Article Text

Abstract
Background: Influenza and pneumococcal vaccination are recommended in patients with chronic obstructive pulmonary disease (COPD). A recent study from Tayside found a reduced risk of all-cause mortality with vaccination in patients with COPD. The Health Improvement Network (THIN) database was used to test this hypothesis in a different data source.
Methods: The THIN database was searched for patients with COPD. Vaccination status against Pneumococcus and the annual influenza vaccination status were determined. Mortality rates were calculated in the periods December to March and April to November. Relative risks for the effect of vaccination on all-cause mortality were estimated by Poisson regression, adjusting for age, sex, year and serious co-morbidities.
Results: 177 120 patients with COPD (mean age 65 years) were identified, with a mean follow-up of 6.8 years between 1988 and 2006. Vaccination rates against influenza rose from <30% before 1995 to >70% in 2005 in patients aged 60 years or more. The cumulative vaccination rate against pneumonia rose from almost zero to 70% in patients aged 70 years or more over the same period. For all-cause mortality the adjusted relative risks associated with influenza vaccination were 0.59 (95% CI 0.57 to 0.61) during the influenza season and 0.97 (95% CI 0.94 to 1.00) outside the season in patients not vaccinated against pneumonia, and 0.30 (95% CI 0.28 to 0.32) and 0.98 (95% CI 0.96 to 1.11), respectively, in patients vaccinated against pneumonia. The relative risk associated with pneumococcal vaccination was >1 at all times of the year.
Conclusions: Influenza but not pneumococcal vaccination was associated with a reduced risk of all-cause mortality in COPD.
Statistics from Altmetric.com
Chronic obstructive pulmonary disease (COPD) is the fourth leading cause of death worldwide resulting in more than 2.7 million deaths in 2000.1 COPD exacerbations are a common cause of mortality and morbidity and prevention is an important strategy as effective treatment of exacerbations is still inadequate. Vaccinations against influenza and pneumococcus are recommended in NICE guidelines for COPD.2
A recent study used data from the Tayside Respiratory Disease Information System (TARDIS) to develop a score predicting mortality in patients with COPD. This showed a reduced risk of all-cause mortality in patients vaccinated against influenza and Pneumococcus.3 As testing for the effect of vaccination was not the primary objective of that study, we tested the hypothesis using a different source of data, The Health Improvement Network (THIN). THIN is a medical research database of over 4.25 million anonymised patient records from information entered by more than 300 general practices throughout the UK that have joined the scheme. An audit of this database confirmed a high level of completeness of recording of clinical information.4
Published randomised controlled trials have not demonstrated a mortality benefit for these interventions,5–9 and observational studies have an important role in addressing this gap in knowledge. Many previous published studies of the effectiveness of influenza vaccine have possible biases as they include only one or a few influenza seasons, thus not controlling for the variability from season to season.10 Such studies attempt to control for confounding factors by adjusting for co-morbidities, as shown by Jackson et al;11 such adjustment is unlikely to remove all bias. This may be due to the presence of functional limitations in the group defined as free of co-morbidity by diagnosis code criteria. Such uncontrolled functional limitations appear to be important confounders of the association of vaccination and risk of death.12
In this study we ascertained the effectiveness of influenza and pneumococcal vaccination in a community population of patients with COPD over an 18-year period in order to obtain a long-term view of the effectiveness of vaccination.
METHODS
Study population and study cohort
The study population consisted of all patients over 40 years of age permanently registered with practices contributing to the THIN database with a diagnosis coded as COPD, chronic obstructive airway disease (COAD), chronic bronchitis or emphysema. Patients with any history of lung fibrosis, sarcoidosis, lung cancer or lung surgery were excluded. The study period was from 1988 to 2006.
Outcomes
We defined three outcomes: all deaths; the subset of deaths where a respiratory code was recorded on the day of death or was cited as the cause of death; and the subset of deaths where a respiratory code was cited as the cause of death (see online Appendix 1 for Read codes).
Bias and confounding factors
Age, gender and co-morbidity were used as covariates to attempt to adjust for any confounding bias that could have affected the likelihood of vaccination. To identify serious co-morbidities that were likely to be risk factors for death, we used the list of serious diseases included in the Charlson co-morbidity score.13 We defined a flag variable for each of these disease groups for each patient in each year. We did not calculate the Charlson score, but used the individual indicator variables in our statistical models.
An apparent vaccination effect outside the influenza season would probably be due to bias associated with unidentified risk factors. A difference between the apparent vaccination effects in the influenza season and in the rest of the year in the same patient population may be a better measure of any benefit provided by vaccination. We therefore estimated the ratio of relative risks in the influenza season and in the rest of the year (ie, the interaction between influenza vaccination and season).
Statistical methods
A retrospective analysis was performed of the cohorts of patients who were vaccinated against influenza, pneumonia, both or neither between 1988 and 2006. The study period for each patient was divided into consecutive 1-year periods starting on 1 December each year.
Patients were regarded as immunised against pneumonia in a given year if they had been vaccinated at any time before 1 December of that year. Patients were regarded as immunised against influenza in a given year if they received a vaccination at any time after 1 August of that year and before 1 August of the next year. We assumed that immunity to influenza was acquired 30 days after vaccination. In patient-years where influenza vaccination occurred, the time before vaccination is “immortal” time (ie, death could not have occurred in this period). We discarded time before the date that immunity was acquired (ie, the immortal period plus the first 30 days after vaccination).
We identified deaths from any cause in December to March and April to November for unvaccinated patient-years, and in the periods of immunity between these dates for vaccinated patient-years. Relative risks for the effect of vaccination on all-cause mortality were estimated for each period by Poisson regression, using time at risk as an offset variable and adjusting for age, sex, year and 15 co-morbidities. We also included a factor to indicate whether or not the influenza vaccine used each year included all the strains of virus in circulation in that season.
Preliminary analyses suggested a strong interaction between pneumonia and influenza vaccination, so we estimated the interaction between influenza vaccination and season separately in patients who had and had not been vaccinated against pneumonia.
RESULTS
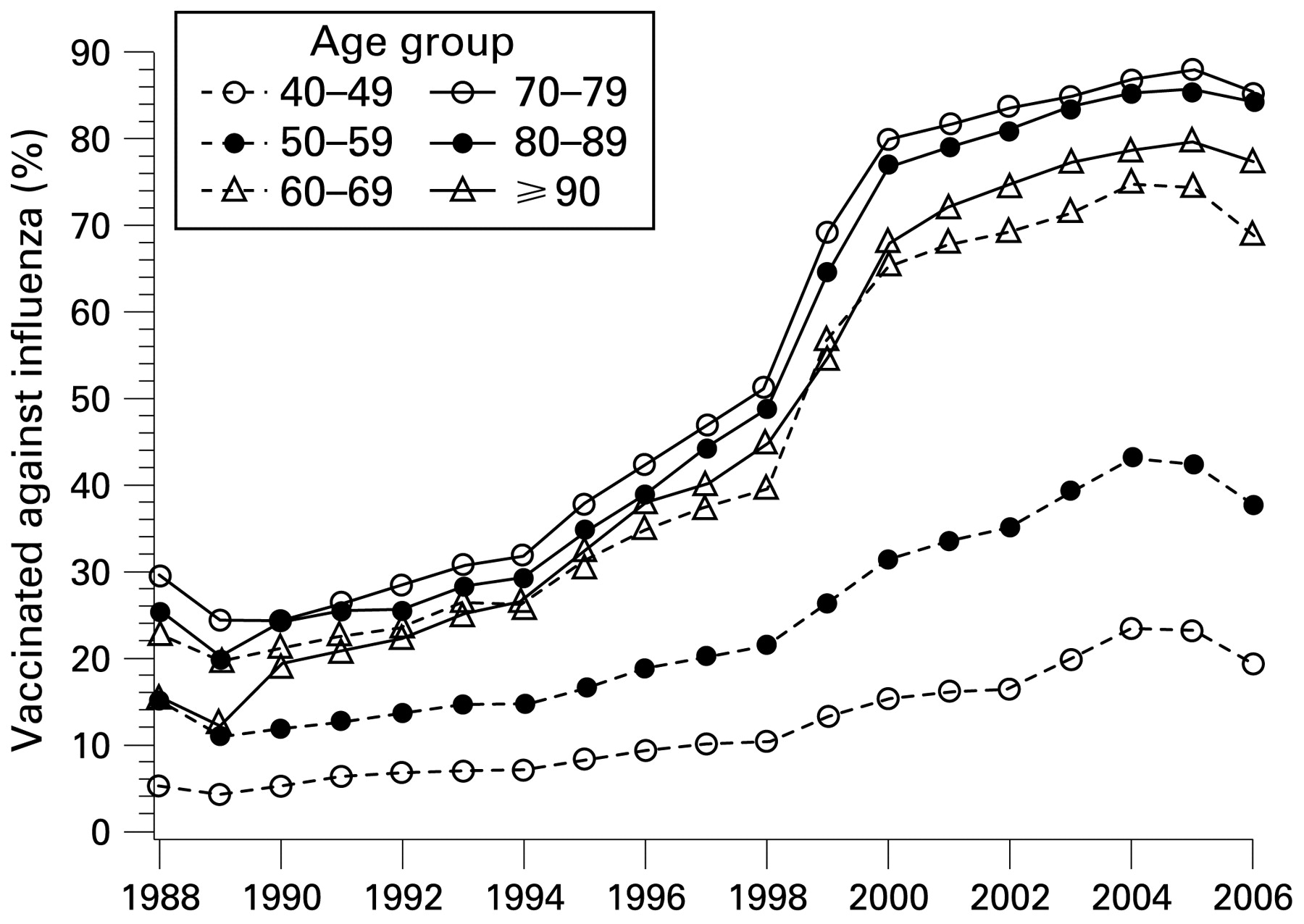
A total of 177 120 patients with COPD with an average of 6.8 years follow-up between 1988 and 2006 were identified. Their mean age at the start of each influenza season was about 65 years. Figure 1 shows that the rate of vaccination against influenza among patients aged ⩾60 years rose from 20–30% in the early 1990s to at least 70% (and 80% in patients aged ⩾80 years) after 2000. Figure 2 shows that the cumulative rates of vaccination against pneumonia rose from almost zero in 1993 to at least 75% in patients aged ⩾70 years in 2006.

Trends in vaccination rates against influenza in patients aged >40 years with chronic obstructive pulmonary disease.

{kind=link}
{kind=link}
Trends in vaccination rates against pneumonia in patients aged >40 years with chronic obstructive pulmonary disease.
Table 1 shows sex and age distributions and the co-morbidities of vaccinated and unvaccinated patients in the 2006/7 influenza season. Vaccinated patients, particularly those who received both vaccinations, were older than unvaccinated patients. Most of the co-morbidities were substantially more prevalent in patients who received either vaccination or both.
Table 2 shows the unadjusted all-cause mortality rates and death rates associated with respiratory events for the periods December to March and April to November, pooled over the whole study period. The all-cause mortality rate was 52 deaths per thousand patient-years (ptpy) during the influenza seasons, and 46 deaths ptpy at other times. The unadjusted death rate was substantially higher among patients vaccinated against pneumonia than those who were not vaccinated (64 vs 48 deaths ptpy in the influenza season, 68 vs 40 deaths ptpy at other times). In April to November it was also higher in patients who had been vaccinated against influenza in the previous influenza season than in those who had not (63 vs 35 deaths ptpy), although the rates had been similar during the influenza season (53 vs 51 deaths ptpy).
The annual all-cause mortality rate varied little over the study period. However, death rates associated with a respiratory event increased substantially over the study period. This may be due to improvements made by GPs in their recording of cause of death, and a year effect was therefore included in all the statistical models to account for this trend.
Table 3 shows the relative risks of death from any cause for the other risk factors included in the models. Men were at higher risk than women and there was a strong trend with age. The relative risk (RR) of death in December to March vs April to November was 1.37 (95% CI 1.33 to 1.40). Furthermore, in years when the influenza vaccine did not include all strains of the virus circulating during that season, mortality rates were also higher (RR 1.19 (95% CI 1.13 to 1.25)). All of the co-morbidities identified, except diabetes with chronic disorders, were also significant risk factors for death.
Table 4 shows the adjusted relative risks for the effect of vaccination against influenza and pneumonia. In December to March the RR associated with vaccination against influenza was 0.59 (95% CI 0.57 to 0.61) in patients not vaccinated against pneumonia, but vaccination against influenza provided no benefit to the same patients in the following April to November (RR 0.98 (95% CI 0.95 to 1.01)). Similar RRs were obtained from the two subsets of deaths associated with respiratory events. An RR close to 1 for influenza vaccination outside the influenza season suggests that confounding between vaccination and the major risk factors for death have been accounted for in the analysis, and that the RR estimated for the influenza season may be a good guide to the benefits of vaccination.
Patients vaccinated against pneumonia but not against influenza had a higher risk of death in both seasons (RR 1.68 (95% CI 1.58 to 1.78) in December to March, RR 1.28 (95% CI 1.20 to 1.36) in April to November). This pattern, too, was repeated from the two subsets of deaths associated with respiratory events. RRs greater than 1 for vaccination against pneumonia suggest that some confounding between vaccination and risk factors for death remains unidentified.
RRs for patients immunised against both pneumonia and influenza were similar to those for patients vaccinated against influenza only.
Table 5 shows the results of subgroup analyses for patients who have and have not been vaccinated against pneumonia. They confirm that in both populations there is a strong interaction between season and the apparent effect of vaccination against influenza. In patients not vaccinated against pneumonia, the ratio of RRs for December to March vs April to November is 0.60 (95% CI 0.58 to 0.63) for all-cause mortality, very close to the apparent effect observed in December to March since the RR in April to November is close to 1.
In patients who had been vaccinated against pneumonia, those who were also vaccinated against influenza had a lower risk of death even outside the influenza season (RR 0.64 (95% CI 0.60 to 0.68)). However, the RR associated with influenza vaccination in these patients during the influenza season was lower still (0.30 (95% CI 0.28 to 0.32)) and the ratio of RRs (0.47 (95% CI 0.43 to 0.51)) suggests a substantial benefit from vaccination in these patients too.
DISCUSSION
Our study is the largest study of patients with COPD and provides data that supports vaccination in this patient group. Unlike a recent Cochrane review which showed no effect of influenza vaccination on mortality,14 our study suggests that influenza vaccinations are effective in decreasing all-cause mortality. NICE guidelines advise vaccination of patients with chronic obstructive pulmonary disease against influenza and Pneumococcus. Rates of influenza vaccination in patients with chronic obstructive pulmonary disease aged >60 years have increased from <30% before 1995 to >70% since 2000. Immunisation against pneumococcal disease has risen from almost zero in 1995 to >70% in patients aged ⩾70 years.
Previous studies of influenza vaccination have shown significant protection against all-cause mortality in a cohort of elderly patients15 and also in elderly patients with chronic lung disease.16 Our study is the first in a community-based population of patients with COPD of all ages.
The strengths of this study are that data were collected in routine care from an unselected community population of patients with COPD throughout the UK. This increases the likelihood that the results will be applicable to other COPD populations. We adjusted for a number of possible confounders and measured the effect of vaccination during the influenza season relative to that among the same patients in the summer in an attempt to minimise the effects of unobserved confounding factors. Unlike most studies which often cover only one season, our study covered several influenza seasons which is especially important as the antibody levels may fall to non-protective levels within a year of vaccination resulting in lack of spillover protection from year to year.17
We used the THIN database, which is a relatively new primary care medical records database in the UK. It comprises prospectively collected data from September 2002. Some practices had electronic medical records as early as 1987 and these data were also included in THIN. The validity of the THIN database was confirmed in a recent study replicating well-established associations and by comparing results with other primary care databases.18
Limitations of the study include possible misclassification since COPD is often misdiagnosed or miscoded in electronic medical records. COPD is a diagnosis based on spirometry, but these results are not always available from routine records. The study population is therefore likely to include patients with a false positive diagnosis of COPD. However, such misclassification of disease is likely to bias the study towards the null unless vaccination has a similar effect size in subjects without COPD. It is also possible that vaccination status misclassification may have occurred; however, this seems less likely. There may also be a channelling bias in this study (ie, patients at most risk of hospitalisation or death may be more likely to be vaccinated). If this had occurred, then vaccination would be expected to be associated with a worse outcome and an observed benefit would be more impressive of efficacy.
We attempted to adjust for this using confounding factors where recorded, but some bias due to unrecorded factors may remain. It may also be true that patients with good health behaviour may seek vaccination more frequently than those with poor heath behaviour. This healthy user effect may partly explain the present results. Also, the completeness of cause of death records appeared to vary substantially over the study period.
It would have been ideal to adjust for years with an influenza epidemic as the protective effect would be expected to be greater but we did not have this information. However, we were able to identify years in which the influenza vaccine included all the strains of virus that were in circulation during the subsequent season, and mortality rates were lower in these years. Pneumococcal vaccination is thought to offer protection against bacterial septicaemia,19 but these data were not available.
CONCLUSION
Influenza vaccination was associated with a reduced risk of all-cause mortality in patients with COPD but pneumococcal vaccination was not, possibly due to the effect of unidentified confounding factors.
REFERENCES
Supplementary materials
Web only appendix 64;7:567-72
Files in this Data Supplement:
Footnotes
▸ Appendix 1 is published online only at http://thorax.bmj.com/content/vol64/issue7
Competing interests: SS has received funding from GlaxoSmithKline, AstraZeneca and Boehringer Ingelheim to attend meetings. He has been a consultant to GlaxoSmithKline. SM has been a paid consultant to Pfizer Inc. JHW has no conflicts of interest. TMM has been paid speaker’s fees or travel costs by Pfizer, Novartis, Servier and Takeda. His department has had research grants from GlaxoSmithKline, Aventis, Novartis, AstraZeneca, BMS, Boehringer Ingelheim, Pfizer and Novartis. TMM has been paid consulting fees by Pfizer, Novartis, Kaiser Permanante, Quintiles, Takeda, AstraZeneca, Sankyo Recordati and Speedel.