Article Text

Abstract
Objective: Resection is the best treatment for patients with stage I non-small cell lung cancer (NSCLC). Patterns of disease recurrence after complete resection in stage I NSCLC have not been well demonstrated. The aim of this study was to evaluate the prognostic predictors of post-recurrence survival in patients with resected stage I NSCLC with local recurrence.
Methods: The clinicopathological characteristics of 123 patients with local recurrence after complete resection of stage I NSCLC in Taipei Veterans General Hospital between 1980 and 2000 were retrospectively reviewed. Post-recurrence survival and their predictors were analysed.
Results: The patterns of local recurrence included local only in 74 (60.2%) and both local and distant in 49 (39.8%) patients. The 1 and 2 year post-recurrence survival rates for the 74 patients with local only recurrence were 48.7% and 17.6%, respectively. Tumour size (p = 0.033) and treatment for initial recurrence (p<0.001) were significant predictors for post-recurrence survival in 74 patients with local only recurrence in univariate analyses. The hazard of death was greater in patients with larger tumour size. Treatment for initial recurrence (p = 0.001) was still a significant prognostic indicator in multivariate analyses. Patients who underwent reoperation after local recurrence survived longer than those who received chemotherapy and/or radiotherapy and those that received no treatment.
Conclusions: Treatment for initial recurrence is a prognostic predictor for post-recurrence survival in resected stage I NSCLC with local recurrence. Complete surgical resection should be considered in selected candidates with resectable local recurrent disease.
Statistics from Altmetric.com
Lung cancer is the leading cause of cancer death worldwide. Surgical resection is the treatment of choice for early stage non-small cell lung cancer (NSCLC).1 Patients with stage I disease have the most favourable prognosis. Five year survival after resection ranges between 55% and 80%.1–5 Recurrence is the most common cause of disease failure and mortality for NSCLC after resection.4–8 Reported recurrence rates after surgical resection in stage I NSCLC range from 27% to 38%.4–6 The incidence of local or regional recurrence in stage I NSCLC after surgical resection has been reported to be between 7% and 15%.4–6 Chemotherapy, radiotherapy or combined therapy are common treatment modalities for patients with resected NSCLC after recurrence. However, reoperation after recurrence is only appropriate in a few patients.7–9
Although the prognosis of stage I NSCLC is relatively good compared with more advanced stages,3–5 the course and predictors of post-recurrence survival in resected stage I NSCLC with local recurrence have rarely been reported. Few studies have focused on the outcome and post-recurrence survival of surgically treated patients with stage I NSCLC after local recurrence. In this report, we analysed the patterns of local recurrence and demonstrated the prognostic predictors of post-recurrence survival in resected stage I NSCLC with local recurrence.
PATIENTS AND METHODS
Between January 1980 and December 2000, 970 patients underwent resections for pathological stage I NSCLC at Taipei Veterans General Hospital. The preoperative staging workup was done as previously described.10 11 Chest and upper abdomen CT scans, nuclear medicine survey (bone and brain) and bronchoscopy were performed before operation. Mediastinoscopy was performed only when the CT scan showed enlarged mediastinal lymph nodes (diameter >1.0 cm). Patients suspected of having distant metastases were excluded from consideration. All patients underwent complete resection of the lung cancer with mediastinal lymph node dissection as previously described.10 11 The resected specimens and all dissected regional nodes were examined for pathological staging. None of the patients had received adjuvant therapy after initial surgical resection for stage I NSCLC. The hospital charts of all patients were reviewed, including operative records and pathological reports. Histological typing was determined according to the World Health Organization classification.12 Determination of disease stages was based on the TNM classification of the International Union Against Cancer.13
All patients were followed-up at our outpatient department with an interval of 3 months in the first 2 years after resection and an interval of 6 months thereafter. Of the 970 patients, complete follow-up was available in 933 patients (96.2%). During that period, local recurrence after surgical resection was detected in 123 (13.2%) of the 933 patients. The characteristics of these 123 patients according to patterns of local recurrence (local only or local with distant) are listed in table 1. To investigate their impact on post-recurrence survival, the following clinicopathological factors were used in univariate and multivariate analyses: age at recurrence, gender, smoking index, laterality of tumour (right vs left), histological type of the tumour (squamous cell carcinoma vs others), tumour size, extent of pulmonary resection (sublobar resection vs lobectomy or bilobectomy or pneumonectomy), T status (T2 vs T1), visceral pleural invasion (present vs absent), number of mediastinal lymph nodes dissected (>15 vs ⩽15), disease free interval (>18 vs ⩽18 months), mediastinal recurrence (present vs absent) and treatment for initial recurrence (none vs with surgery vs chemotherapy and/or radiotherapy). Secondary primary lung cancer was differentiated from recurrent NSCLC according to the criteria proposed by Martini and Melamed.4 14 Local recurrence was defined as tumour recurrence in a contiguously anatomical site, including the ipsilateral hemithorax and mediastinum, after surgical resection. Distant recurrence was defined as tumour recurrence in the contralateral lung or outside the hemithorax and mediastinum after surgical resection. The length of post-recurrence survival was defined as the interval (in months) between the date of initial recurrence identified and the date of either death or the last follow-up. Treatment for local recurrence included surgical resection, chemotherapy, radiotherapy and combined modalities.
Post-recurrence survival was calculated by the Kaplan–Meier method.15 Univariate and multivariate analyses were performed by means of the Cox proportional hazards model using SPSS software (V.12.0; SPSS, Chicago, Illinois, USA). Backward stepwise regression procedure was used. Data for treatment of recurrence were only available in 41 of the 74 patients with local only recurrence. Only these 41 patients were entered into the multivariate analyses. Statistical analysis was considered to be significant when the probability value was <0.05.
RESULTS
Median follow-up time for all 933 surgically resected stage I NSCLC patients was 60.7 months (mean 71.1 (57.1) months). The overall 5 and 10 year survival rates were 51.7% and 31.8%, respectively. No recurrence was found in 644 (69.0%) of the 933 patients. The patterns of recurrence included distant only in 166 (17.8%), local only in 74 (7.9%), and local and distant in 49 (5.3%) patients.
Local recurrence after surgical resection developed in 123 (13.2%) of the 933 patients. Median follow-up time for these 123 surgically resected stage I NSCLC patients with local recurrence was 28.9 months (mean 35.7 (26.0); range 5.4–204.8). Median time to initial recurrence for these 123 patients was 15.2 months (mean 18.3 (13.5)). The 1 and 2 year post-recurrence survival rates were 48.0% and 18.7%, respectively. The patterns of local recurrence included local only in 74 (60.2%) and both local and distant in 49 (39.8%) patients (local with distant in 19, local before distant in 24 and distant before local in six). At the last follow-up session, only three patients were alive, 117 patients had died of cancer, one patient had died of other causes and two patients had died of unknown causes. Treatments after initial recurrence included surgery for 10 patients, chemotherapy for 18 patients, radiation for 20 patients and a combination of chemotherapy and radiotherapy for 15 patients. Sixteen patients had no treatment after initial recurrence (eight patients because of poor performance status, two patients sought alternative treatment, three patients refused treatment, one patient underwent surgery but the lesion was found to be unresectable and another two patients had unknown causes).
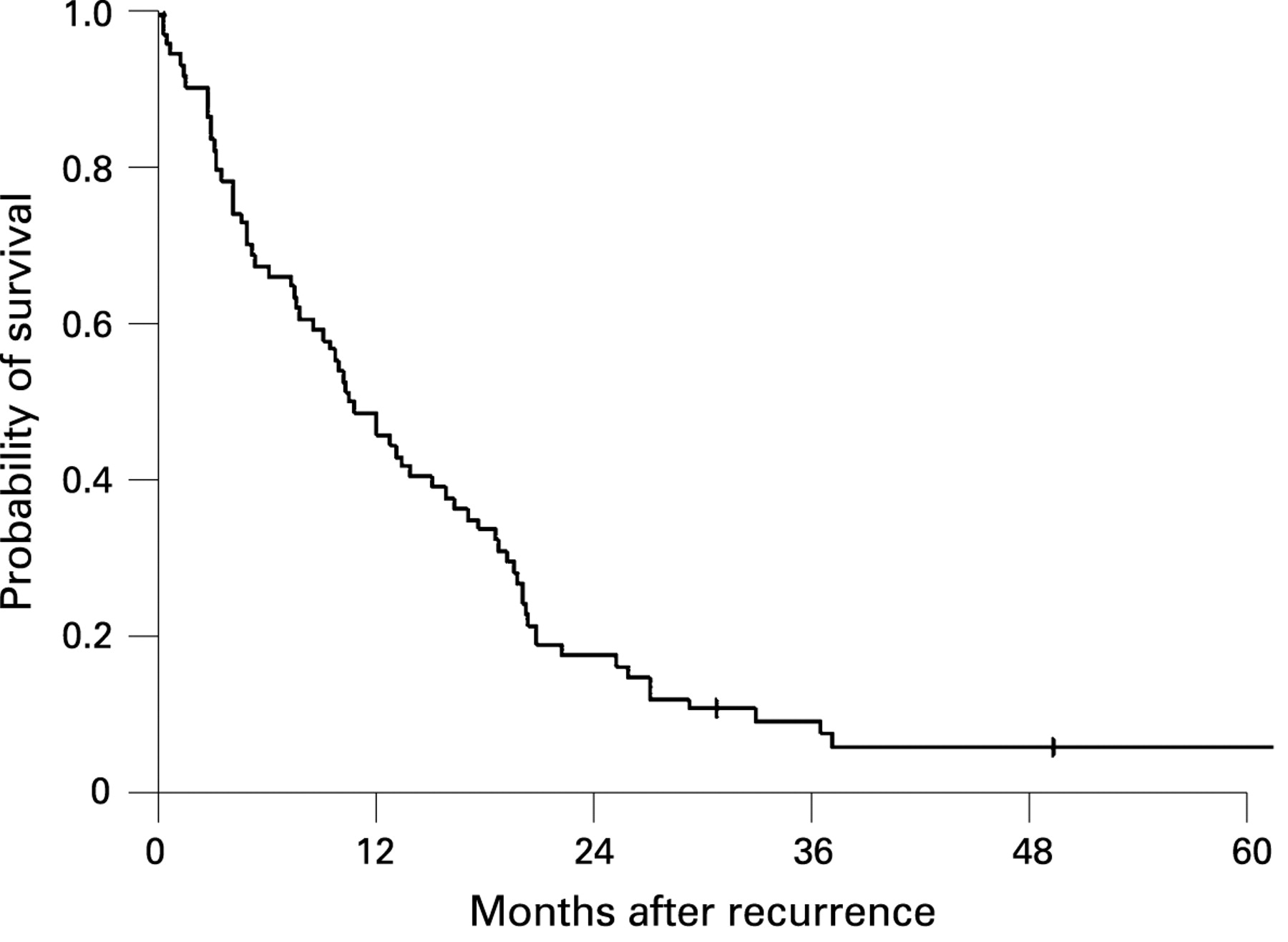
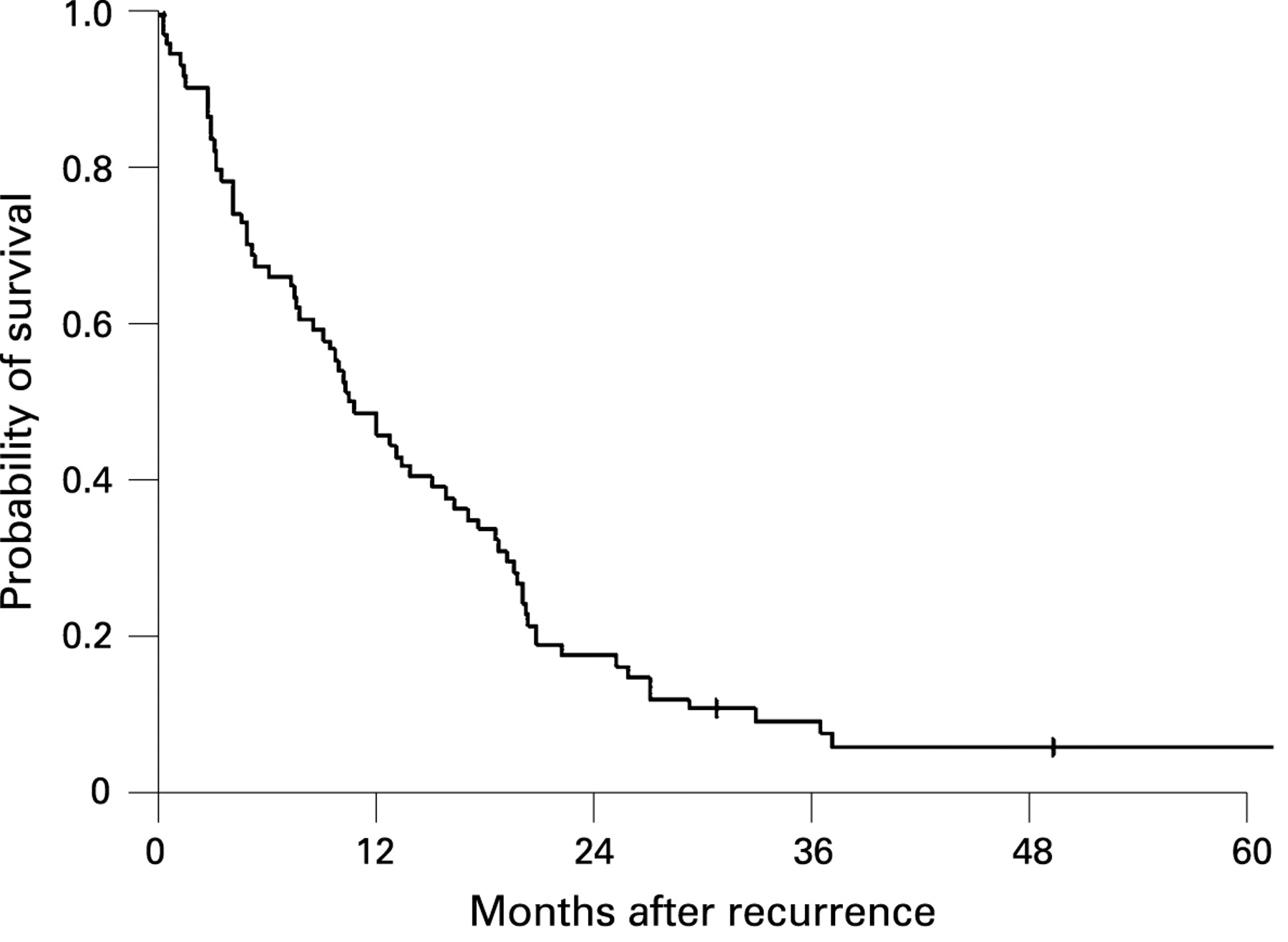
Median follow-up time for the 74 patients with resected stage I NSCLC with local only recurrence was 28.3 months (mean 36.1 (28.8); range 5.5–204.8). Median time to initial recurrence for these 74 patients was 16.8 months (mean 18.4 (12.0)). The 1 and 2 year post-recurrence survival rates were 48.7% and 17.6%, respectively (fig 1). The sites of initial local recurrence and treatment for initial recurrence in these patients with local only recurrence are listed in table 2. Among the eight patients who underwent reoperation, five had stump recurrence while the other three patients had recurrence at the lung parenchyma. A stump recurrence was more likely to undergo resection. Characteristics and outcome of all 10 patients (eight with local only and two with local and distant recurrences) who underwent reoperation after local recurrence are available as an online supplement (see supplementary table 1 online). The initial pulmonary resection was lobectomy in five patients, bilobectomy in two, wedge resection in two and pneumonectomy in one. The operation for recurrence was completion pneumonectomy in four patients, lobectomy in three, wedge resection in two and stump revision in one. Two postoperative deaths occurred, both with completion pneumonectomy. The 5 year post-recurrence survival of the 10 patients was 15%. Distant recurrences were detected in two patients after reoperation.
{kind=link}
Univariate analyses indicated that tumour size (p = 0.033) and treatment for initial recurrence (p<0.001) had a significant influence on post-recurrence survival in 74 patients of resected stage I NSCLC with local only recurrence (table 3). The hazard of death was greater in patients with larger tumour size. Patients who received surgery as treatment for the initial recurrence survived longer than those who received chemotherapy and/or radiotherapy. Furthermore, patients who received chemotherapy and/or radiotherapy survived longer than those who received no treatment. Treatment for initial recurrence (p = 0.001) was still a significant prognostic indicator in multivariate analyses (table 4). Patients with resected stage I NSCLC who underwent reoperation after local recurrence had a more favourable survival than those who received chemotherapy and/or radiotherapy and those who received no treatment. For the 38 patients with local only recurrence without mediastinal involvement, only treatment for the initial recurrence (p = 0.011) had a significant influence on post-recurrence survival in univariate analyses. Post-recurrence survival in patients with local only recurrence was not significantly different from that in those with both local and distant recurrences (p = 0.664).
DISCUSSION
Complete follow-up was achieved in 933 (96.2%) of the 970 surgically resected stage I NSCLC patients from January 1980 to December 2000. The overall 5 year survival for all 933 patients was 51.7%. Five year survival of surgically resected stage I NSCLC was reported as 55–80%.1–5 Our result is lower than in most other reports. Possible reasons include long period of patient collection, surgery performed by different surgeons and variations in mediastinal lymph node dissection. The number of mediastinal lymph nodes dissected represents the quality of lymphadenectomy in patients with resected stage I NSCLC. The quality of lymphadenectomy has impact on a more accurate tumour staging and affects the survival rate for patients with stage I NSCLC significantly.10 11 The number of mediastinal lymph nodes dissected was 15 or less in 534 (57.2%) and more than 15 in 382 (41.0%) patients (unknown in 17 patients) in our study. For patients with more than 15 mediastinal lymph nodes dissected, 5 year survival reached 58.5%.
This study investigated the prognostic role of conventional clinicopathological factors on post-recurrence survival in patients with resected stage I NSCLC with local recurrence. Local recurrence after surgical resection was detected in 123 (13.2%) of the 933 patients. Median time to initial recurrence for these 123 patients was 15.2 months. The 1 and 2 year post-recurrence survival rates were 48.0% and 18.7%, respectively. For 74 patients with local only recurrence, the 1 and 2 year post-recurrence survival rates were 48.7% and 17.6%, respectively. Only treatment for initial recurrence was a significant predictor of post-recurrence survival in multivariate analyses.
Martini et al reported that the overall incidence of recurrence in patients with resected stage I NSCLC was 27% (local or regional 7%, systemic 20%).4 In the study of Harpole et al, the initial location of recurrence of stage I NSCLC after surgical resection was at a distant site in 19%, within the ipsilateral hemithorax in 11% or at both locations in 6% of patients.5 Our results demonstrated that the overall incidence of recurrence was 31.0% (distant only in 17.8%, local only in 7.9%, local and distant in 5.3%). The patterns of local recurrence included local only in 74 (60.2%), local with distant in 19 (15.4%), local before distant in 24 (19.5%) and distant before local in six (4.9%) patients. Approximately 78% of patients with local recurrence occurred within the first 2 years after operation. Furthermore, our study followed the course and reoperation after local recurrence. More than half of the patients (51.3%) died within 1 year after local only recurrence. The longest post-recurrence survival after local recurrence in our series was 15.8 years in a patient with stump recurrence who underwent reoperation.
Surgical resection offers a good chance of cure for patients with stage I NSCLC.1–5 However, the outcome of surgical treatment in resected stage I NSCLC after local recurrence has rarely been reported. Walsh et al reported that treatment with curative intent had significantly better overall survival and post-recurrence survival than treatment with palliative intent in patients with NSCLC.16 Sugimura et al demonstrated that surgery or combination chemotherapy with radiation significantly improved post-recurrence survival over both no treatment and radiation alone in resected NSCLC after recurrence.7 Voltolini et al reported that 5 year survival after reoperation for locally recurrent bronchogenic carcinoma was 15.5%.8 The 5 year post-recurrence survival in our patients undergoing reoperation after local recurrence was 15%. Our study further showed that surgical resection had a favourable survival in resected stage I NSCLC after local only recurrence (hazard ratio (HR) 0.089) than with chemotherapy and/or radiotherapy (HR 0.326) and with no treatment (HR 1.0, reference; p = 0.001). Eight of 16 patients had no treatment for recurrence because of poor performance status. This may be a contributory factor to poor prognosis.
Recently, local and regional nodal recurrences were not considered the cause of significant cancer cell dissemination, distant metastases or death.17 18 Rather, they are thought to be indicators of poor prognosis but not determinants of survival. Many studies have shown that better local control increases survival in some cancers.18–23 On the other hand, distant metastasis represents dissemination of cancer cells in distant organs and has significant impact on survival.18 24 Our study showed that patients who underwent complete resection for local only recurrence survived longer than those who received chemotherapy and/or radiotherapy and those who received no treatment. However, post-recurrence survival in patients with local only recurrence was not significantly different from those with both local and distant recurrences in our study. The seventh edition of the TNM Classification of Malignant Tumours is scheduled to be published in 2009. For lung cancer, some studies propose that pleural effusion be moved from T4 to M1a.25–27 Our results showed that post-recurrence survival in patients with pleural effusion as part of the local only recurrence was not significantly different from that in those without pleural effusion (p = 0.432).
Treatment for recurrence is a prognostic predictor for post-recurrence survival in resected stage I NSCLC with local recurrence. Complete surgical resection should be considered in selected candidates with resectable recurrent disease.
Acknowledgments
The authors are grateful to Drs Liang-Shun Wang of En Chu Kong Hospital and Wen-Juei Jeng of Chang Gung Memorial Hospital for their contribution to this article. They also thank Mr Jung-Hsing Lin for his assistance in data collection.
REFERENCES
Supplementary materials
web only appendix 64/3/192
Files in this Data Supplement:
Footnotes
See Editorial, p 185
A supplementary table is published online only at http://thorax.bmj.com/content/vol64/issue3
Competing interests: None.
Linked Articles
- Airwaves
- Editorial