Article Text

Abstract
Rationale: There is increasing interest regarding asthma heterogeneity in relation to inflammatory patterns.
Objectives: To assess phenotypic characteristics, in particular clinical presentation of the disease, in 381 well-characterised adults with asthma from the French Epidemiological study on the Genetics and Environment of Asthma (EGEA) according to their blood inflammatory pattern.
Methods: Four blood inflammatory patterns were defined according to eosinophil (EOS) and neutrophil (NEU) count cut-off points. Samples with ⩾250 EOS/mm3 were classified as EOShi and those with ⩾5000 NEU/mm3 as NEUhi. Clinical characteristics include typical asthma and chronic obstructive pulmonary disease (COPD)-like symptoms, as well as composite quantitative scores addressing the activity of the disease.
Results: A substantial number of those with asthma (56.2%) had the EOSlo pattern (<250 EOS/mm3). Patients with asthma who had the EOShi pattern had higher immunoglobulin E (IgE), a lower forced expiratory volume in 1 s (FEV1) and presented a more active asthma than those with the EOSlo pattern. Among those with the EOSlo pattern, neutrophil inflammation (NEUhi) was related to a less frequent positive skin prick test response (OR 0.44, 95% CI 0.20 to 0.96). Among those with the EOShi pattern, neutrophil inflammation did not explain current asthma or asthma activity, and was significantly related to nocturnal symptoms (OR 5.21, 95% CI 1.44 to 18.8) independently of age, sex, smoking and inhaled corticosteroid treatment. In non-smokers with asthma, COPD-like symptoms, in particular chronic phlegm, were more frequent in those with neutrophil inflammation, independent of eosinophil inflammation (OR 2.35, 95% CI 1.08 to 5.10).
Conclusions: Besides eosinophilia, neutrophil inflammation assessed in the blood is related to specific characteristics of asthma. Considering simultaneously neutrophilic and eosinophilic inflammation may contribute to help to disentangle this complex disease.
Statistics from Altmetric.com
There is increasing interest in asthma heterogeneity in relation to inflammatory patterns. Reviews have focused on non-allergic and on non-eosinophilic asthma, showing that only 50% of all asthma cases were attributable to eosinophilic airway inflammation.1 Concomitantly, the negative results of anti-interleukin 5 (IL5) treatment in asthma also increased interest in patients with asthma without eosinophilia.2 Recent observations from the Epidemiological study on the Genetics and Environment of Asthma (EGEA) on the inter-relationships of the three classical allergy markers used in epidemiology, the skin prick test response, total immunoglobulin E (IgE) and eosinophils, showed that eosinophils were significantly related to IgE and the skin prick test response in children only,3 increasing the likelihood that they are key to disentangling the phenotypic heterogeneity of asthma. In that context, Wenzel4 suggested considering “inflammatory phenotypes”—that is, eosinophil and neutrophil inflammation—in adult persistent asthmas.
Few epidemiological reports have simultaneously considered associations of blood eosinophil and neutrophil inflammation with respiratory symptoms, including bronchitis, chronic phlegm, bronchial hyper-responsiveness (BHR) and lung function impairment.5 6 None of these studies attempted to characterise patients with asthma phenotypically regarding clinical symptoms, lung function and BHR according to their inflammatory patterns.
The overall hypothesis of this report is that phenotypic characteristics of patients with asthma vary depending on the amount of circulating eosinophils and neutrophils. Using data from the EGEA study, the aim of the present study is to assess phenotypic characteristics among 381 well-characterised adults with asthma according to their blood inflammatory pattern. Four inflammatory patterns were considered, depending on eosinophils and neutrophils, like those proposed by Simpson7 in induced sputum. Respiratory symptoms were those typical of asthma and those typical of chronic obstructive pulmonary disease (COPD), composite scores of symptoms potentially reflecting some clinical severity, lung function and BHR. Analyses took into account the two other allergy markers, skin prick test response and total IgE, highly related to eosinophils, and smoking highly related to neutrophils.
METHODS
Study design
The EGEA survey (1991–1995) combines a case–control study with a family study of cases with asthma.8 Briefly, cases with asthma were recruited in chest clinics in five French cities, and relatives with asthma were recruited following answers to a detailed questionnaire by cases regarding respiratory symptoms, environment and treatment. The study was approved by the relevant institutional review boards, and written informed consent was obtained from each subject. Of the 2047 subjects (904 children, 1143 adults), 217 were adult cases, and, among the 794 adult relatives, 191 had asthma. The present study includes the 381 adults with asthma (200 cases and 181 relatives) with available blood eosinophil and neutrophil cell counts.
Phenotypes
In the cases, asthma was defined by a positive answer to four standardised questions: “Have you ever had attacks of breathlessness at rest with wheezing?”, “Have you ever had asthma attacks?”, “Was this diagnosis confirmed by a doctor?” and “Have you had an asthma attack in the last 12 months?”. In family members, asthma was defined by a positive answer to the first or the second question. Symptoms typical of asthma (chest tightness, shortness of breath, cough and nocturnal symptoms) and symptoms typical of COPD (chronic cough, chronic phlegm, dyspnoea grade 3) were recorded by standardised questionnaires.8 9 Two composite scores already used in the literature, and capturing different dimensions of the expression of the disease, were studied.10 11 The first score,10 varying from 1 to 4, based on 2002 GINA (Global Initiative for Asthma) guidelines, combines clinical data (frequency of asthma attacks, persistent symptoms between attacks and hospitalisation in the past 12 months) and treatment (inhaled corticosteroids (ICS) in the past 12 months), was labelled here as the asthma event score.12 The second score, proposed by Pekkanen,11 labelled here as the asthma symptomatic score, varying from 1 to 5, is based on the number of asthma symptoms (wheeze and breathlessness, woken with chest tightness, woken by an attack of shortness of breath, attack of shortness of breath at rest, attack of shortness of breath after exercise). Total IgE determination, skin prick tests to 11 allergens and a lung function test with methacholine challenge were performed.8
Inflammatory patterns
Subjects were asked to avoid smoking for at least 1 h and to avoid use of their inhaler for at least 4 h prior to testing. Four inflammatory patterns were defined from white blood cell counts (WBCs) according to eosinophil (EOS) and neutrophil (NEU) count cut-off points. Samples with ⩾250 EOS/mm3 were classified as EOShi. The cut-off point for eosinophils, commonly used in epidemiology, corresponded to the 75th percentile in the 1356 adults from the EGEA study.
In our population, only 27 patients with asthma had a neutrophil count equal to or higher than the upper limit adult reference of 6700 cells/mm3.13 Therefore, a cut-off point corresponding to the 75th percentile was also chosen for neutrophils (5000 NEU/mm3), and samples with ⩾5000 NEU/mm3 were classified as NEUhi. A cut-off point corresponding to the 90th percentile (6040 NEU/mm3) was also studied (data not shown). Subjects were classified as EOSlo/NEUlo, EOSlo/NEUhi, EOShi/NEUlo and EOShi/NEUhi.
Statistical analysis
Phenotypic characteristics were first compared between subjects with the EOSlo pattern and those with the EOShi pattern. Then, among subjects with the EOSlo and EOShi pattern, phenotypic characteristics were compared regarding neutrophilic inflammation (EOShi/NEUlo vs EOShi/NEUhi, and EOSlo/NEUlo vs EOSlo/NEUhi, respectively). For COPD-like symptoms, comparisons were also performed between subjects with the NEUlo and those with the NEUhi pattern, according to current smoking status. Standard statistical tests (χ2 or Fisher exact test when appropriate, univariate and multivariate regression analyses adjusting for confounders) were performed. Due to the familial aggregation of the data, all multivariate analyses were conducted using generalised estimated equations (GEEs) to take into account dependence between observations (GENMOD and MIXED procedures in SAS), unless there were <10 families which included more than one subject (in such a situation, one individual was chosen at random and the analysis was redone with the standard test). All statistical analyses were done using SAS version 9.1 (SAS Institute, Cary, North Carolina, USA).
RESULTS
The overall characteristics of the 381 adults with asthma are summarised in table 1. As expected, women reported dyspnoea more frequently than men (odds ratio (OR) 1.93, 95% CI 1.17 to 3.18). Eosinophil and neutrophil counts were significantly higher in ICS users than in non-users (mean (SD), 304 (218) cells/mm3 vs 244 (174) cells/mm3, p = 0.003, and 4362 (1914) cells/mm3 vs 4029 (1330) cells/mm3, p = 0.05, respectively). No significant association was found between eosinophil and neutrophil counts and hour of blood withdrawal, or use of concomitant medications such as antihistaminic drugs, phenothiazines or imipramine (not shown).
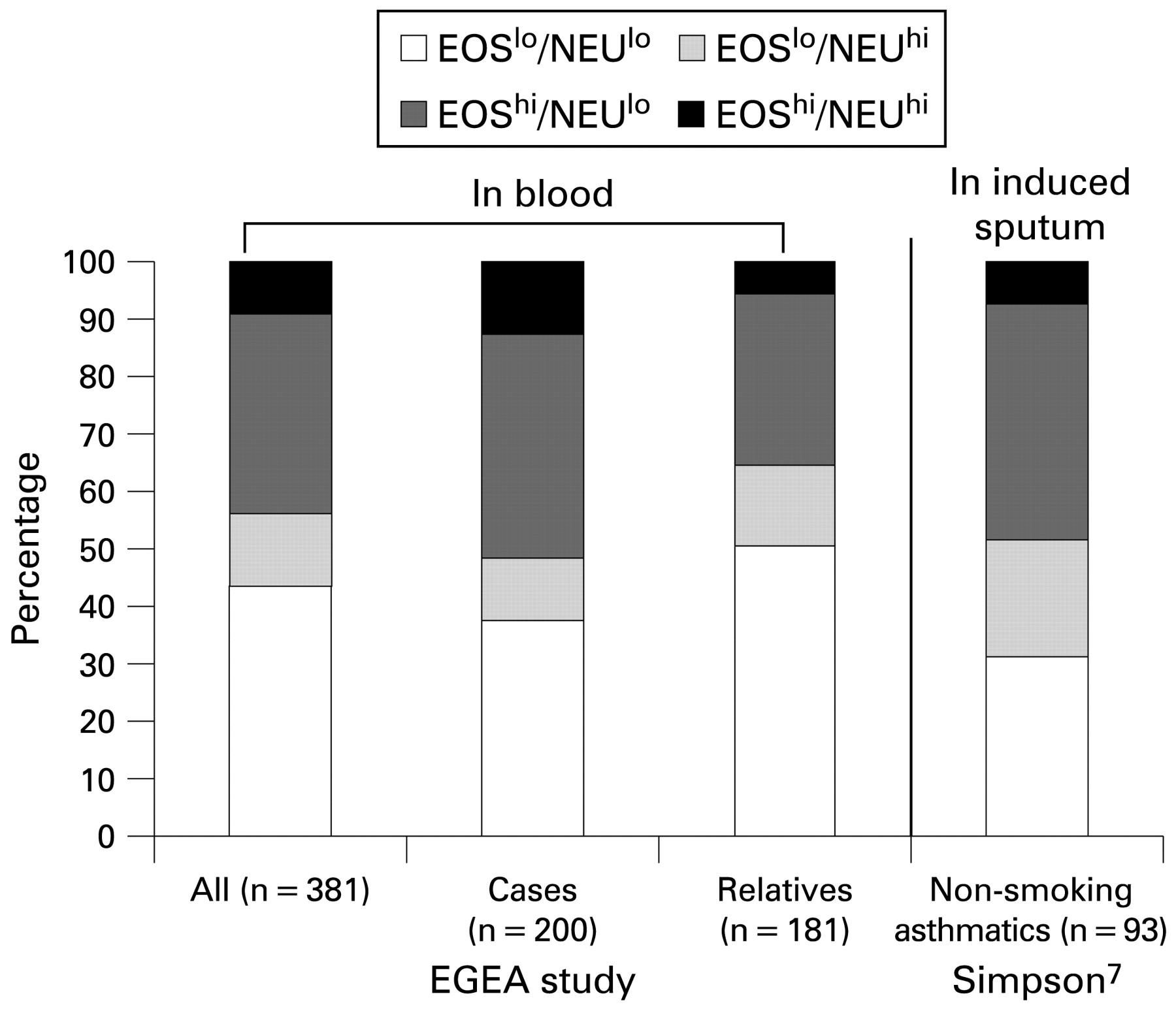
EOSlo/NEUlo, EOSlo/NEUhi, EOShi/NEUlo and EOShi/NEUhi patterns concerned 43.6, 12.6, 34.6 and 9.2% of the 381 adults with asthma (fig 1).

Frequency of each inflammatory pattern in adults with asthma. Numbers of patients with asthma are shown below each bar. EGEA study, Epidemiological study on the Genetics and Environment of Asthma; EOS, eosinophils; NEU, neutrophils.
Comparison of asthma and COPD-like symptoms among patients with asthma with the eosinophilic and non-eosinophilic pattern
Patients with asthma with the EOShi pattern had significantly higher total IgE than those with the EOSlo pattern (table 2), which remained significant after adjustment for age, sex and smoking: 233 vs 117 IU/ml, p<10−4. They also had significantly lower FEV1 (forced expiratory volume in 1 s) with adjusted values of 89.4 vs 96.5%, (p = 0.0003), and higher BHR than those with the EOSlo pattern (tables 2 and 5).
Patients with asthma with the EOShi pattern reported significantly more asthma attacks in the last 12 months, and more often being woken by an attack of shortness of breath or with chest tightness than those with the EOSlo pattern (tables 3 and 5). They also had a significantly higher asthma event score and symptomatic score than those with the EOSlo pattern, with adjusted values of 2.64 vs 2.22, p = 0.001, and 3.46 vs 2.69, p<10−4 respectively. Further adjustment for ICS treatment did not change the conclusion (not shown).
For COPD-like symptoms, patients with asthma with the EOShi pattern reported significantly more dyspnoea than those with the EOSlo pattern (table 4), though the association was no longer significant in the multivariate analysis (table 5). This association was observed in both men and women.
Neutrophil inflammation among patients with asthma with the eosinophilic pattern
Patients with asthma with the EOShi/NEUhi pattern were older and more frequently women (OR = 2.25 (1.02 to 4.96)) than those with the EOShi/NEUlo pattern.
Despite a higher frequency of treatment with ICS, those patients with asthma who had the EOShi/NEUhi pattern reported significantly more often being woken with chest tightness or by an attack of coughing than those with the EOShi/NEUlo pattern (table 3), an association which remained significant for chest tightness after adjustment (table 5). Patients with asthma with the EOShi/NEUhi pattern also reported more nocturnal symptoms considered together than those with the EOShi/NEUlo pattern. Excluding being woken by an attack of coughing from nocturnal symptoms did not change the conclusion. Patients with asthma with the EOShi/NEUhi pattern have a significantly higher asthma symptomatic score than those with the EOShi/NEUlo pattern, independently of age, sex and smoking (4.04 vs 3.36, p = 0.03), an association which became of borderline significance after further adjustment for ICS treatment (3.84 vs 3.31, p = 0.07).
For COPD-like symptoms, patients with asthma with the EOShi/NEUhi pattern reported significantly more dyspnoea than those with the EOShi/NEUlo pattern, but the difference did not reach the level of significance after adjustment (tables 4 and 5).
Neutrophil inflammation among those with asthma with the non-eosinophilic pattern
Patients with asthma with the EOSlo/NEUhi pattern were more often current smokers than those with the EOSlo/NEUlo pattern (OR = 3.54 (1.78 to 7.04)) (table 2). They had fewer positive skin prick test responses than those with the EOSlo/NEUlo pattern (tables 3 and 5). No other differences were observed.
Comparisons of COPD-like symptoms among those with asthma with the neutrophilic and non-neutrophilic pattern
Although chronic cough and chronic phlegm were more frequently reported by those with asthma with the neutrophilic pattern (EOSlo/NEUhi or EOShi/NEUhi, n = 48+35, NEUhi) than in those with the non-neutrophilic pattern (EOSlo/NEUlo or EOShi/NEUlo, n = 166+132, NEUlo) (table 4), associations did not reach the level of significance, with OR = 1.32 (0.72 to 2.43) and 1.66 (0.85 to 3.22) for chronic cough and chronic phlegm, respectively. Patients with asthma with the NEUhi pattern reported significantly more dyspnoea than those with the NEUlo pattern (OR = 1.93 (1.12 to 3.35)). This association was similarly observed in men and in women, and remained significant after adjustment for age and smoking in women only, with OR = 2.08 (1.08 to 4.18), and OR = 1.89 (0.74 to 4.81) in men.
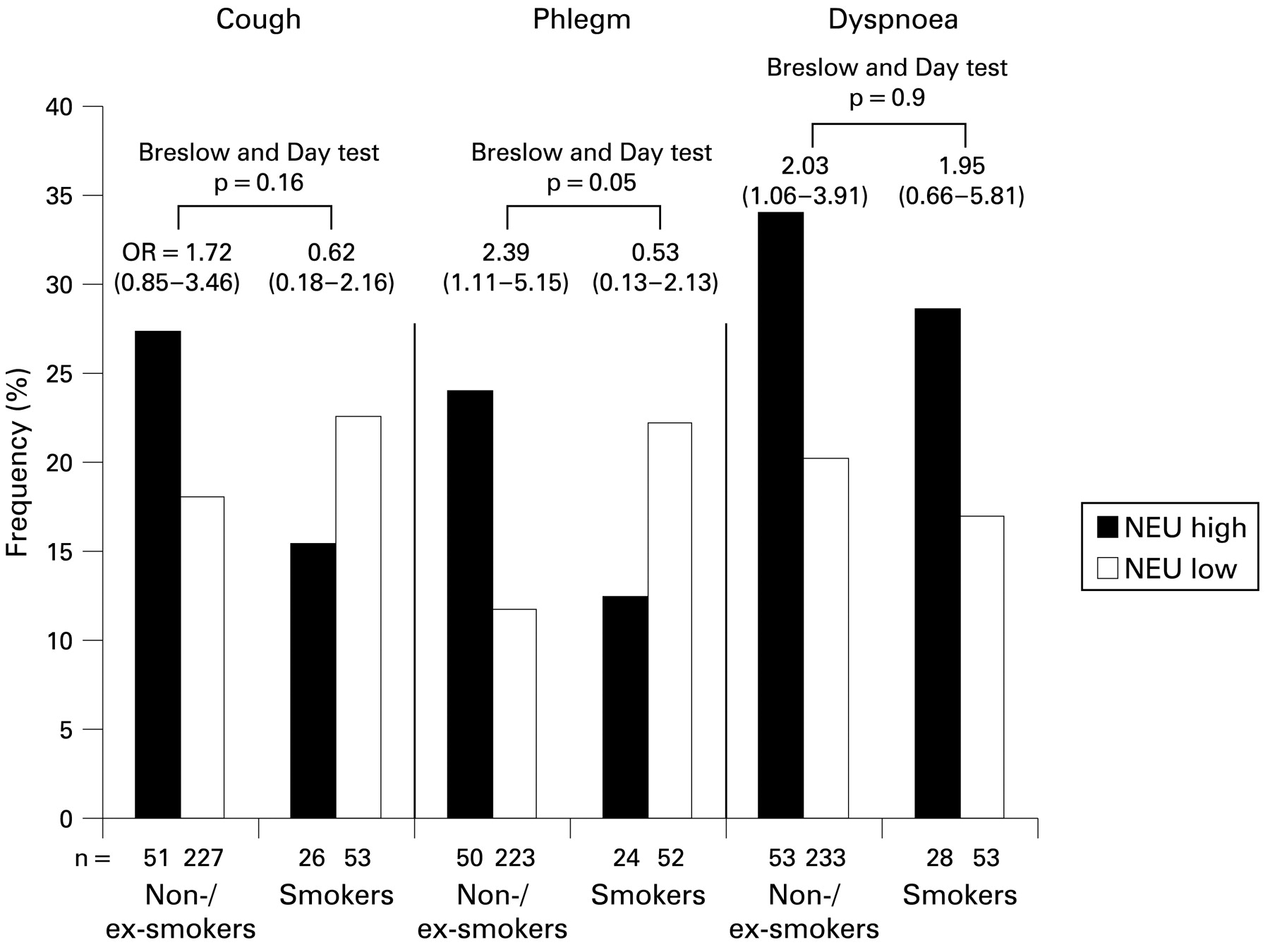
The relationships of COPD-like symptoms to the neutrophilic pattern were examined by current smoking status (fig 2). Only in non-smokers did those with asthma with the NEUhi pattern report significantly more chronic phlegm and dyspnoea than those with the NEUlo pattern. The association remained significant after adjustment for age, sex and eosinophilic inflammation, and taking into account familial dependence of the subjects for chronic phlegm only with OR = 2.35 (1.08 to 5.10), and OR = 1.83 (0.95 to 3.53) and 1.79 (0.89 to 3.57) for dyspnoea and chronic cough, respectively. Adjusting for respiratory infections in the last 3 weeks did not change the conclusion (not shown).

{kind=link}
{kind=link}
Associations of chronic obstructive pulmonary disease (COPD)-like symptoms, chronic cough, chronic phlegm and dyspnoea, with neutrophilic pattern according to current smoking. Black boxes, neutrophilic pattern (EOSlo/NEUhi or EOShi/NEUhi); white boxes: non-neutrophilic patterns (EOSlo/NEUlo or EOShi/NEUlo). The numbers of those with asthma are shown below each bar. p Values of Breslow and Day tests for interaction, which refers to the heterogeneity of odds ratios according to smoking habits. EOS, eosinophils; NEU, neutrophils.
Analyses done with the cut-off point for neutrophils corresponding to the 90th percentile gave similar findings.
DISCUSSION
The present study shows marked differences in asthma phenotypic characteristics according to four blood inflammatory patterns defined by the amount of circulating eosinophils and neutrophils. The non-eosinophilic pattern (EOSlo) was present in 56% of the cases with asthma, the EOSlo/NEUlo pattern being present in the majority (77%) of these. Comparison of the EOShi with the EOSlo pattern confirms that EOShi had higher IgE, lower FEV1 and corresponds to more active asthma (frequency of events and symptoms). Among EOSlo, neutrophil inflammation (NEUhi) was related to less frequent positive skin prick test responses. Among EOShi, NEUhi did not explain current asthma or asthma event frequency, but was significantly related to nocturnal symptoms. In those with asthma who were not current smokers, COPD-like symptoms, in particular chronic phlegm, were more frequent in those with NEUhi, independently of eosinophilic inflammation.
The first strength of this study was the possibility to study simultaneously the four inflammatory patterns in a way similar to that proposed by Simpson7—that is, without overlap between the patterns, which was never done previously in epidemiology. Interestingly, the relative proportions of each pattern in our study were similar to those defined by Simpson7 using induced sputum. The good characterisation of patients with asthma, and their heterogeneity regarding asthma, made the EGEA the ideal population to assess phenotypic characteristics according to blood inflammatory patterns. The limitations of our study are those commonly related to comparisons of groups with small sample sizes and those related to cross-sectional analyses of the data. Inflammatory patterns were defined according to eosinophil and neutrophil counts in blood, a fluid which may be considered as reflecting lung inflammation less than induced sputum, but is more easily accessible in clinical practice. The eosinophil count cut-off point (250 cells/mm3) used was one commonly used in epidemiology, and a cut-off point of 5000 cells/mm3 was chosen for neutrophils. Both cut-off points corresponded to the 75th percentile among the 1356 adults of the EGEA, and the 75th percentile among the 901 adults who did not have asthma of the EGEA corresponded to the same neutrophil cut-off point. Increasing the neutrophil cut-off point of 15% did not change the main conclusions. Further, correlations between inflammatory markers, including eosinophils and neutrophils, in induced sputum and peripheral blood have only rarely been studied.14–18 The morphological and functional characteristics of bronchial eosinophils were similar to those of blood low-density eosinophils in patients with asthma,14 and concomitant decreases in FeNO and blood neutrophil counts were observed among bar workers 2 months after a legislative ban on smoking in public places,15 whereas no significant correlations between sputum and blood lymphocyte subsets in non-smoking adults with asthma were reported.16 In welders, only blood eosinophil count was related to the extent of welding,17 whereas both sputum and blood eosinophils decreased in those with asthma after treatment with steroids.18 These results suggest that blood and sputum eosinophils and neutrophils could respond differently to the same stimuli, and that the measurement of eosinophils and neutrophils in each of the specimens may give interesting complementary information.
Interestingly, in our population with asthma, around 56% had a “non-eosinophilic asthma”, a result similar to those reported in general populations, accounting for around 30–70% of those with asthma depending on the studies.1 Regarding eosinophil and neutrophil cut-off points, 44% of patients with asthma had an EOSlo/NEUlo pattern, suggesting that this pattern may represent another “type” of asthma in which blood inflammation is not a major feature, or that the disease was not active at the moment of the study.
We confirmed the well-documented associations of blood eosinophilic pattern with high IgE, increased BHR and lower FEV1 previously reported in general or occupational populations.5 6 19 Activated eosinophils are known to release several mediators which cause damage to the airway epithelium, leading to BHR due to increased permeability.20 We observed associations of the eosinophilic pattern with more asthma attacks and more nocturnal symptoms reported in the last 12 months, and higher asthma event score and symptomatic score. These two scores should be considered as continuous variables reflecting the activity of the disease and also its severity,10 21 and the peripheral eosinophil count has been suggested to be a marker of asthma activity.22
Among patients with asthma with the non-eosinophilic pattern, neutrophil inflammation was associated with less allergic sensitisation, a result which supports and extends previous reports,23 suggesting a different pathogenesis from allergen-induced asthma, possibly more related to environmental exposure to various pollutants such as ozone or particulates,1 and mediated through macrophages and epithelial cells rather than activated TH2 cells.24
Among those with asthma with the eosinophilic pattern, neutrophil inflammation was clearly associated with more reports of dyspnoea and nocturnal symptoms, and with a higher symptomatic score, suggesting a “more active” disease. No association was observed in those with asthma with non-eosinophilic inflammation, as previously found by Wenzel in induced sputum.25 There is also growing evidence supporting that increased neutrophilic inflammation is present in “more severe” asthma.26 Patients with asthma who have severe disease and are resistant to corticosteroids have raised neutrophil counts in their airways. Positive correlations between the concentrations of neutrophils and eosinophils in induced sputum from patients with severe asthma who are treated with drugs including corticosteroids have been reported.27 As those with asthma with the EOShi/NEUhi pattern were more often treated with ICS, the high eosinophil and neutrophil counts could be at least partially a consequence of steroid treatment, known to enhance neutrophil survival.28 Neutrophils may lead eosinophils to accumulate in the airways of patients with severe asthma and possibly aggravate the disease,29 and it is unlikely that eosinophils regulate neutrophilic inflammation.30 High eosinophil and neutrophil counts may also be related to exposure to specific environmental factors, in particular ozone, recently found to promote an antiapoptotic environment in allergen-primed animals.31 Overall, the relationships of neutrophil inflammation to asthma severity seem to depend upon the presence of eosinophil inflammation.
In our study, among those with asthma who had the eosinophilic pattern, those with neutrophil inflammation were older and more frequently women. Remodelling is known to increase with age and to be associated with neutrophilia.32 Activated neutrophils may release inflammatory mediators, oxygen radicals and proteases, which supports their involvement in the intense inflammation and remodelling found in severe asthma.33 Regarding nocturnal asthma, intricate circadian variations in inflammation and in physiological manifestations have been reported,34 including the proinflammatory hormone melatonin, and the hypothalamic–pituitary–adrenal axis. We previously found that in women with a history of premenstrual asthma, eosinophil counts were significantly higher than in other women with asthma, an association that remained after adjustment for asthma severity.35 Further, spontaneous neutrophil apoptosis is lower in healthy women as compared with men.36 Hormone-related events may have an influence on the relationships of high eosinophil and neutrophil numbers with symptoms of asthma. Despite the small sample size of the group of those with asthma who had the EOShi/NEUhi pattern, all our results suggest that these patients with asthma should be considered as having asthma with specific features different from those of those with eosinophilic inflammation alone.
Regarding COPD-like symptoms, our study revealed associations of the neutrophilic pattern with more frequent reports of chronic cough, chronic phlegm and dyspnoea. Significant associations of NEUhi with more frequent reports of chronic phlegm and dyspnoea occurred in non- or ex-smokers, whereas no association was observed in smokers. The prevalence of reported chronic phlegm in our study was similar to that in previous epidemiological studies conducted in general populations from various countries,37 38 and even when considering non-smokers only.39 The results should be interpreted with caution as they were based on cross-sectional analyses. In non- or ex-smokers, the results suggest that the association of hypersecretion with neutrophils reflects airway inflammation related to asthma and not to smoking. The lack of association in smokers may reflect a “healthy smoker effect”—that is, that smokers with asthma stop smoking earlier than controls.40 More attention should be paid to mucus hypersecretion in non-smokers. Analyses performed in our study did not allow the association of EOShi/NEUhi with female sex and dyspnoea to be disentangled; this could be specifically considered in future epidemiological studies.
In conclusion, as suggested by Wenzel,4 marked differences in phenotypic characteristics of asthma were evidenced according to blood inflammatory patterns. Besides eosinophilia, blood neutrophil inflammation is related to a different presentation of the disease. Epidemiological studies on blood inflammatory patterns may provide additional information to physiological studies, and may contribute to help to untangle this complex disease.
Acknowledgments
The authors thank Benedicte Jacquemin and Jean Maccario for helpful discussions.
REFERENCES
Footnotes
Funding: This research was funded in part by the INSERM/Ministry of Research, ANR 05-SEST-020-02/05-9-97, ANR-06-CEBS and the GA2LEN project, Global Allergy and Asthma European Network.
Competing interests: CP has not received any research grants from companies but received reimbursement from Novartis France, GlaxoSmithKline France, Boehringer Ingelheim France, AstraZeneca France and Actélion France for attending several conferences: ISHLT, ERS, CPLF.
Ethics approval: The study was approved by the relevant institutional review boards, and written informed consent was obtained from each subject.
The EGEA cooperative group. Coordination: F Kauffmann; F Demenais (genetics); I Pin (clinical aspects). Respiratory epidemiology: INSERM U 700, Paris, M Korobaeff (EGEA1), F Neukirch (EGEA1); INSERM U 707, Paris, I Annesi-Maesano; INSERM U 780, Villejuif, F Kauffmann, N Le Moual, R Nadif, MP Oryszczyn; INSERM U 823, Grenoble, V Siroux. Genetics: INSERM U 393, Paris, J Feingold; INSERM U 535, Villejuif: MH Dizier; Inserm U 794, Evry: E Bouzigon, F Demenais; CNG, Evry: I Gut, M Lathrop. Clinical centres: Grenoble, I Pin, C Pison; Lyon, D Ecochard (EGEA1), F Gormand, Y Pacheco; Marseille, D Charpin (EGEA1), D Vervloet; Montpellier, J Bousquet; Paris Cochin, A Lockhart (EGEA1), R Matran (now in Lille); Paris Necker, E Paty, P Scheinmann; Paris-Trousseau, A Grimfeld, J Just. Data and quality management: INSERM ex-U155 (EGEA1), J Hochez; INSERM U 780, Villejuif, N Le Moual, C Ravault; INSERM U 794, Paris, N Chateigner; Grenoble, J Ferran.
Linked Articles
- Airwaves
- Editorial