be less correlated in this study with shorter follow-up (8.3 years) and only three urban areas.
While the Seventh Day Adventist study (AHSMOG) reported an association between the incidence of asthma and ozone in men, as well as non-significant associations with particulate matter during the follow-up initiated in the late 1970s, local traffic-related pollution was not characterised.16 21 Time, location and population characteristics differ substantially between AHSMOG and SAPALDIA, limiting formal comparisons.
Biases are not a plausible explanation for our positive findings. Point estimates were neither sensitive to model specification nor to adjustment for fixed and time-varying determinants of asthma incidence nor study area (fixed or random effect). It appears unlikely that some uncontrolled factor was a strong enough risk for asthma onset and sufficiently correlated with dTPM10 to confound our estimates. To avoid multiple comparisons we a priori restricted the main analyses on one single marker of exposure—namely, traffic-related particles. Despite small numbers of new cases, associations were clearly statistically significant in several models and thus are unlikely to be explained by chance alone.
The consistency between our findings and observations made in children suggests that similar mechanisms may be involved both in early-life asthma and adult-onset asthma. Many of the traffic-originated pollutants have strong redox cycling capacity.26–28 This results in oxidative stress and both local as well as systemic inflammation, which are considered key pathways in the development of asthma.26 29 Experimental studies confirm an adverse role in IgE-mediated allergic responses which may play a role in asthma development among atopic subjects.30 Our data suggest the latter to be more strongly affected by traffic-related pollution. Respective findings in children are not consistent.2 This inconsistency may suggest different pathways being involved in childhood and adult-onset asthma among those exposed to traffic-related pollution. Future studies on adult-onset asthma may investigate the interaction of traffic-originated pollutants with genetic variants to elucidate the mechanisms involved in the observed associations.
In summary, the ability to assign space, time and source-specific exposure to traffic-related pollution to each individual is a strong feature of SAPALDIA. In line with numerous studies conducted in children, the findings suggest that traffic-related local pollutants contribute to asthma development and, even more importantly, that reductions in these pollutants decrease asthma risks as well. Given the widespread exposure to traffic pollution, we recommend studies to investigate the mechanisms of adult-onset asthma and identify the most susceptible subjects. Studies with a much larger sample size of asthma cases would greatly attenuate all the limitations faced in this study.
Acknowledgments
The SAPALDIA team (as of December 2008) including the authors was responsible for the study. Letters in parentheses are defined as follows: a, allergology; c, cardiology; cc, clinical chemistry; e, epidemiology; exp, exposure; g, genetic and molecular biology; m, meteorology; p, pneumology; s, statistics.
Study directorate: T Rochat (p), U Ackermann-Liebrich (e), J M Gaspoz (c), P Leuenberger (p), L J S Liu (exp), N M Probst Hensch (e/g), C Schindler (s).
Scientific team: J C Barthélémy (c), W Berger (g), R Bettschart (p), A Bircher (a), G Bolognini (p), O Brändli (p), M Brutsche (p), L Burdet (p), M Frey (p), M W Gerbase (p), D Gold (e/c/p), W Karrer (p), R Keller (p), B Knöpfli (p), N Künzli (e/exp), U Neu (exp), L Nicod (p), M Pons (p), E Russi (p), P Schmid-Grendelmeyer (a), J Schwartz (e), P Straehl (exp), J M Tschopp (p), A von Eckardstein (cc), J P Zellweger (p), E Zemp Stutz (e).
Scientific team at coordinating centres: P O Bridevaux (p), I Curjuric (e), J Dratva (e), D Felber Dietrich (c), A Gemperli (s), D Keidel (s), M Imboden (g).
REFERENCES
Supplementary materials
Web Only Data thx.2008.110031
Files in this Data Supplement:
Footnotes
Competing interests: None.
Funding: Swiss National Science Foundation (grants no 4026-28099, 3347CO-108796, 3247BO-104283, 3247BO-104288, 3247BO-104284, 32-65896.01, 32-59302.99, 32-52720.97, 32-4253.94); Federal Office for Forest, Environment and Landscape; Federal Office of Public Health; Federal Office of Roads and Transport; canton’s government of Aargau, Basel-Stadt, Basel-Land, Geneva, Luzern, Ticino, Zurich; Swiss Lung League; canton’s Lung League of Basel Stadt/Basel Landschaft, Geneva, Ticino and Zurich; Centre for Research in Environmental Epidemiology (CREAL), Barcelona, Spain; Catalan Institution for Research and Advanced Studies (ICREA), Barcelona, Spain. None of the funding sources had a role in the study design, data collection, analysis and interpretation of the data.
▸ Additional details are published online only at http://thorax.bmj.com/content/vol64/issue8
Ethics approval: Ethical approval was obtained from the Swiss Academy of Medical Sciences and the regional ethics committees and written informed consent was obtained from all participants.
Linked Articles
- Airwaves
- Editorial