Article Text

Abstract
Background: Although several risk factors for asthma have been identified in infants and young children with recurrent wheeze, the relevance of assessing lung function in this group remains unclear. Whether lung function is reduced during the first 2 years in recurrently wheezy children, with and without clinical risk factors for developing subsequent asthma (ie, parental asthma, personal history of allergic rhinitis, wheezing without colds and/or eosinophil level >4%) compared with healthy controls was assessed in this study.
Methods: Forced expiratory flows and volumes in steroid naïve young children with ⩾3 episodes of physician confirmed wheeze and healthy controls, aged 8–20 months, were measured using the tidal and raised volume rapid thoracoabdominal compression manoeuvres.
Results: Technically acceptable results were obtained in 50 wheezy children and 30 controls using tidal rapid thoracoabdominal compression, and 44 wheezy children and 29 controls with the raised volume technique. After adjustment for sex, age, body length at test and maternal smoking, significant reductions in z scores for forced expiratory volume at 0.5 s (mean difference (95% CI) −1.0 (−1.5 to −0.5)), forced expired flow after 75% forced vital capacity (FVC) has been exhaled (FEF25) (−0.6 (−1.0 to −0.2)) and average forced expired flow over the mid 50% of FVC (FEF25–75) (−0.8 (−1.2 to −0.4)) were observed in those with recurrent wheeze compared with controls. Wheezy children with risk factors for asthma (n = 15) had significantly lower z scores for FVC (−0.7 (−1.4 to −0.04)) and FEF25–75 (−0.6 (−1.2 to −0.1)) than those without such risk factors (n = 29).
Conclusions: Compared with healthy controls, airway function is reduced in young children with recurrent wheeze, particularly those at risk for subsequent asthma. These findings provide further evidence for associations between clinical risk factors and impaired respiratory function in early life.
Statistics from Altmetric.com
Recurrent wheeze is a common symptom during infancy and early childhood.1 2 Although the majority of children will outgrow their symptoms, some go on to develop asthma.3 4 Early onset of asthma has been associated with persistence of symptoms and reduced lung function that continues into adulthood.5–7 A recently described clinical index considers young children with recurrent wheezing in the first 3 years of life to be at high risk of developing asthma if there is a parental history of asthma or personal history of eczema, or if two of the following are present: personal history of allergic rhinitis, wheezing without a cold and/or serum eosinophil level >4%.8 Other predictive indices additionally take immunological measurements1 and clinical parameters into account9 but these indices cannot be easily applied to daily practice.
Apart from clinical risk factors, lung function evaluation may contribute to the assessment of wheezing phenotypes during early life. A reduction in premorbid lung function has been associated with increased risk of wheezing in the first years.3 10–12 Tracking of lung function (whereby those with lower lung function initially continue to do so thereafter) has been well documented during infancy,5 13 14 childhood15 16 and adulthood.5 7 17 However, the association between wheezing phenotypes and early airway function remains unclear. The Tucson study reported a link between reduced maximal forced expiratory flow at functional residual capacity (V’maxFRC) from the tidal rapid thoracoabdominal compression (RTC) technique, in the first weeks of life prior to the onset of respiratory symptoms, and transient wheeze but not with persistent wheeze.2 Similarly, data from Wilson et al found no association between wheezing beyond 4 years and reduced V’maxFRC at 4 weeks of age.18 In contrast, the Perth group reported that persistent wheeze/asthma at 11 years was associated with reduced premorbid V’maxFRC at 1 month.16 A further study observed that children with transient wheeze had lower V’maxFRC at 17 months compared with those with persistent wheeze.19 Others have suggested that asymptomatic children with evidence of flow limitation during tidal breathing in the first days of life are likely to have a higher risk of subsequent asthma.20
In recent years, several investigators have reported that, compared with tidal RTC manoeuvres, the raised volume RTC technique is more sensitive in distinguishing lung function between infants with and without respiratory disease.21–24 The raised volume technique has been used in children with24 25 and without recurrent wheezing26 but not, to our knowledge, to compare lung function in wheezy young children according to the risk of developing asthma.
This aim of this study was to assess whether lung function was reduced during the first 2 years of life in recurrently wheezy children with a high risk of developing subsequent asthma8 compared with age matched “low risk” wheezy children and healthy controls.
METHODS
Subjects
Infants and young children, aged between 8–20 months, with recurrent wheeze (⩾3 episodes of medically diagnosed wheeze) but prior to receiving any inhaled corticosteroid or anti-leukotriene agents, were recruited from the outpatient clinic in Hospital Dona Estefania, Lisbon (September 2005 to September 2007). Children requiring hospitalisation for exacerbations were ineligible for the study. Children were stratified into high and low risk for developing asthma.8
Age matched healthy children without a prior history of lower respiratory illness, wheeze or allergic disorders (food allergy, eczema) or parental asthma were recruited from those attending routine developmental screening appointments. Control children meeting the inclusion criteria, and who had been recruited to epidemiological studies at the UCL Institute of Child Health, London, UK,14 were also included in the study population.
All children were born ⩾37 gestational weeks with birth weight >10th percentile, and any with cardiac, metabolic, neurological or gastrointestinal diseases, or upper airway pathology were excluded.
The ethics committees at the Lisbon and London institutions approved the study. Parents of participating children gave informed written consent and were present during measurements.
Respiratory function tests
At the time of the assessments, infants were free of respiratory symptoms or illness for at least 3 weeks. Weight and crown–heel length were measured using digital scales and a calibrated stadiometer, and values expressed as z scores.27 Lung function measurements were undertaken in the supine position during quiet sleep following oral administration of chloral hydrate (60–75 mg/kg). Prior to sedation, the child’s heart rate and oxygen saturation level were recorded, and continuous monitoring maintained throughout the test period.
Identical equipment (VIASYS Healthcare Masterscreen BabyBody, V.4.6, Hochberg, Germany) and standardised techniques, which adhered to international guidelines,28 29 were used in both laboratories. The London team provided training for the Lisbon group and ongoing supervision throughout the study through inter-laboratory visits; all datasets were cross analysed anonymously. A lung inflation pressure of 30 cm H2O was used during the raised volume test.28 At least two technically satisfactory and reproducible (within 10%) partial and raised volume forced expiratory flow volume curves were collected.28 29 Detailed descriptions of both techniques, including quality control criteria, are available in the online supplement. Results were reported as z scores,30 31 values being considered abnormal if below −1.96 z score.
A questionnaire was completed by parents documenting smoking habits, family history of allergic illness and their child’s respiratory symptoms or illnesses since birth. Peripheral blood samples for eosinophil levels were obtained in those with recurrent wheeze when seen at the outpatient clinics.8
Sample size and statistical analysis
Power calculations indicated that 35 children per group would provide 80% certainty of detecting differences of 0.67 in z scores at the 5% significance level for the selected outcome variables between wheezy infants and controls. For subgroup analysis according to wheezing phenotype, 20 per group would provide 80% power to detect differences of 0.9 in z score.32
Comparisons of group characteristics and lung function between study groups were performed using independent sample t tests with 95% confidence intervals (CI) and χ2 tests. The extent to which recurrent wheeze is associated with lung function was also examined using multiple linear regression (MLR) (SPSS for Windows, V.15, Chicago, Illinois, USA) after adjustment for sex, age, body weight and length, and effects of potential confounding factors, such as maternal smoking.
RESULTS
Parents of 82/94 (87%) eligible Lisbon wheezy children gave consent for lung function measurements and of these, 55/82 (67%) attended for tests (fig 1). Technically satisfactory V’maxFRC flow–volume curves were obtained in 50 wheezy infants whereas 44 had acceptable raised volume forced expiratory flow volume curves. In contrast, among the eligible Lisbon healthy children, 21/59 (36%) families gave consent and of these, 14 (24%) attended for tests. Technically acceptable data were obtained in 12 healthy Lisbon children for V’maxFRC and 11 for the raised volume technique. Technically satisfactory data using both partial and raised volume manoeuvres were collected in 18 healthy children in London.

At birth, there was no significant difference in gestational age, weight or prevalence of smoking during pregnancy between the Lisbon and London controls, nor were there any significant differences in age or body size at the time of the tests or lung function results (see table E1 in the online supplement). Consequently, datasets from the two healthy subgroups were combined for comparison with wheezy children.
Comparison of wheezy and healthy groups
Gestational age of the wheezy group was 0.6 weeks lower than that of controls (p<0.02) but there were no significant differences in sex, birth weight or maternal smoking during pregnancy (table 1). At the time of the tests, wheezy children were somewhat older, heavier and longer than the healthy controls, primarily because of deferment of testing following upper respiratory infections in the wheezy infants. After expressing weight and length as z scores to adjust for age and sex, the wheezy group remained significantly heavier than controls, with no difference in length (table 1). There was a non-significant tendency for weight gain since birth to be greater among wheezy children (mean (95% CI) change in weight z score 0.4 (−0.1 to 1.0)).
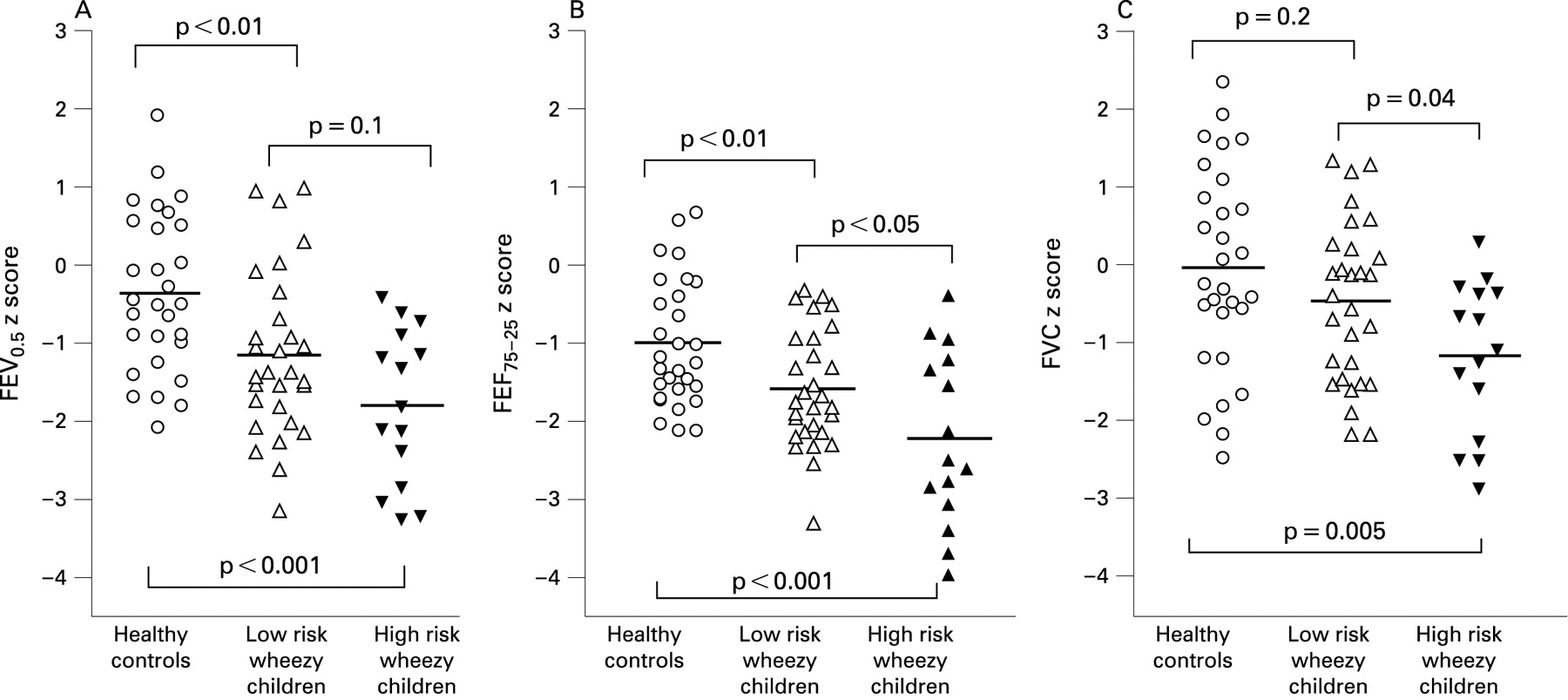
Z scores for forced vital capacity (FVC), forced expiratory volume at 0.5 s (FEV0.5), forced expired flow after 75% FVC has been exhaled (FEF75) and average forced expired flow over the mid 50% of FVC (FEF25–75) were all significantly lower in wheezy than in healthy children (fig 2) but no differences were observed in V’maxFRC z score, respiratory rate, tidal volume or ratio of time taken to reach peak tidal expiratory flow to total expiratory time (tPTEF:tE) between the groups (table 1).
{kind=link}
{kind=link}
Associations between lung function and wheezing phenotype were also examined after adjusting for factors that influenced lung function on univariable analysis (sex, birth weight z score, age and test length and smoking during pregnancy). After adjustment for these covariants, significant reductions (mean (95% CI), wheeze controls) were observed for FVC (−42 (−78 to −6) ml), FEV0.5 (−30 (−54 to −6) ml), FEF75 (−42 (−75 to −10)) and FEF25–75 ( −70 (−117 to −23) ml/s). Addition of change in weight z score since birth had minimal effect on these relationships.
After adjustment for other factors, FVC was 57 (21 to 92) ml higher in boys than girls and 26 (5 to 48) ml higher per unit increment in birth weight z score. Maternal smoking was not significantly associated with any outcome on MLR. There was no association between V’maxFRC and wheeze on MLR analysis.
Wheezing subgroups
Among the 17 infants at high risk for subsequent asthma8 (table 1), 13 (76%) had a history of parental asthma, five (29%) a personal history of rhinitis, 12 (71%) had wheezed without colds and nine (53%) had serum eosinophil levels >4%. When dichotomised into wheezy subgroups according to these risk factors, there were no significant differences in background characteristics between the three groups, apart from controls being slightly more mature at birth (table 1). After adjusting for age and sex, both wheezing subgroups were significantly heavier than controls at the time of the test (mean (95% CI) difference in weight z score for low risk wheezers (controls 0.6 (0.04 to 1.1) and high risk wheezers (controls 1.0 (0.3 to 1.8)).
FEV0.5, FEF75 and FEF25–75 z scores were all significantly lower in both wheezing subgroups compared with healthy controls; FVC z score was also lower in the high but not the low risk group (table 2, fig 2). Compared with low risk wheezers, FVC and FEF25–75 were significantly reduced in high risk young children (table 2, fig 2). A significant difference in V’maxFRC z score was only observed between the high risk wheezers and healthy controls. No significant differences were seen in respiratory rate, tidal volume or tPTEF:tE between the three groups (table 2).
The associations between lung function and wheezing phenotype were also examined using MLR after adjusting for factors found to be significant on univariable analysis (sex, birth weight z score, age and length at test, and maternal smoking). After adjustment for these covariants, FVC was significantly reduced in the high versus low risk group by −45 (−89 to −2) ml whereas, despite a trend towards lower values among high risk children, there were no significant differences in FEV0.5 (−25 (95% CI −56 to 7)) ml or FEF25–75 (−47 (−115 to 20) ml/s). Among the wheezy children, FEF25–75 was significantly lower (−78 (−149 to −8) ml/s) in those whose mothers had smoked during pregnancy.
DISCUSSION
Findings from our study demonstrated that, after adjustment for sex, age, length and maternal smoking, forced flows and volumes from the raised volume technique, but not V’maxFRC or any of the tidal breathing variables, were significantly reduced during the first 2 years of life in young children with recurrent physician confirmed wheeze compared with prospective healthy controls. Among recurrently wheezy infants, those with a positive clinical index for asthma had significantly reduced FVC and FEF25–75 than those without such risk factors.
Strengths and limitations
Interpretation of these findings and their clinical relevance depends on factors such as accuracy of measurements, lack of bias and the extent to which results can be generalised, as discussed below.
Population
Our sample included 59% of eligible wheezy young children who presented at clinic during a 2 year recruitment period. In an attempt to study a relatively homogenous group and collect essential baseline data prior to long term interventions, young children with recurrent wheeze were only eligible if they had not yet received inhaled corticosteroids or anti-leukotriene therapy, or had been hospitalised during exacerbations. Similarly, since our research questions specifically related to risk factors for wheezing, healthy controls were only eligible if there was no prior history of lower respiratory illness, wheeze, allergic disorders or parental asthma. Children born prematurely or small for gestational age were excluded from index and control groups. While these stringent criteria inevitably excluded a number of children who would otherwise have been eligible, they allowed us to undertake a comparison of steroid naïve, recurrently wheezy young children versus healthy controls, without additional bias related to preterm delivery13 or intrauterine growth restriction,14 both of which can impact negatively on subsequent lung development.
Among the wheezy children enrolled, 28% could not be tested: either because they became too old for inclusion or because of hospitalisation/treatment with corticosteroids/anti-leukotrienes before they could be tested. Results from this study may therefore underestimate the true magnitude of the difference between groups as some of the more severely affected children were excluded. Despite this, when using the raised volume technique, clear differences were evident not only between wheezy infants and healthy controls but within the wheezing group according to risk factors.
Index children were slightly older than controls at time of the test (table 1), both because of the requirement for at least three episodes of physician confirmed wheeze prior to recruitment and postponements of tests as a result of respiratory illness, particularly in those with viral associated wheeze. After adjustment for age and sex, the wheezy infants were significantly heavier, although not longer, than the healthy controls. While the reason for this is unclear, by expressing lung function as z scores or adjusting for age and length when using MLR, such differences were accounted for when ascertaining the effect of wheeze on lung function. Turner et al33 reported a negative association between postnatal weight gain and change in length adjusted V’maxFRC in some infants between 1 and 12 months of age. They speculated that, in infants with reduced birth weight but accelerated “catch-up” during infancy, somatic growth may outstrip that of the lungs, resulting in reduced lung function. Although we excluded any infants with low birth weight for gestational age, a similar phenomenon might have occurred in those with rapid weight gain. However, we did not observe any significant relationship between change in weight and lung function, once other covariants had been adjusted for.
Ideally we would have assessed bronchodilator responsiveness in this study but this would have prolonged test duration and potentially jeopardised success rates. Furthermore, although airway obstruction may be largely reversible in older subjects with asthma, bronchodilator response is far more variable among wheezy infants, many of whom may show no improvement or even paradoxical responses.22
Power of study
This study was well powered to identify clinically significant differences (0.67 z scores) between wheezy children and controls. Original power calculations were based on 35 in each group. The final study population consisted of 73 children (44 wheezy, 29 controls). Retrospective power calculations confirmed that with a 1.5:1 imbalance between groups, there would be the same power as 35/group. Similarly, although there was an imbalance of 1.9:1 between the wheezy subgroups (29 low; 15 high risk), the total of 44 subjects provided the same power as 20/group. Nevertheless, the lower numbers meant that there was only 60% power of detecting differences as small as 0.67 z scores (80% for detecting 0.9 z score), increasing the risk of type II errors during subgroup analysis, especially during MLR.
Lung function testing and results
The standardised approach to data collection and analysis between the two centres was one of the strengths of this study. The London team provided intensive training to the Lisbon principal investigator (LMB), followed by the establishment of identical infant lung function equipment and measurement protocols in Lisbon. In addition, regular inter-laboratory site visits and cross analysis of data were undertaken throughout the duration of the study to minimise bias.
Results from this study suggest that while lung function is reduced in infants with recurrent wheeze but low risk for subsequent asthma, these differences are less marked than in those at high risk. The reduction in FVC in the wheezy children, which was accompanied by reduced flows, was more evident in the high risk group, and probably reflects small airway obstruction and airway closure at low volumes during forced expiration rather than any alteration in lung growth or gas trapping during spontaneous breathing. While reductions in FVC can also occur because of gastric distension during the raised volume rapid thoraco-abdominal compression,28 we took particular care to exclude this possibility by checking that there was no systematic fall in FVC between the first and last manoeuvre. Similarly, data from manoeuvres where there was any indication of early termination of forced expiration were excluded (see online supplement).
We were not able to assess resting lung volume in this study because of the limited duration of sleep in many of the subjects but had there been any dynamic elevation of functional residual volume in those who wheezed, measures of V’maxFRC would have been obtained at a higher volume than in healthy controls, thereby minimising differences between groups.21 This, together with the intrinsic variability of end expiratory level during infancy, could contribute to the reduced sensitivity of the partial compared with the raised volume technique in differentiating between those with and without prior wheeze. Although some studies have reported reductions in V’maxFRC in wheezy infants,34 35 recent publications suggest that the raised volume technique is more discriminative.21–24
It has been reported that tidal breathing indices such as tPTEF:tE may be associated with subsequent wheezing or asthma in later life.20 36 Significant associations between tPTEF:tE and subsequent outcome have, however, largely been limited to large epidemiological studies with premorbid assessments of tidal breathing measured shortly after birth, a time when modulation of expiratory flows and timing is most active. In this study, tPTEF:tE was slightly, but not significantly, lower in wheezy infants; this relative lack of discrimination of tidal breathing parameters in older infants with prior wheeze being in keeping with previous reports.37
In contrast with previous publications,2 37 we did not find a significant effect of maternal smoking during pregnancy although flows tended to be lower in those exposed. This may reflect the relatively small subgroups, the highly selected nature of the population or some interaction between the effects of wheezing and maternal smoking on measured flows. In support of this contention, when analysis was limited to wheezy infants, flows were significantly lower in those whose mothers had smoked.
CONCLUSIONS
We have demonstrated that lung function is reduced in infants and young children with recurrent wheeze, and that these changes are most marked in those at high risk of subsequent asthma. Findings from this study suggest that the raised volume technique is able to identify diminished lung function in wheezy infants compared with controls, and between wheezy subgroups according to clinical risk factors. Given the overlap between groups, it is, however, unlikely that such tests would be able to predict persistent wheeze within individuals.
While further work is still required to establish short and long term repeatability, use of such physiological measures in combination with clinical symptoms and risk factors could potentially influence therapeutic interventions.
Acknowledgments
We thank the parents who consented for their infants and young children to participate in this study and staff at the Hospital de Dona Estefânia, Lisbon, and Portex Respiratory Unit, UCL Institute of Child Health, London, for their support. We thank Dr Sooky Lum for her assistance in providing technical training.
REFERENCES
Supplementary materials
web only appendix 64/3/203
Files in this Data Supplement:
Footnotes
Additional material published online only at http://thorax.bmj.com/content/vol64/issue3
Funding: We thank Schering Plough for financial support towards travel expenses which enabled collaborative work between the two institutions (Hospital de Dona Estefânia, Lisbon and Portex Respiratory Unit, UCL Institute of Child Health, London).
Competing interests: None.
Ethics approval: The ethics committees at the Lisbon and London institutions approved the study.