Article Text

Statistics from Altmetric.com
The cost-effectiveness of prostanoids in pulmonary arterial hypertension (PAH) has recently been called into question by the National Institute for Health and Clinical Excellence (NICE),1 and the possibility exists that this treatment would not be recommended by this body. This would be the first time that a treatment already in routine clinical practice would be withdrawn as a result of NICE recommendations. Guidelines published by the UK, European and US authorities still advocate prostanoid use in certain patient groups.2–4 Of the disease-targeted therapy available for PAH, only epoprostenol has been shown to improve patient survival in the context of a randomised controlled trial.5
To assess the impact that withdrawal of intravenous epoprostenol in 1997 would have had, its use was retrospectively reviewed in a well-defined population of patients with PAH. This analysis includes eras before and after the licensing of oral agents in 2002.
All patients treated with intravenous epoprostenol by the Scottish Pulmonary Vascular Unit from 1997 to 2007 were identified. Case notes of this cohort were reviewed to determine (1) the reason for initiation of epoprostenol, (2) the outcome after 12 months of treatment as assessed by changes in conventional outcome measures and survival, and (3) the outcome in those patients whose treatment with epoprostenol commenced after licensing of oral disease-targeted therapy in 2002. Patient improvement was defined as either an improvement in functional class or an improvement in the 6-minute walk distance (6MWD) 3 months after initiation of treatment. Patients were then divided into the following groups: (1) improvement and survived >12 months; (2) stabilised (ie, no improvement but survived >12 months); (3) died within 12 months; or (4) intolerant of treatment. Where available, N-terminal proB type natriuretic peptide (NT-proBNP) and quality of life (QOL) measurements were also analysed.
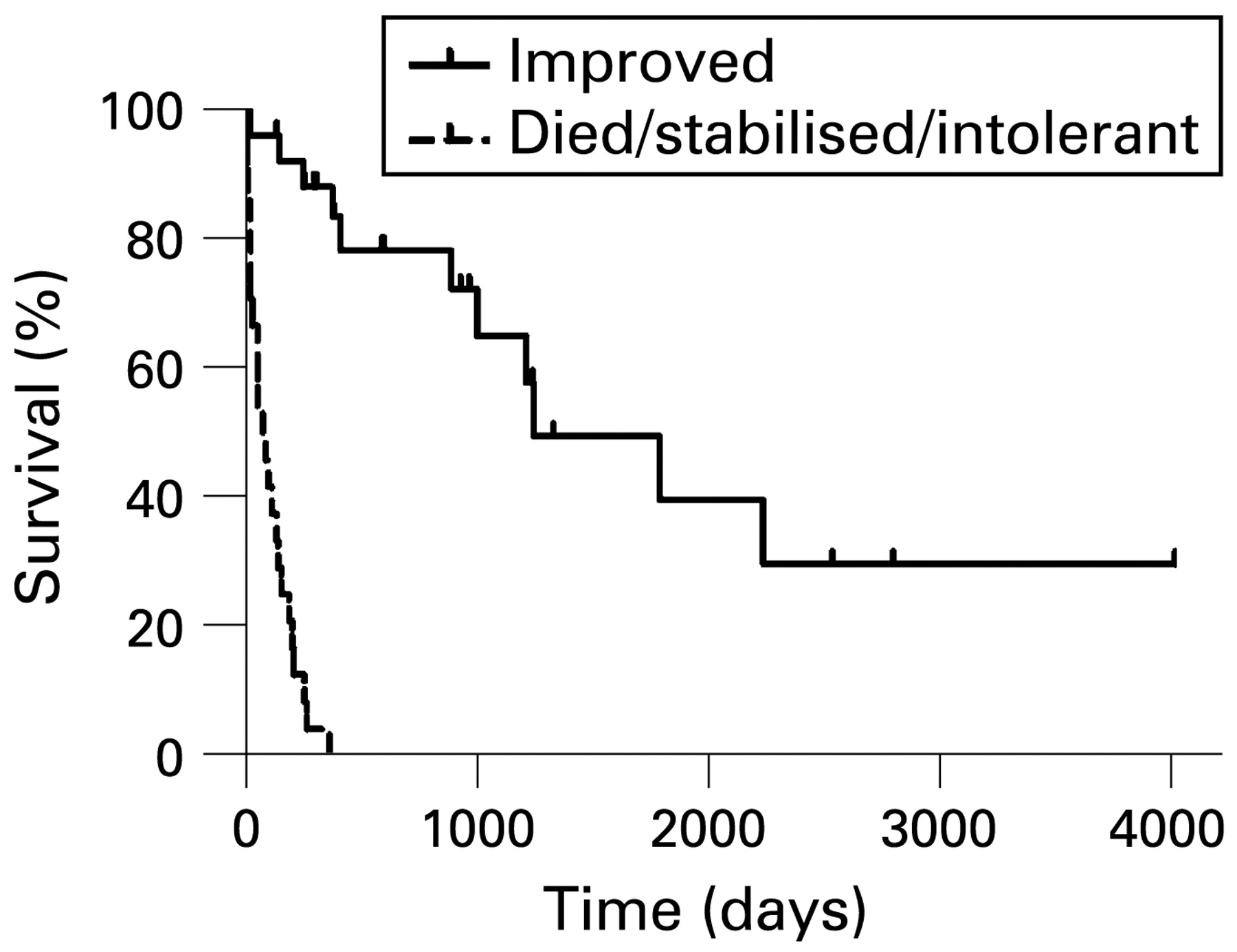
Fifty (20%) of 252 patients with PAH were identified as having received epoprostenol during this period. Of this group, 30 (60%) either improved or stabilised for >12 months. Data on the improvements in 6MWD, QOL, functional class and NT-proBNP are included in the online supplement. Figure 1 shows the survival advantage for patients whose functional class or 6MWD improved with intravenous epoprostenol.

{kind=link}
Survival from time of initiation of epoprostenol in the entire cohort.
For the subset of patients following the introduction of oral disease-targeted therapy agents in 2002, 30 (15%) out of 199 required epoprostenol; 17 (57%) improved, 9 (30%) died before 12 months, 3 (10%) stabilised and 1 was intolerant of the agent. Included in this group were 12 patients who required epoprostenol after deterioration on oral agents; 7 improved, 3 died, 1 stabilised and 1 was intolerant. Data on the improvements in 6MWD, QOL, functional class and NT-proBNP in this group of patients are also shown in the online supplement.
Point prevalence data (see online supplement) still demonstrated an ongoing need for epoprostenol in the current era of oral agents.
This study suggests that, had intravenous epoprostenol not been available over the last decade as a treatment for PAH, a significant number of patients in Scotland would have been denied an effective treatment. Where data are available in the subjects, there were improvements in all outcome measures (functional class, 6MWD, NTproBNP, QOL). More compelling, however, is the survival analysis of the entire cohort which demonstrated a large survival advantage in those patients in whom functional class or 6MWD improved. This situation remains true in the era of oral treatments. This should have implications for future NICE review of the role of epoprostenol in PAH.
Supplementary materials
Web only appendix 64:7;642
Files in this Data Supplement:
{kind=link}
{kind=link}
{kind=link}
Footnotes
▸ Additional data are published online only at http://thorax.bmj.com/content/vol64/issue7
Funding: National Services Division.
Competing interests: None.